
Asthma — optimising long-term management with inhaled corticosteroid ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) covers clinical assessment, pharmacological treatment, and non-pharmacological strategies for managing asthma over the long term, with a focus on inhaled corticosteroid as the mainstay. The accompanying Appendix provides a list of preventer medications registered for asthma in Singapore.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Regularly assess asthma symptoms and risk of poor asthma outcomes, including factors that can influence these.
Consider using a validated questionnaire to assess asthma symptoms.
Assess factors influencing asthma symptoms or risk of poor asthma outcomes. These can be remembered with the acronym BREATHE.
Use inhaled corticosteroid as the mainstay of long-term asthma management.
For patients aged 6 years and older, do not use short-acting beta2agonist alone (without a preventer) to treat asthma long term.
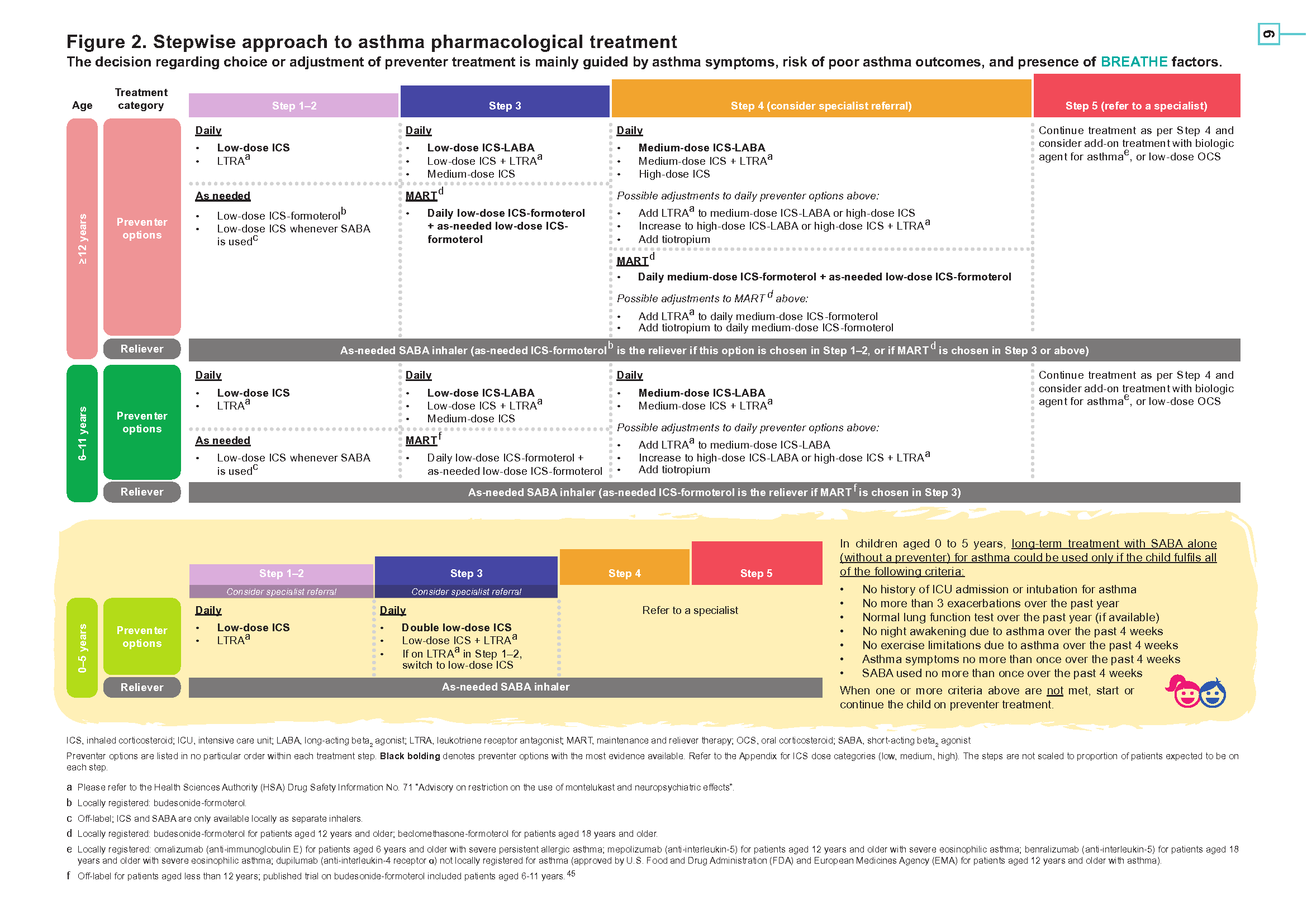
Use a stepwise approach when selecting or adjusting preventer treatment for asthma (see Figure 2 on page 6).
Educate all patients with asthma or their caregivers on how to self-manage.
Regularly follow up all patients with asthma.
Referral to a specialist could be made at any point.
Download the ACG and reference in PDF
Asthma Management - Optimising long-term management with inhaled corticosteroids (Oct 2020) [PDF]
Asthma Management Appendix (Oct 2020) [PDF]
Asthma Management References (Oct 2020) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Asthma is one of the most common chronic respiratory conditions seen in primary care in Singapore.1 Around 5% of residents in Singapore aged 18 to 69 years have asthma.2 About 1 in 3 patients with asthma aged 12 years and older in Singapore report exacerbations in the past year, and about 1 in 2 have missed work or school due to asthma in the past year.3 The impact of asthma locally is also reflected in hospital admissions, with Singapore’s asthma hospital admission rates being higher than countries in the Organisation for Economic Co-operation and Development (OECD).4
Risk of exacerbations and other poor asthma outcomes, such as hospital admissions, can be reduced with preventer (or controller) medications, particularly inhaled corticosteroid (ICS)─the mainstay of long-term asthma management.5-8 Despite wide availability of ICS, use of preventers in Singapore is the lowest among eight countries in the Asia-Pacific region, with only 1 in 4 patients with asthma aged 12 years and older using a preventer in the past month.3 Locally, one third of patients with a severe asthma exacerbation requiring mechanical ventilation or intensive care unit (ICU) admission were not on ICS prior to the exacerbation.9
To reduce the impact of asthma in Singapore, more optimal ICS use as part of long-term management is needed.
Management goal for asthma
Although asthma is a chronic condition, it typically manifests as episodic symptoms with variable expiratory airflow limitation. Asthma symptoms include shortness of breath, cough, wheeze, and chest tightness, which tend to vary over time in frequency or intensity.10,11
The underlying pathophysiology of asthma is characterised by chronic airway inflammation, rendering the airways more susceptible to a variety of stimuli that may trigger bronchoconstriction (hyper-responsiveness), leading to asthma symptoms. However, the degree of chronic airway inflammation does not always correlate with the extent of symptoms.12,13
Without adequate long-term management, asthma may result in poor outcomes including exacerbations,* hospital admissions, fixed airflow limitation, and in some cases, even death. The management goal for asthma is to prevent or minimise symptoms and reduce risk of poor outcomes.5,10,11
To achieve the management goal, this heterogeneous condition should be addressed in totality, including comprehensive clinical assessment and personalised management.
Asthma assessment
Recommendation 1: Regularly assess asthma symptoms and risk of poor asthma outcomes, including factors that can influence these.
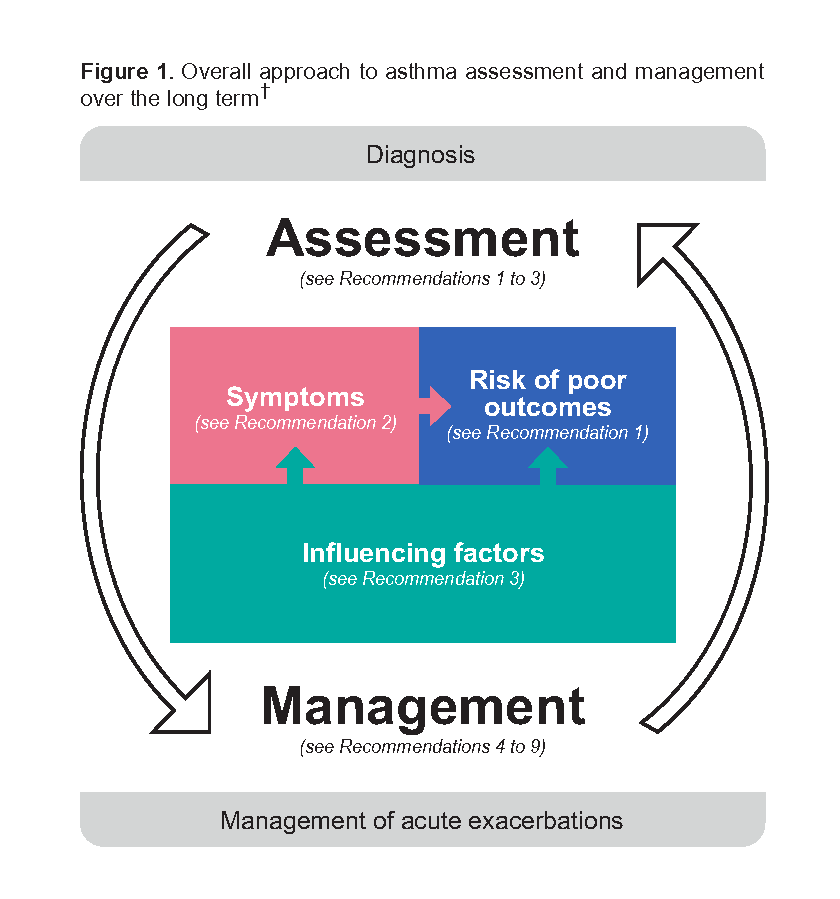
Asthma assessment over the long term is to evaluate the patient in relation to the management goal, and therefore encompasses assessment of both symptoms and risk of poor outcomes (see Figure 1).
While more frequent or intense asthma symptoms are associated with higher risk of poor asthma outcomes (including exacerbations and hospital admissions), such risk may still exist even if the patient reports minimal symptoms.14,15 Factors other than symptoms that can affect risk of poor asthma outcomes include adherence to treatment, inhaler technique, lung function, and relevant comorbidities. Some of these factors can also worsen asthma symptoms (see Figure 1).
Consequently, symptoms as well as factors known to influence symptoms or risk of poor outcomes (influencing factors) should be assessed.
Recommendation 2 and Recommendation 3 provide more details on assessing asthma symptoms and influencing factors, to better determine risk of poor asthma outcomes and hence the patient’s overall status in relation to the management goal, for guiding management decisions.
* Exacerbations refer to worsening of asthma symptoms beyond those typically experienced by the patient, sometimes requiring urgent actions, including unscheduled clinic visits, use of oral corticosteroid, emergency department visits, and hospital admissions. Asthma exacerbations may lead to mortality in some cases.
†Grey boxes denote areas outside the scope of this clinical guidance.
Recommendation 2: Consider using a validated questionnaire to assess asthma symptoms.
Aspects of asthma symptom assessment include:
Frequency and intensity of daytime and night-time symptoms
Frequency of reliever use for symptom relief (excluding pre-exercise use for symptom prevention)
Ability to carry out daily activities
In addition to broad questions such as “How is your asthma?”, use specific questions like “Over the past four weeks, how many times did you have asthma symptoms at night?”. Specific questions are often used in validated questionnaires‡ for asthma symptom assessment.
Examples of such questionnaires‡ include the Asthma Control Questionnaire (ACQ),17 the Asthma Control Test (ACT),18 the Royal College of Physicians Three Questions,19,20 the Pharmacy Asthma Control Screening Tool,21 and the Childhood Asthma Control Test (C-ACT) for patients aged 4 to 11 years.22
Consider reviewing asthma management when symptoms are frequent (for example, an average of more than twice a week), when they affect the patient’s ability to carry out daily activities or rest at night, or when there is a change in usual number or intensity of symptoms.
Notepad: Peak expiratory flow (PEF) PEF is a simple, self-administered objective measure of expiratory airflow limitation. Consider PEF for patients prone to underperceiving symptoms (such as adolescents, patients who have comorbidities with symptoms similar to asthma, elderly patients), or those likely to overperceive them (such as anxious patients).16 |
When choosing an asthma symptom assessment questionnaire‡ for children aged 0 to 5 years, select one developed especially for this age group or their caregivers, such as the Test for Respiratory and Asthma Control in Kids (TRACK).23-25 |
Recommendation 3: Assess factors influencing asthma symptoms or risk of poor asthma outcomes. These can be remembered with the acronym BREATHE.
Several factors are known to worsen asthma symptoms or risk of poor asthma outcomes. The BREATHE acronym below is an easy and comprehensive way to remember these influencing factors.
Table 1. BREATHE factors for asthma assessment
Beliefs, knowledge, and attitudes Assess possible misconceptions about asthma and its management, including understanding of asthma as a chronic condition, the management goal, and role of preventers and relievers.26 |
Recent asthma treatment Identify patients with suboptimal treatment, such as those not on ICS or those using SABA often.9,27 |
Effects of asthma Assess extent of asthma effects, including current effects such as reduced quality of life or productivity, and past effects such as an exacerbation over the past year, or history of intubation or admission to ICU for asthma.28 |
Adherence Assess extent of asthma effects, including current effects such as reduced quality of life or productivity, and past effects such as an exacerbation over the past year, or history of intubation or admission to ICU for asthma.28 |
Triggers Evaluate asthma triggers (for example, dust or occupational exposures) to identify those potentially avoidable, such as cigarette smoking.26,30 |
History of asthma Review initial diagnosis (if needed) and the course of disease, including lung function and other relevant test findings (for example, FEV1 , FEV1 /FVC, or inflammatory biomarker levels), especially for patients in whom asthma symptoms persist or worsen despite appropriate management. |
Existing comorbidities or medications Assess presence of comorbidities relevant for asthma, such as rhinitis, rhinosinusitis, obesity, obstructive sleep apnoea, GORD, asthma-COPD overlap, or mental health disorders.10 Also assess for medication interactions. |
COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in first second; FVC, forced vital capacity; GORD, gastro-oesophageal reflux disease; ICS, inhaled corticosteroid; ICU, intensive care unit; SABA, short-acting beta2 agonist
‡Some of these questionnaires are protected by copyright and require a licensing fee to use.
Some of the factors captured in BREATHE are associated with more severe asthma outcomes (such as severe exacerbations or mortality). Listed in Table 2 below are such factors that can be readily assessed clinically.
Table 2. Risk factors for more severe asthma outcomes that can be readily assessed clinically
Consider prioritising these when assessing factors influencing asthma symptoms or risk of poor asthma outcomes: |
|---|
|
|
|
|
|
ICS, inhaled corticosteroid; ICU, intensive care unit; SABA, short-acting beta2 agonist
Asthma management
Long-term asthma management involves personalising both pharmacological treatment and non-pharmacological strategies according to the patient’s needs as reflected in the assessment findings. In particular, it targets chronic airway inflammation and BREATHE factors where applicable, to achieve the management goal of preventing or minimising symptoms and reducing risk of poor outcomes.
In addition to management strategies outlined in this section, offer influenza and pneumococcal vaccination to patients with asthma, consistent with the National Adult Immunisation Schedule and the National Childhood Immunisation Schedule.31,32
Pharmacological treatment
Pharmacological treatment for asthma encompasses preventers and relievers.
Recommendation 4: Use inhaled corticosteroid as the mainstay of long-term asthma management.
Inhaled corticosteroid (ICS) addresses airway inflammation and is the most effective treatment to achieve the management goal for asthma. It reduces poor asthma outcomes in the long term, including exacerbations and mortality.33–36 Benefits of ICS have been observed at low doses even in patients with infrequent or minor asthma symptoms.37
Some patients or caregivers may be reluctant to use ICS as they believe it may result in adverse effects similar to those with oral corticosteroid (OCS). Proactively address this misconception and educate them regarding risk of adverse effects with ICS, which is much lower than with OCS. Consider the following general suggestions and measures to minimise risk of adverse effects associated with ICS:
Optimise inhaler technique to minimise systemic medication absorption
Advise patients to rinse their mouth after ICS use and to use a spacer if appropriate, to reduce topical adverse effects
Use the lowest effective ICS dose. If treatment needs to be increased, consider adding another agent, such as a long-acting beta2 agonist (LABA) or a leukotriene receptor antagonist (LTRA), rather than increasing the ICS dose. If not possible to avoid long-term daily high-dose ICS, monitor patients closely for adverse effects and consider specialist referral
Recommendation 5: For patients aged 6 years and older, do not use short-acting beta alone (without a preventer) to treat asthma long term.
Short-acting beta2 agonist (SABA) does not address airway inflammation. Compared to patients using an ICS-containing treatment as the preventer with SABA as the reliever, those relying on SABA alone (without a preventer) are more likely to experience poor asthma outcomes, such as need for OCS, emergency department visits, or hospital admissions.38,39
Notepad: Important change in asthma management The recommendation not to use SABA alone (without a preventer) for the long-term treatment of patients aged 6 years and older, even those with infrequent or minor symptoms, is the most significant change in asthma management recently. SABA is still recommended for short-term relief of symptoms as needed (see Figure 2 on page 6). |
Recommendation 6: Use a stepwise approach when selecting or adjusting preventer treatment for asthma (see Figure 2 on page 6).
A patient with well-managed asthma would, ideally, have no symptoms. While this may not always be feasible, long-term asthma management, including pharmacological treatment, should be aimed at preventing symptoms from occurring. Preventer treatment does so by addressing chronic airway inflammation. The decision regarding choice or adjustment of preventer treatment is mainly guided by asthma symptoms, risk of poor asthma outcomes, and presence of BREATHE factors. As part of the decision-making, practical considerations include the patient's ability to use the inhaler correctly, concerns about using ICS, and inhaler cost. Preventers registered for asthma in Singapore are listed in the Appendix.
Across the asthma treatment steps overall (see Figure 2 on page 6), daily ICS-containing treatment is the most effective preventer option at preventing or minimising asthma symptoms, and has the most evidence available─including long-term benefits on exacerbations and mortality.40,41 Daily ICS-containing treatment is particularly important for patients at higher risk of poor asthma outcomes (for example, those with frequent or intense symptoms, or those with multiple BREATHE factors, as described in Recommendation 2 and Recommendation 3).
Depending on individual patient circumstances, including treatment adherence, as-needed ICS-containing treatment could be a suitable option in Step 1–2. However, reliance on a solely symptom-driven approach may limit the achievement of the management goal for asthma, and may render adjustment to daily treatment more difficult if this is required.
STARTING PREVENTER TREATMENT ICS-naïve patients usually respond well to initial ICS treatment with daily low-dose ICS. A higher step could be used for initial treatment as necessary, for example for patients with frequent or intense symptoms, those who had an exacerbation over the past year, those with relevant comorbidities, or smokers.42 |
STEPPING UP Consider stepping up the preventer treatment for patients who still have frequent or intense symptoms, and based on risk of poor outcomes (especially if particular BREATHE factors are present, such as an exacerbation over the past year), after assessing adherence and inhaler technique. Options for stepping up within the same step or by moving up steps include:
|
STEPPING DOWN Consider gradually stepping down the preventer treatment to the lowest effective dose once symptoms are well managed for at least 3 to 6 months, and based on risk of poor outcomes, including choice of a suitable time for stepping down (for example, not stepping down in times of higher exacerbation risk such as during illness, allergy season, pregnancy, period of travel or high stress). Options for stepping down include:
|
For patients diagnosed with asthma aged 6 years and older, stopping ICS altogether is not recommended as this is associated with increased risk of exacerbations.43 Discuss with the patient or caregiver potential benefits and risks of adjusting the preventer treatment. Monitor patients closely after any treatment change. If asthma worsens after stepping down, resume the previous dose. If the patient’s condition is not improving after stepping up, consider other management options─including specialist referral.
Regularly assess children aged 0 to 5 years to evaluate the need for ongoing ICS. Consider discontinuing ICS when appropriate (see Figure 2 on page 6), and monitor these patients closely.44
Click here for larger version of the image
Patient education
Recommendation 7: Educate all patients with asthma or their caregivers on how to self-manage.
Asthma patient education addresses some of the BREATHE factors, and has been shown to reduce asthma-related days off work or school, unscheduled clinic visits, emergency department visits, and hospital admissions.46,47 It also improves quality of life in patients with asthma.46 Although usually delivered at diagnosis, consider reinforcing some or all key components of asthma patient education (see Figure 3 below) as informed by findings of asthma assessment or when adjusting preventer treatment.
Figure 3. Key components of asthma patient education
Share information on:
|
Teach how to:
|
Emphasise the importance of adherence to:
|
Provide a written asthma action plan to all patients |
An individualised written asthma action plan (WAAP) includes details of the patient’s usual asthma medications, as well as instructions on how to recognise worsening asthma and actions to take in case this happens (including actions in addition to reliever use, such as increasing the ICS dose, using OCS, or getting emergency help).48
Discuss non-pharmacological aspects of asthma management as appropriate. These include smoking cessation, trigger avoidance, healthy eating, physical activity, and weight loss. Breathing exercises are aimed at altering the breathing pattern and could be considered for some patients with asthma, such as those prone to experiencing hyperventilation.49
Follow-up and referral
Recommendation 8: Regularly follow up all patients with asthma.
Generally, patients with asthma underestimate the importance of regular follow-up, especially when they have infrequent or minor symptoms.3 This belief can be harmful, as it may add to reliance on a solely symptom-driven approach to managing asthma, and increases risk of poor asthma outcomes. Address this belief as part of asthma patient education and provide long-term scheduled appointments with reminders to enhance adherence to follow-up visits.46,50 While all patients with asthma should be followed up at least twice a year, more frequent follow-up should be planned as required (see Table 3 below).
Table 3. Frequency of follow-up for patients with asthma
| Follow up within 1 to 2 weeks |
| Follow up within 1 to 3 months |
| Follow up every 1 to 3 months |
| Follow up at least twice a year |
Recommendation 9: Referral to a specialist could be made at any point.
Most patients with asthma can be effectively managed in primary care. However, specialist referral could be considered at any point, particularly for:
Patients with inadequate response to asthma management, such as persistent or worsening symptoms despite having stepped up preventer treatment and with BREATHE factors addressed where applicable
Patients needing medium to high doses of ICS-containing treatment, or biologic agent
Children with asthma aged 0 to 5 years
Specific patient groups with asthma, such as patients with occupational asthma, pregnant patients, elderly patients, or athletes
Patients in whom the asthma diagnosis is uncertain
Expert group
Co-chairpersons
Clin A/Prof Mariko Koh Siyue, Respiratory and Critical Care Medicine (SGH)
Adj Asst Prof Tan Tze Lee, Family Medicine (The
Edinburgh Clinic)
Members
Dr Ang Joo Shiang, Emergency Medicine (TTSH)
Prof Chay Oh Moh, Respiratory Medicine (KKH)
Ms Joy Chong, Pharmacy (Watson’s Personal Care Stores Pte Ltd)
Dr Choo Xue Ning, Respiratory and Critical Care Medicine (CGH)
Dr Agnes Koong Ying Leng, Family Medicine (SHP)
Mr Ong Kheng Yong, Pharmacy (SGH)
Dr Phua Huei Wen Daryl, Family Medicine (NUP)
Ms Lathy Prabhakaran, Nursing (TTSH)
Ms See Chue Win, Nursing (SHP)
Ms Chioh Mei Suang, Nursing (AIC)
Dr Tan Teck Jack, General Medicine (Northeast Medical Group)
Dr Ronnie Tan Voon Shiong, Internal Medicine (NTFGH)
Dr Jenny Tang Poh Lin, Paediatrics (SBCC Asthma Lung Sleep Allergy and Paediatric Centre)
A/Prof Tang Wern Ee, Family Medicine (NHGP)
Dr Michael Wong Wen Yao, Family Medicine (Raffles Medical Group)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Chronic obstructive pulmonary disease — diagnosis and management
Patient education flipchart on asthma
Written asthma action plan templates
Patient fact sheet on steroid inhalers for asthma
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Asthma – optimising long-term management with inhaled corticosteroid. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2020. Available from: go.gov.sg/acg-asthma-optimising-long-term-management-with-inhaled-corticosteroid
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.