
Allergic Rhinitis – Diagnosis and management ACG
Last updated 9 June 2026
Published on 15 May 2026
Overview
This ACE Clinical Guideline (ACG) provides evidence-based recommendations on the diagnosis and management of perennial allergic rhinitis. Specifically, guidance is provided on the diagnostic criteria for allergic rhinitis, clinical indications for allergy testing, considerations when selecting pharmacological therapy, and use of allergen avoidance strategies.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Diagnose allergic rhinitis based on the patient’s history, particularly their symptoms, combined with a physical examination.
Conduct allergy testing only when clinically warranted, for example when diagnosis is unclear, or when optimised pharmacotherapy provides inadequate symptom control.
Prescribe intranasal corticosteroid, oral antihistamine (2nd generation or later), or combination intranasal corticosteroid and intranasal antihistamine to manage allergic rhinitis.
Offer allergen avoidance advice to all patients with allergic rhinitis as an adjunct to pharmacological therapy, focusing on accessible and practical strategies.
Download the ACG, reference and EG composition
Download the ACG, reference and EG composition
Allergic rhinitis – diagnosis and management (May 2026) [PDF]
Allergic rhinitis – diagnosis and management references (May 2026) [PDF]
Allergic rhinitis ACG EG composition and other details (May 2026) [PDF]
ACG EtR framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values, acceptability and other considerations.
Allergic Rhinitis ACG EtR framework with summary of findings (May 2026) [PDF]
Request for a hard copy
Click here
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
The prevalence of allergic rhinitis (AR) is estimated to be more than 30% in Singapore,1,2 with most cases observed in the paediatric and young adult population.3 It is commonly perceived as a benign and self-limiting condition, leading to symptom normalisation, reliance on intermittent self-treatment, and delays in seeking care.4 While AR is not associated with severe outcomes, a recent local study found that approximately 85% of AR cases are undiagnosed and 73% untreated, where most had moderate-to-severe disease. Moreover, poorly controlled or untreated AR can lead to complications such as asthma, sinusitis, or otitis media with effusion. Therefore, these findings highlight a hidden disease burden among individuals with AR despite the availability of effective therapies.
AR is classified into perennial and seasonal forms. In Singapore’s warm, humid climate, perennial AR predominates and is mainly driven by indoor allergens,5 particularly house dust mites (HDM). Over 80% of the local population is sensitised to HDM,6 primarily Dermatophagoides pteronyssinus, Dermatophagoides farinae, and Blomia tropicalis, with mite droppings being the main trigger of symptoms. Seasonal AR, usually related to pollen that appear seasonally, is uncommon in Singapore and is therefore out of scope for this guideline.5
This ACE Clinical Guideline (ACG) emphasises that AR is a chronic condition which requires regular assessment and a planned approach to treatment, rather than episodic symptom relief. It provides evidence-based recommendations for the diagnosis and management of AR in the primary and generalist care setting.
Diagnosis
Recommendation 1: Diagnose allergic rhinitis based on the patient’s history, particularly their symptoms, combined with a physical examination.
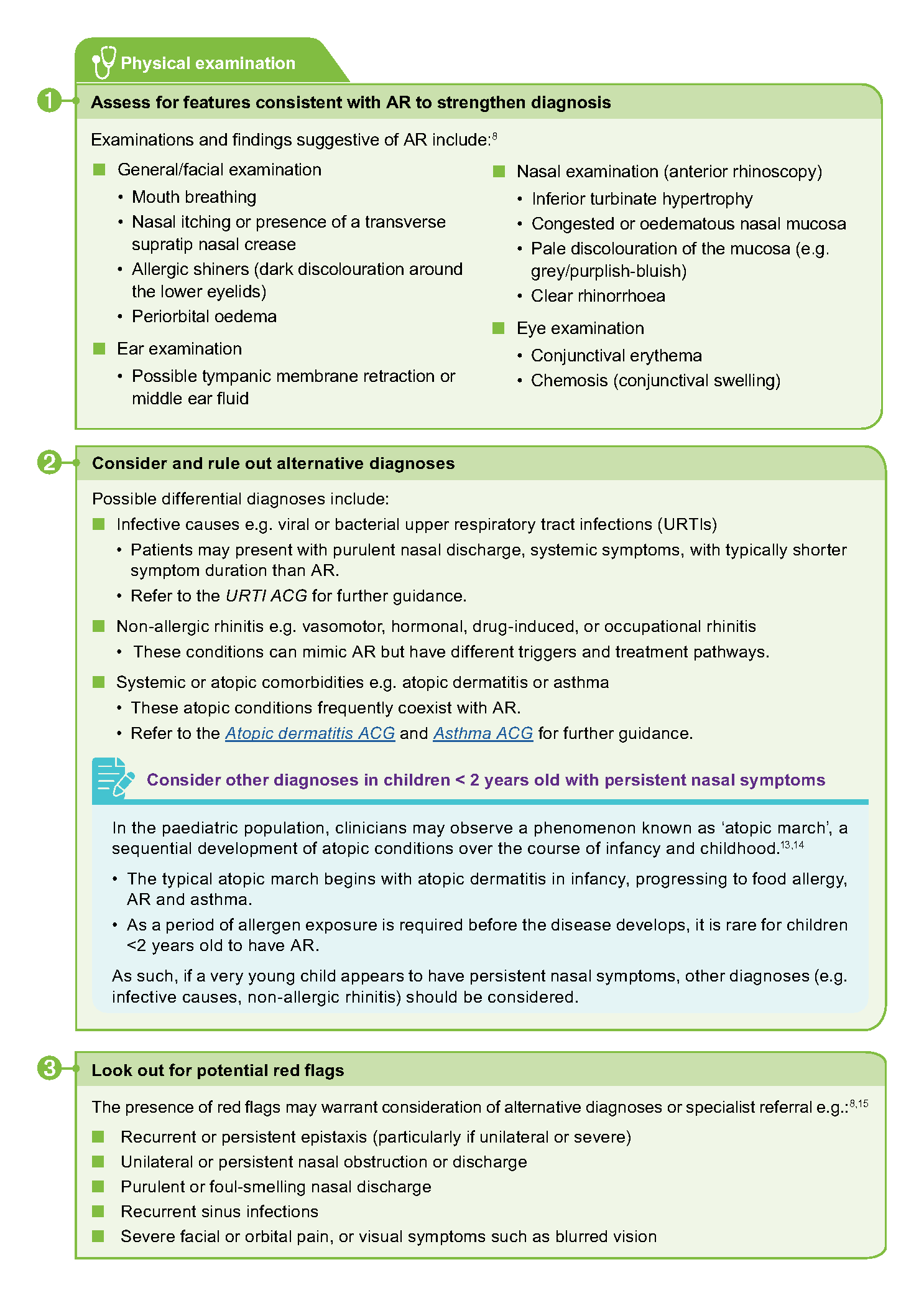
For most patients, a combination of patient history and physical examination are required, and in themselves sufficient, to maximise the likelihood of a correct AR diagnosis (Figure 1).7
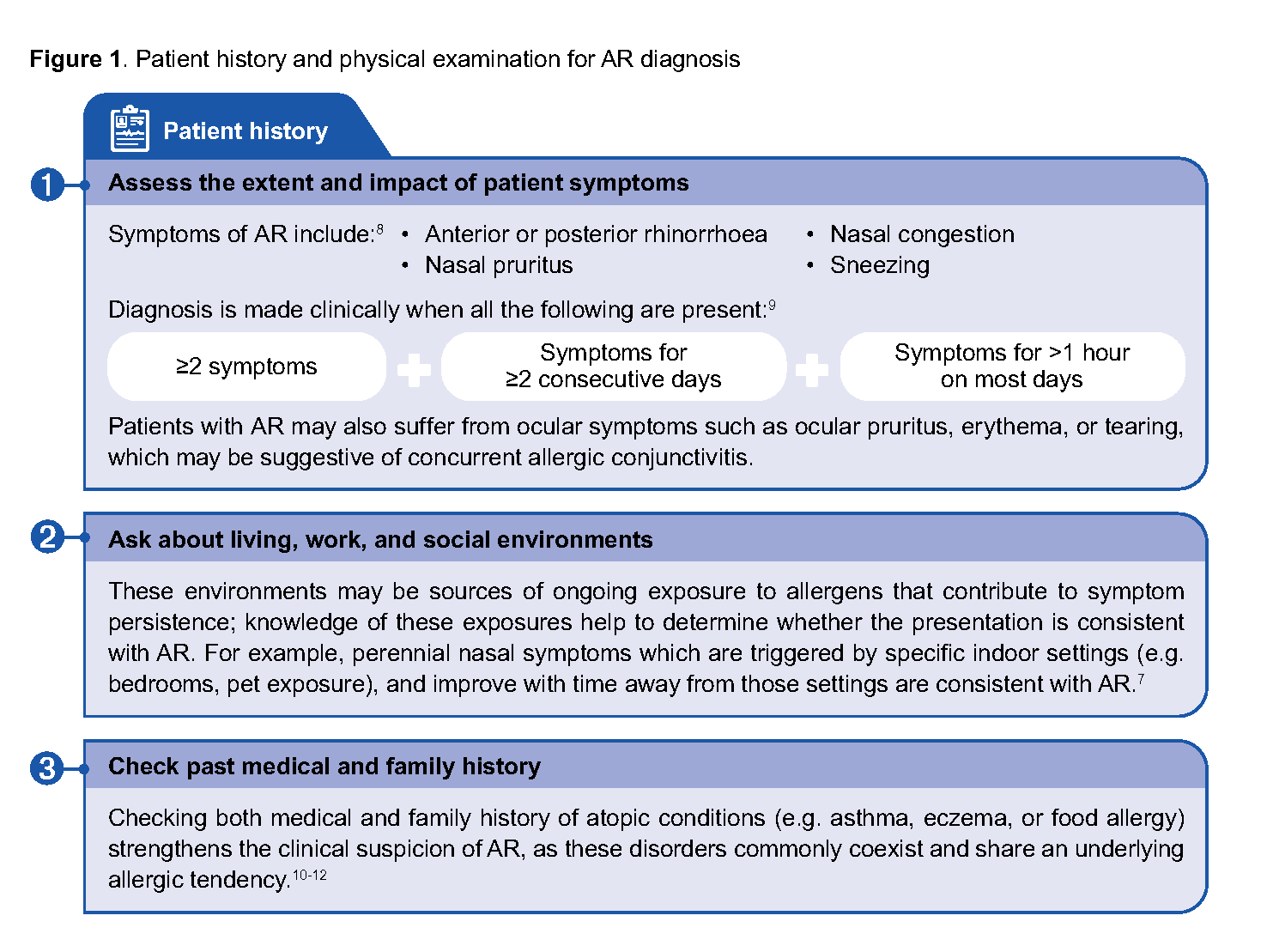
Figure 1. Patient history and physical examination for AR diagnosis
Following diagnosis, AR is classified based on the frequency and severity of symptoms:15
Frequency
Intermittent – symptoms <4 days/week or <4 consecutive weeks
Persistent – symptoms ≥4 days/week and ≥4 consecutive weeks
Severity
Mild – symptoms not troublesome and not affecting quality of life (QoL)
Moderate-severe – symptoms affecting QoL, through ≥1 of the following:
- Sleep disturbance
- Impaired daily activity, leisure or sport
- Impaired school or work attendance and performance
While there is no single definitive symptom scale for AR, validated symptom severity or control tools such as the Visual Analog Scale (VAS) may be helpful to establish a baseline level of symptom severity.16 These tools can then be used to monitor ongoing symptom control and inform treatment adjustments.
Notepad: Telemedicine and AR As a physical examination cannot be conducted via telemedicine, clinicians should use teleconsultations judiciously and refer to prevailing MOH telemedicine guidelines. In-person assessment is recommended when red flags or diagnostic uncertainty are present. |
Notepad: Considering nasal endoscopy when AR diagnosis remains unclear Nasal endoscopy provides a direct visualisation of the entire nasal cavity. A specialist referral for nasal endoscopy may be considered when structural abnormalities or alternative diagnoses to AR are suspected (e.g. nasal polyps, deviated septum, adenoid hypertrophy, unilateral obstruction, or purulent nasal discharge) |
Role of allergy testing
Recommendation 2: Conduct allergy testing only when clinically warranted, for example when diagnosis is unclear, or when optimised pharmacotherapy provides inadequate symptom control.
Allergy testing is not routinely required for AR diagnosis and management.17 However, it may be helpful in certain situations, for example where:
There is diagnostic uncertainty despite a thorough patient history and physical examination5
AR symptoms persist and/or remain severe despite optimised pharmacotherapy7
Allergens need to be identified to enable allergen-specific avoidance measures7
Allergen immunotherapy is being considered7
The patient presents with multiple atopic conditions18
Both skin prick test (SPT) and serum-specific immunoglobulin E (sIgE) detect sensitisation rather than clinical allergy, and should be interpreted alongside the patient’s history, exposure, and symptom patterns. Key considerations to guide appropriate test selection are summarised in Table 1 below.
Table 1. Comparison between SPT and sIgE blood test
Attribute | Skin prick test (SPT) | Serum-specific immunoglobulin E (sIgE) blood test |
|---|---|---|
What it measures | Immediate IgE-mediated skin reactivity to allergen extracts | Circulating allergen-specific IgE antibodies from a blood sample |
Diagnostic performance | Sensitivity and specificity greater than 80% for common aeroallergen19-22 | Sensitivity of 67-96% and specificity of 80-100%; may detect low-level sensitisation of uncertain clinical relevance7 |
Time to results | 15–20 minutes | Several days (typically) |
Cost and resource requirements | Lower cost per allergen; requires clinic-based facilities and consumables Requires trained personnel and allergen extracts | Higher cost than SPT; also dependent on laboratory equipment and reagents Requires blood draw and laboratory processing |
Patient suitability | SPT is not suitable for:
May be a preferred test for younger children due to less discomfort compared to a blood test | Preferred alternative when SPT is contraindicated or impractical |
Safety considerations | Very rare risk of systemic allergic reactions | No risk of provoking allergic reactions |
Example of appropriate indication | When rapid results or targeted panel testing in one sitting is useful | When antihistamines cannot be discontinued or when existing skin disease affects suitability for SPT |
Broad testing of allergens is not routinely necessary in Singapore as house dust mites (HDM) are the predominant allergen. Other less common allergens include mould spores (in damp or poorly ventilated areas), pet dander and perennial pollens (e.g. oil palm pollen). Testing for these should only occur if suggested by patient history.5
Non-allergenic irritants such as tobacco smoke are recognised triggers that may exacerbate AR symptoms but are not detectable through allergy testing; their identifcation relies on clinical history and exposure assessment
Management – pharmacotherapy
Recommendation 3: Prescribe intranasal corticosteroid, oral antihistamine (2nd generation or later), or combination intranasal corticosteroid and intranasal antihistamine to manage allergic rhinitis.
Pharmacotherapy plays a crucial role in AR management due to its effectiveness in achieving symptomatic control and improving patients’ daily functioning, sleep, and QoL.
Three classes of medications are recommended as initial treatment options:
Intranasal corticosteroids (INCS)
Oral antihistamines (OAH) – 2nd generation or later
Combination intranasal corticosteroid and intranasal antihistamine (INCS+INAH)
While these options differ in efficacy and onset of action, ultimately, patient preferences, tolerability, and access should guide the choice of initial treatment23 (Table 2).
Pharmacotherapy should be continued until symptoms resolve, after which treatment review and step-down can be considered. If AR symptoms recur, pharmacotherapy should be restarted on the previous most effective dose.
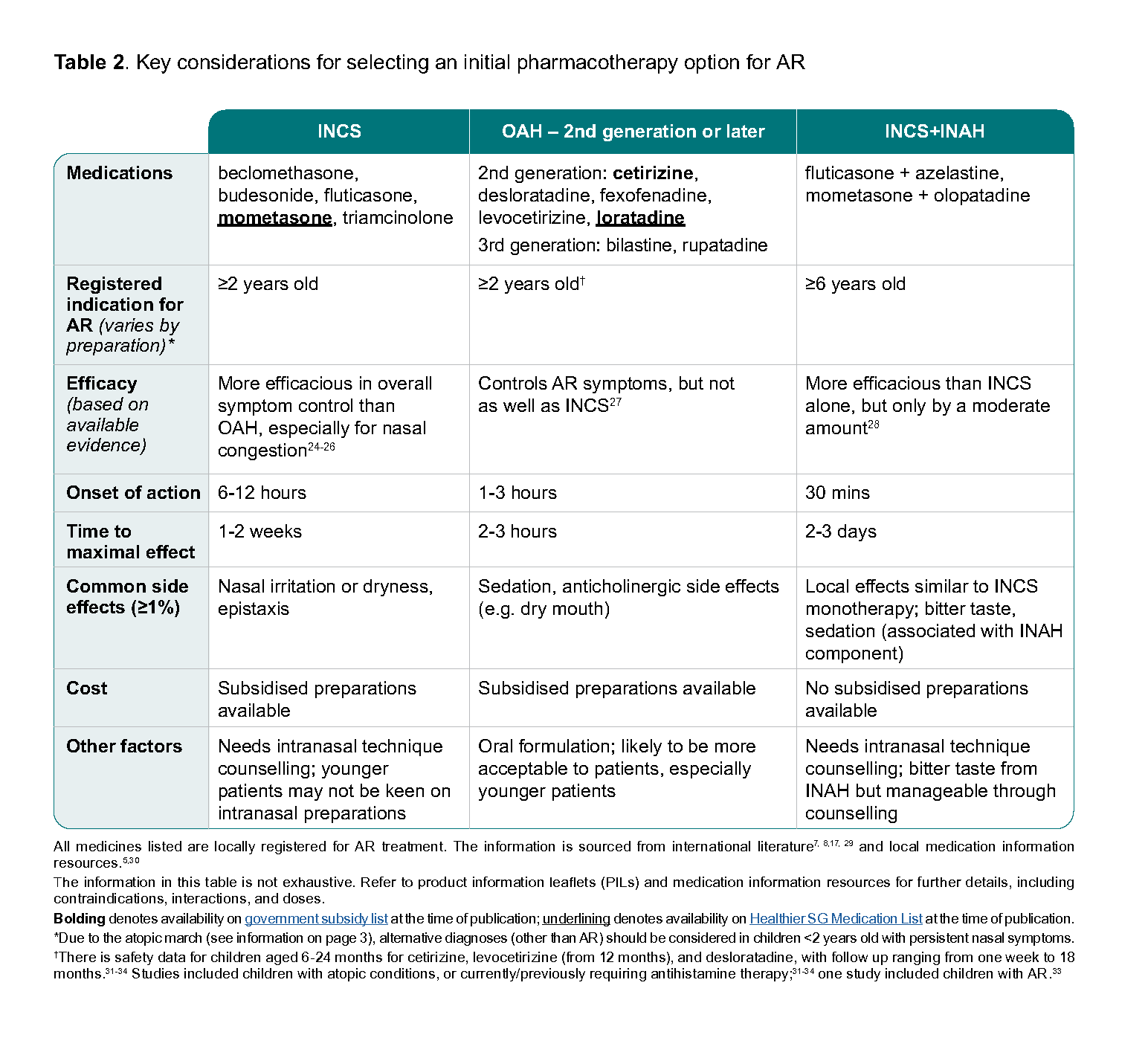
Table 2. Key considerations for selecting an initial pharmacotherapy option for AR
Intranasal corticosteroids
The INCSs provide effective AR symptom control, including for nasal congestion, rhinorrhoea, sneezing, sleep disturbance, and improve QoL.7 Their safety profile is well established when used at recommended doses, and they are widely used in the long-term management of AR. For information on INCS dosages, refer to their accompanying product information leaflets (PILs) for details on starting doses and dosing adjustments.
Oral antihistamines
Second-generation (and later) OAH provide effective symptom control with generally acceptable safety profile and are widely available as over-the-counter medications.7 OAHs have faster onset than INCSs, although the latter are more effective in addressing nasal congestion.27 First-generation oral antihistamines (e.g. chlorpheniramine, hydroxyzine, ketotifen and promethazine) are not recommended for the treatment of AR because of their central nervous system and anticholinergic side effects.
Intranasal corticosteroid and intranasal antihistamine combination
INCS+INAH combinations demonstrate the greatest efficacy and most rapid onset of action compared to INCS or OAH monotherapy.28 INCS+INAH are effective in improving nasal symptoms, ocular symptoms and QoL. For patients with AR on INCS monotherapy, INCS+INAH combination is often recommended as a step-up option. However, their uptake may be limited by their bitter aftertaste and higher cost.
Notepad: Switching between treatment options If initial treatment options remain insuffcient in achieving adequate symptom control despite optimal adherence, clinicians may consider switching to a different medication.35 For example:
The decision to switch and what medication to use is guided by similar considerations applied to the initial treatment decision, such as patient preferences, tolerability, and access. |
Notepad: Other oral treatments for AR Leukotriene receptor antagonists (LTRAs) provide inferior symptom control compared with the recommended frst-line therapies for AR.7 However, they may be considered as a treatment option for AR in patients with concomitant asthma, either as an alternative to frst-line therapies if they are contraindicated, or as an adjunct to INCS.7 Montelukast, an LTRA, is associated with a serious but rare risk of neuropsychiatric adverse effects.35 If prescribing montelukast is unavoidable, review the HSA advisory and follow the recommended risk mitigation principles, including appropriately counselling the patient. Oral corticosteroids also have unfavourable safety profiles if used long term, and lack additional benefit compared with the initial treatment options listed above for AR symptom management.7 Oral decongestant monotherapy lacks effectiveness for AR symptom relief other than nasal congestion and is associated with increased risk of adverse effects.7 However, when combined with OAH for a short term, the combination provides AR symptom relief, including for rhinorrhoea, nasal congestion, nasal itching, and sneezing.7 Chronic use of oral decongestants are not recommended due to an increased risk of adverse effects (e.g. insomnia, headache, nervousness). |
Enhancing treatment effectiveness in AR
Suboptimal disease control in AR is commonly observed, driven by poor treatment acceptance and adherence, together with limited understanding of the condition.13 Therefore, targeted patient education and counselling would improve acceptance of steroid-containing intranasal therapies and the correct intranasal technique.
Improving patient acceptance of steroid-containing preparations
Several barriers can impede the use of steroid-containing preparations, including safety concerns and undesirable sensations associated with intranasal administration.37 To support patient confdence, remind patients that these intranasal preparations have good safety profles which have been established through evidence, are safer than oral corticosteroids, and rarely cause serious side effects, with most local side effects manageable through correct technique.
Intranasal technique counselling
Counsel on correct intranasal spray technique to optimise treatment outcomes, as suboptimal technique may lead to reduced effectiveness, local side effects (e.g. nasal irritation) or unnecessary dose escalation.8
Proper technique includes ensuring appropriate head position, contralateral hand use, and angling the nozzle away from the septum. Patients can be directed to the medication PILs for detailed steps.
Notepad: Use of digital tools to support AR management Digital tools, such as reminder systems, treatment trackers or monitoring applications, can serve as enablers to support adherence and AR symptom management.38 These tools have the potential to help patients with AR recognise if their symptoms are worsening, adjust their actions accordingly or seek care. |
Additional treatment options
In patients with AR who have persistent symptoms despite initial therapy, adjunct treatment options may be added to improve symptom control (see Table 3).
Table 3. Additional treatment options for AR
Treatment‡ | Summary |
Intranasal saline |
|
Intranasal decongestants |
|
‡Intranasal anticholinergics have been shown to reduce the duration and severity of rhinorrhoea, and can be used together with INCS or OAH if rhinorrhoea persists.8 However, products are not yet registered by the Health Sciences Authority and hence not available in primary care.
Considerations for specialist referral
If symptoms persist or remain severe despite optimised pharmacotherapy, clinicians should consider referring to a specialist for further evaluation and management, particularly if:
AR significantly impacts QoL, including sleep disturbance or impaired school or work performance
The patient has relevant comorbidities, such as poorly controlled asthma, chronic rhinosinusitis, suspected nasal polyposis, septal or nasal deviation
Specialist assessment may include re-evaluation of the AR diagnosis, additional investigations where appropriate, and consideration of allergen immunotherapy when indicated.
Management – allergen avoidance
Recommendation 4: Offer allergen avoidance advice to all patients with allergic rhinitis as an adjunct to pharmacological therapy, focusing on accessible and practical strategies.
Allergen avoidance refers to measures aimed at reducing exposure to allergens that trigger or exacerbate AR symptoms, e.g. HDM or other environmental allergens. For HDM, current evidence is based on international studies and is of low quality, with studies showing limited usefulness of allergen avoidance in improving AR symptoms.28 However, recognising its practicality, allergen avoidance is recommended as an adjunct to pharmacological therapy. Clinicians should focus on low-risk and accessible strategies for patients, prioritising child-friendly approaches for paediatric patients.
For HDM allergy, no single HDM avoidance method is superior.41 Therefore, allergen avoidance should be individualised, considering patient preference, feasibility within the home or work environment, and overall acceptability. While complete HDM elimination is not feasible, exposure can be reduced through practical measures, e.g.:
Encasing mattresses, pillows and bolsters with HDM-proof covers13
Washing bedding frequently, preferably in hot water (above 60°C)13
Removing rugs or carpets13
Minimising additional soft items on the bed (e.g. stuffed toys, cushions) that can collect dust
Avoiding agitation of dust to reduce allergen exposure
Beyond HDM, other less commonly encountered indoor allergens may also warrant allergen-specific environmental interventions, if sensitisation and clinically relevant exposure is identified.These interventions can be included as part of a broader AR management plan but should complement and not replace pharmacological treatment.
Expert group
Chairpersons
Clin Assoc Prof Charn Tze Choong, Ear, Nose & Throat (SKH)
Dr Tan Wee Hian, Family Medicine (NUP)
Members
Dr Chang Zi Ying, Family Medicine (Sengkang Polyclinic)
Dr Cheng Yew Kuang, Rheumatology, Allergy, and Immunology (Arthritis & Rheumatism Clinic)
Dr Elaine Chua, Family Medicine (Bedok Medical Centre)
Dr Ding Si Yan, Family Medicine (Hougang Polyclinic)
Clin Prof Anne Goh Eng Neo, Paediatrics, Allergy, and Immunology (KKH)
Dr Gui Huey Sywu, Pharmacist (Geylang Polyclinic)
Dr Suraj Kumar, Family Medicine (Drs Bain & Partners)
Adj Prof Lee Bee Wah, Paediatrics, Allergy and Immunology (NUS)
Adj Assoc Prof Ng Chew Lip, Ear, Nose & Throat (NTFGH)
Clin Assoc Prof Siow Jin Keat, Ear, Nose & Throat (TTSH)
Dr Tan Wei Lynn Justina, Rheumatology, Allergy, and Immunology (TTSH)
Mr Teo Yi Liang, Pharmacist (Guardian)
Dr Tham Chengyao Alex, Ear, Nose & Throat (Asian Healthcare Specialists Alvernia)
Dr Nelson Wee, Family Medicine (Silver Cross Medical)
Prof Hugo Van Bever, Paediatrics, Division of Rheumatology, Allergy and Immunology (NUH)
For more information on the Expert Group composition and other details, click here.