
Generalised anxiety disorder – easing burden and enabling remission ACG
Last updated 19 May 2026
ACE Clinical Guidelines (ACG) provide concise, evidence-based recommendations to inform specific areas of clinical practice and serve as a common starting point nationally for clinical decision-making.
Overview
This ACE Clinical Guideline (ACG) highlights non-pharmacological and pharmacological management of generalised anxiety disorder to achieve remission and reduce the risk of relapse. The ACG offers evidence-based recommendations on assessment for treatment planning, selection of psychological and/or pharmacological treatment, and strategies for inadequate response. Appropriate use of benzodiazepines is also discussed.
Though the guideline focuses on adults (patients 18 years old and above), brief supplementary resources on assessment and management in perinatal women, as well as children and adolescents, are included.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Select the treatment approach by assessing GAD severity and other factors, taking into account the needs, preferences, and readiness of the patient.
For patients with mild GAD:
Consider CBT-based psychological treatments as first-line.
Consider medication if psychological treatments are not feasible or acceptable.
For patients with moderate GAD:
Offer a CBT-based psychological treatment or an SSRI/SNRI medication.
Consider a combination of both modalities if supported by clinical need.
For patients with severe GAD, offer a combination of CBT-based psychological treatment and SSRI/SNRI medication as first-line.
If treatment does not achieve adequate response in patients with GAD, assess possible reasons before considering modifying treatment or seeking specialist advice.
Continue treatment with an SSRI or SNRI for at least six months after achieving remission.
Do not routinely prescribe benzodiazepines as first-line treatment for GAD.
Refer to the Evidence-to-Recommendation (EtR) framework below for a summary of the factors underpinning the ACG’s recommendations.
Download the ACG and reference in PDF
Generalised anxiety disorder – easing burden and enabling remission (Mar 2025) [PDF]
Generalised anxiety disorder – easing burden and enabling remission references (Mar 2025) [PDF]
EtR Framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the major depressive disorder EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Generalised anxiety disorder – easing burden and enabling remission EtR framework (Mar 2025) [PDF]
Request for a hard copy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guidance (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.

Introduction
Generalised anxiety disorder (GAD) is characterised by excessive anxiety and worry across multiple domains of life, with additional physical and/or cognitive symptoms, that lead to significant distress and functional impairment. GAD is reported by patients to have the most significant impact on quality of life compared to other mental health disorders studied in Singapore.1
Enhancing the capacity of community-based mental health care through a tiered care model is a focus area of the 2023 National Mental Health and Well-being Strategy. Accordingly, this ACE Clinical Guidance (ACG) aims to inform the clinical management of adults (18 years old and above) in primary and generalist care with a diagnosis of GAD, including those with comorbid depression or other anxiety disorders. Guidance on major depressive disorder (MDD) can be found in the ACG Major depressive disorder – achieving and sustaining remission.
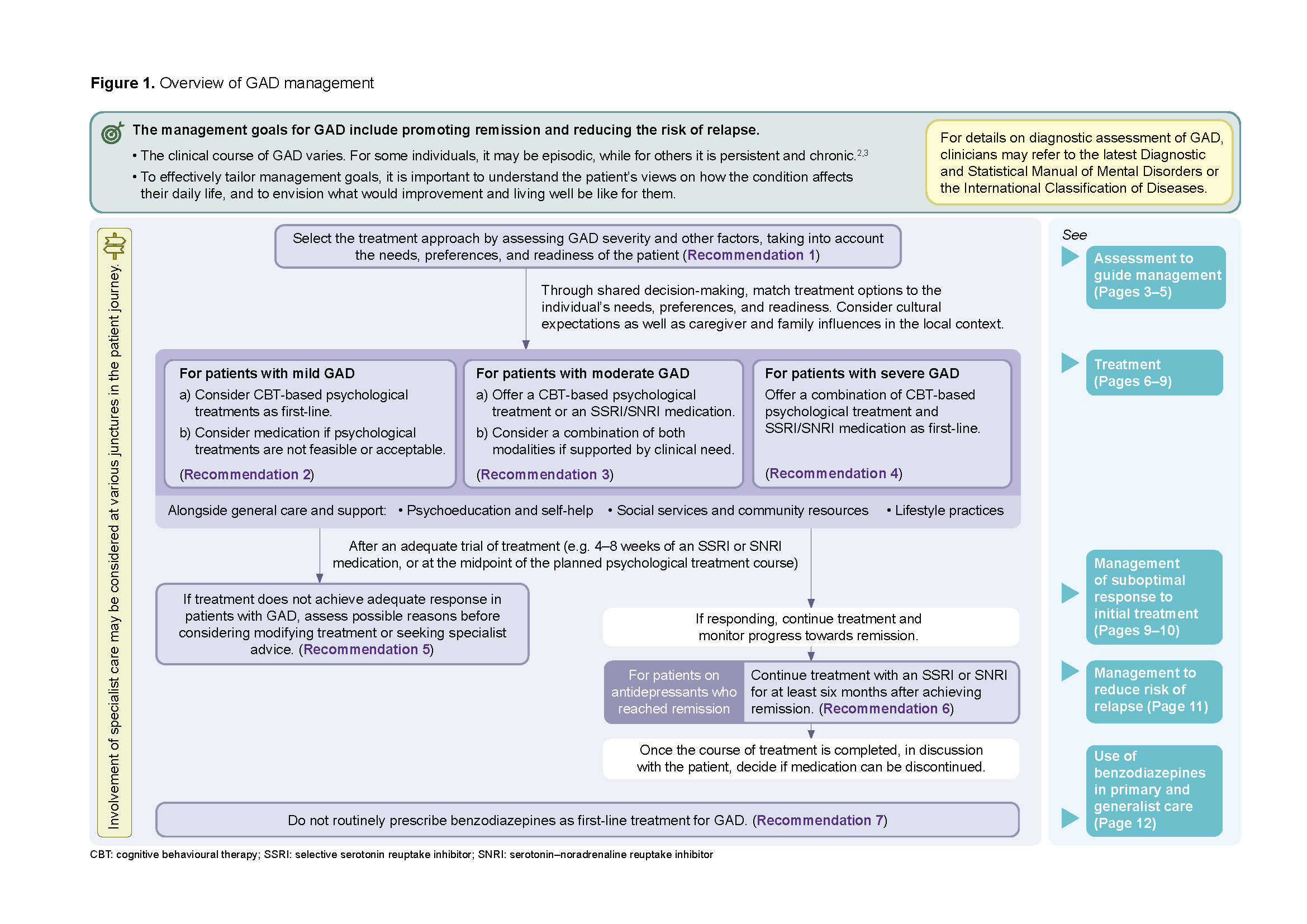
Figure 1. Overview of GAD management
Click here for larger version of this image
Assessment to guide management
Recommendation 1: Select the treatment approach by assessing GAD severity and other factors, taking into account the needs, preferences, and readiness of the patient.
Assessing the severity of symptoms, degree of functional impairment, and other patient factors informs treatment planning.
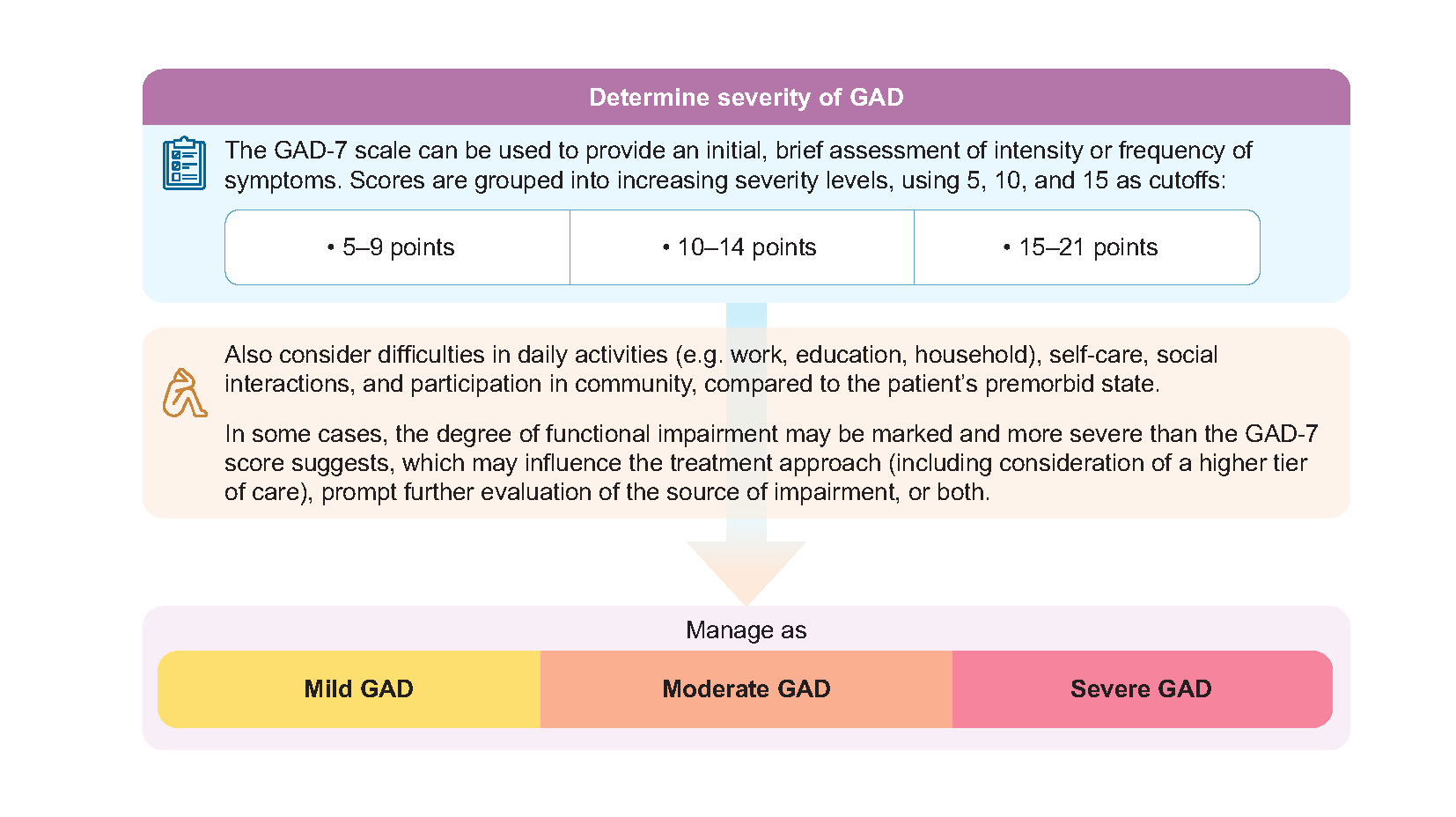
GAD severity
Clinicians should assess whether a patient’s condition is mild, moderate, or severe, based on the intensity of symptoms and the impact on subjective distress and daily functioning.
The Generalised Anxiety Disorder 7-item (GAD-7) scale can be used to monitor the intensity of GAD symptoms over time.4
Functioning can be assessed through the additional functional question in GAD-7 or more systematically through rating scales such as the World Health Organization Disability Assessment Schedule 2.0. Apart from the overall level of disability, clinicians can take note of specific domains where the patient experiences significant difficulties due to their mental health condition.
Other patient factors
Overlay other patient factors to tailor treatment approach to the individual. Patient factors are explored in more detail below and continues on the following page.
Overlay other patient factors |
|---|
Patient needs, preferences, and readiness Consider patient needs, preferences, and readiness by discussing and agreeing on:5,6
|
Comorbid mental health conditions
|
Comorbid physical illnesses
|
Social and environmental factors Identify adverse life events, relationship conflicts, and stressors at home, workplace, or school. Some stressors can be addressed through social care and assistance.7 |
Substance use Specialised, integrated treatment may be suitable to address both substance use (e.g. alcohol, nicotine, prescription medications, or illicit drugs) and GAD. |
GAD treatment history and past episodes Use past responses to medication or psychological treatment to help guide choice of treatment. |
Elderly
|
Perinatal See Supplement 3 (page 16) for principles of care for pregnant and postpartum women. |
Neurodevelopmental disorders (e.g. intellectual disability, autism spectrum disorder, attention-deficit/hyperactivity disorder)
|
Risk of harm to self and others:
Risk of harm to self
GAD is associated with an increased risk of having suicidal thoughts, planning, and attempts.11 Use an empathetic patient-centred approach to identify any thoughts of suicide and planning, as discussions often carry stigma.12
Clinical judgment is essential, and can be informed by questions developed to assess risk. An example is the Columbia-Suicide Severity Rating Scale (C-SSRS) screener. In devising a safety plan, it is also important to understand the patient’s risk factors (e.g. past self-harm, hopelessness), and protective factors (e.g. social support).
Risk of harm to others
Assess if the patient has any thoughts or plans to harm others.
Refer to the upcoming Practice Guide for Tiered Care Model for Mental Health (Adult) for further details on suicide risk management and red flag situations. Patients at high risk may require immediate medical attention at emergency services.
Over the GAD treatment course, the safety plan may need to be revisited.
Monitor closely for emergent suicidal thoughts and behaviour when initiating any antidepressant medication.
Collaborate with other providers or family/caregivers to ensure support is in place.
Treatment
Treatment for GAD is broadly categorised into psychological, pharmacological, or a combination of both modalities.
General care and support complement pharmacological or psychological treatments.
Notepad: General care and support Psychoeducation and self-help
Social services and community resources
Lifestyle practices
|
Psychological treatment
Cognitive behavioural therapy (CBT) has the most empirical support for GAD.19–21 Apart from traditional CBT, other approaches include third-wave CBT (e.g. acceptance and commitment therapy, mindfulness-based cognitive therapy) and transdiagnostic approaches (treatments that target shared features across several disorders).22
Notepad: Psychological treatments Common elements of CBT-based approaches are psychoeducation, cognitive restructuring, behavioural techniques, relaxation, stress and worry management, problem-solving, and relapse prevention. Sleep management may be relevant if sleep is a concern. The number of sessions can vary depending on the patient’s progress and needs. Delivery format Face-to-face therapy has the strongest evidence base for GAD. Guided internet-delivered therapy is emerging as an alternative for suitable individuals with mild to moderate conditions, who may prefer the flexibility and accessibility of learning via online materials supported by trained professionals. |
Applied relaxation, a non-CBT-based approach that teaches patients to counter anxiety with relaxation practices, also has some evidence of efficacy for GAD.19
Pharmacological treatment
Though commonly referred to as ‘antidepressants’, selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs) have anxiolytic effects, and are established first-line medications for GAD.23,24 The choice between individual SSRIs and SNRIs can be guided by factors like the patient’s medical history, concomitant medications, risk of serious adverse effects, and hepatic or renal impairment (see Supplement 1).
Notepad: SSRI and SNRI medications
|
If SSRIs and SNRIs are not suitable or poorly tolerated, effective alternatives include agomelatine, mirtazapine (off-label use), and pregabalin.23 Note that agomelatine carries a risk of liver injury (requiring regular monitoring of liver function) and mirtazapine may cause sedation and weight gain. Consider seeking specialist input for cases where pregabalin might be useful.
Other anxiolytic medications mentioned in this guidance
Hydroxyzine may be useful in mild GAD (see Recommendation 2) or as an adjunct.28 It carries arisk of anticholinergic effects and excessive sleepiness, and may prolong QTc interval.
Some benzodiazepines may be used short-term for anxiety symptoms (see Recommendation 7).
A note on use of complementary and alternative medicine
|
Recommendation 2: For patients with mild GAD; a) Consider CBT-based psychological treatments as first-line; b) Consider medication if psychological treatments are not feasible or acceptable.
CBT-based psychological treatments are preferred when GAD severity is mild, as they are associated with fewer adverse effects compared to pharmacotherapy. However, they may not be feasible or acceptable, such as when:
The healthcare professional assesses a need for, or the patient prefers, initiating treatment sooner (than waiting time allows).
The healthcare professional assesses that some symptomatic improvement is required before the patient can adequately engage in psychological treatment.
The patient is unwilling to engage in psychological treatment.
The patient is unable to attend or commit to regular therapy sessions.
The patient is unable to participate in or understand tasks for therapy sessions (e.g. due to cognitive impairment).
Medication options for mild GAD are either an SSRI or SNRI medication or a trial of hydroxyzine (with a plan to start CBT-based psychological treatment or SSRI or SNRI, if ineffective).
Hydroxyzine has limited usefulness for comorbid depression symptoms, where proven treatments such as psychological therapy or SSRI/SNRI medications are preferred. Due to significant anticholinergic effects, hydroxyzine is also less suitable for elderly patients.
Recommendation 3: For patients with moderate GAD; a) Offer a CBT-based psychological treatment or an SSRI/SNRI medication; b) Consider a combination of both modalities if supported by clinical need.
As either psychological treatment or an SSRI or SNRI medication can be offered first-line for moderate GAD,19–21,23,24 various factors unique to each patient’s situation, including personal preferences and values, must be considered when determining the most appropriate treatment option. Features of each treatment modality are described in Table 1:
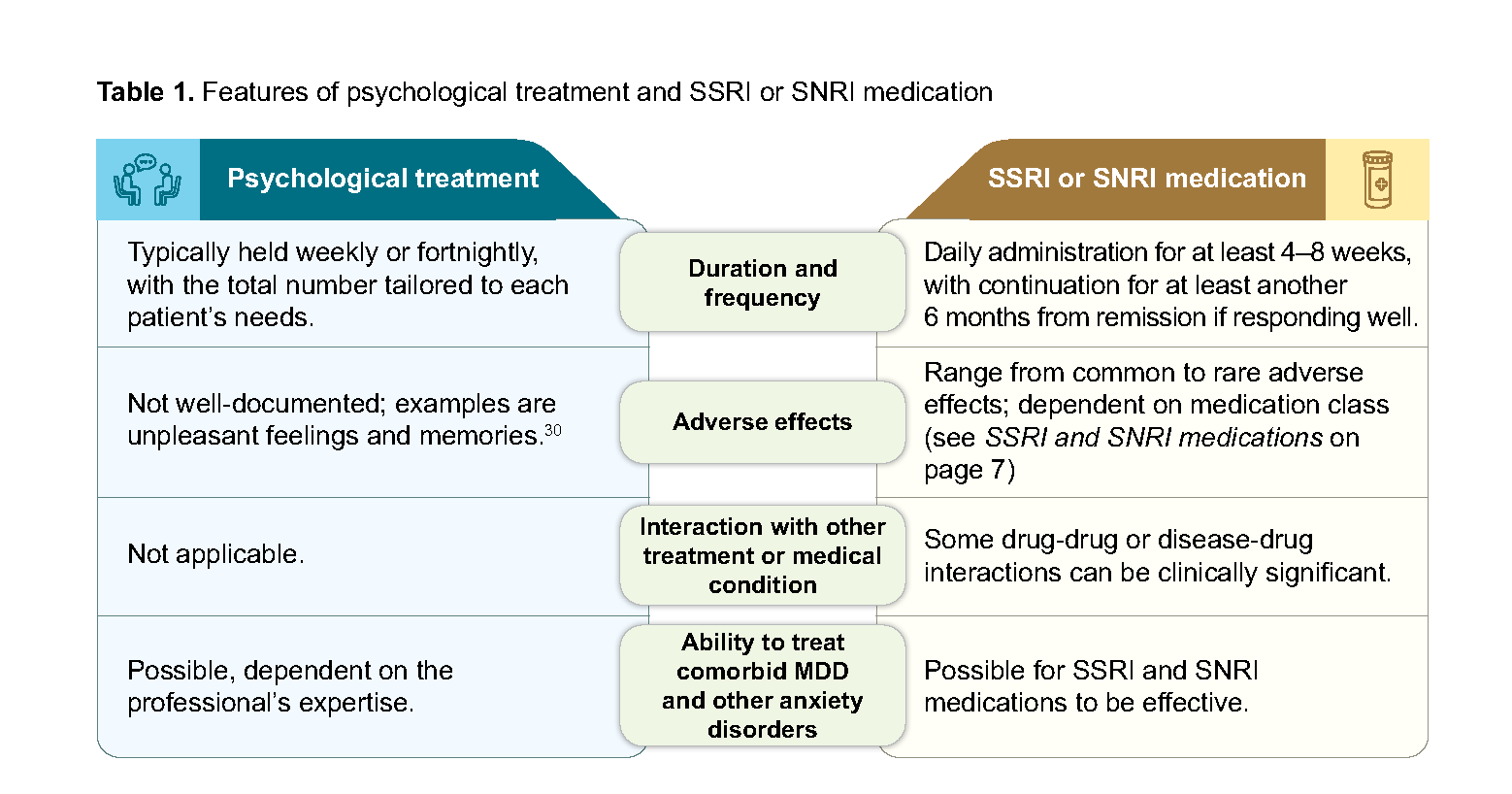
Table 1. Features of psychological treatment and SSRI or SNRI medication
It is unclear from available evidence if combined treatment is more effective than single treatment modality alone. Circumstances that favour combination treatment, based on clinical experience, include:
Presence of comorbid MDD, panic disorder, or social anxiety disorder
Previous treatment response
Intense or prolonged psychosocial stressors
Poor social support
Marked functional impairment
Recommendation 4: For patients with severe GAD, offer a combination of CBT-based psychological treatment and SSRI/SNRI medication as first-line.
Research on combination treatment approaches for GAD is limited.31,32 The potential benefits need to be weighed against higher treatment burden, to ensure patients can adhere to treatment. When combination treatment is not feasible or acceptable, either CBT-based psychological treatment or SSRI or SNRI medication can be offered as alternatives. Psychiatrist-led services with the ability to treat more complex cases are preferred for severe GAD due to possible comorbidities and severity of the condition. Depending on the setting, co-management with specialists may be feasible.
Additional remarks: The recommendation strength is based predominantly on expert consensus. Please click here for the full rationale. |
Notepad: Management considerations for comorbid MDD or anxiety disorders The presence of comorbid MDD and other anxiety disorders contribute to overall functional impairment and may reduce treatment response and remission.33,34
|
Management of suboptimal response to initial treatment
Recommendation 5: If treatment does not achieve adequate response in patients with GAD, assess possible reasons before considering modifying treatment or seeking specialist advice.
Assess response, evaluate patient adherence, and monitor for any adverse effects throughout treatment with psychological treatments and/or medication. It’s important to note the absence of a single definition for response in GAD.
For SSRI and SNRI medications, the time needed to find an optimal dose differs for each patient. As a general guide, the full benefit of an antidepressant should be assessed after 4–8 weeks of treatment, including any titration to reach the recommended dose or range if suitable.a
For psychological treatment, the number of preparatory sessions required to understand therapy work can vary; response could be evaluated at the midpoint of the planned treatment course.
Notepad: Assessing response Response can be evaluated by whether patients have experienced significant improvement in symptoms and functioning, compared against their management goal(s), incorporating both clinical judgement and the patient’s perspective. To inform clinical judgment, some clinicians may find it helpful to have a practical guide on when treatment is likely ineffective after an adequate trial at an optimal dose. For example, a Clinical Global Impressions-Improvement score >2 or <20% improvement on the GAD-7 scale can inform judgment that response could be inadequate.41,42 However, the patient’s perspective remains important in determining the significance of change. |
When an inadequate response is observed (after an adequate trial of treatment), possible reasons that can be evaluated and addressed include:43
Ongoing psychosocial stressors
Suboptimal treatment adherence
Misdiagnosis or presence of other mental health conditions
Comorbid conditions with symptoms that may mimic those of GAD, e.g. hyperthyroidism, arrhythmia
a. Optimal therapeutic doses are not well-established in GAD. Consider adjusting dose based on early response and tolerability, as well as patient profile.
Modifying treatment
If the above reasons do not fully explain the response, consider modifying treatment. The following treatment approaches may be considered (in no particular order) if initial treatment is ineffective (Table 2). As limited evidence is available to inform optimal sequencing of treatment in GAD, choose next-step treatment based on individual patient characteristics and shared decision-making. Seek specialist involvement if response remains inadequate after two trials of treatment, or earlier if needed (e.g. worsening or new symptoms, clinical need for another treatment, tolerability issues with antidepressants).
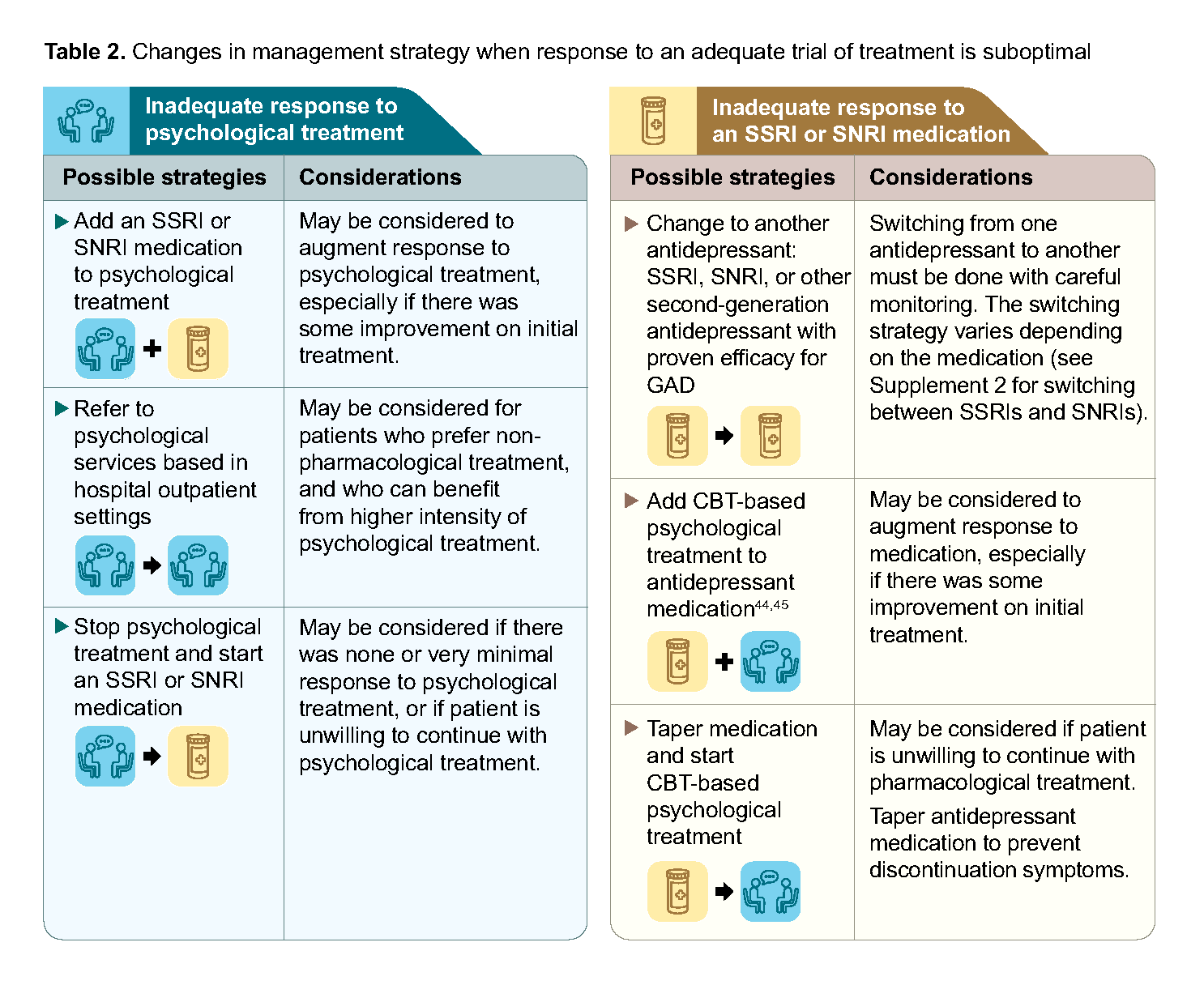
Table 2. Changes in management strategy when response to an adequate trial of treatment is suboptimal
Management to reduce risk of relapse
Recommendation 6: Continue treatment with an SSRI or SNRI for at least six months after achieving remission.
For patients who reach remission on SSRI or SNRI treatment, continuation of the same dose for at least another 6 months (up to 12 months) has been shown to lead to lower relapse rates.46 It is important to note the absence of a single definition for remission in GAD. A guide for assessing these outcomes is provided below.
Notepad: Assessing remission Remission in GAD can be evaluated by all of the following:
On an individual basis, clinicians may also judge remission by other personalised management goal(s) agreed on with the patient. |
Consider tailoring strategies to stay well based on the individual’s needs, e.g. psychoeducation on symptoms of relapse, information on where to seek help, self-help resources, engagement of social support networks, lifestyle and wellness programmes, and regular follow-up.
Role of psychological treatment in preventing relapse
After remission is reached on medication, the evidence for alternative options such as changing to or adding psychological treatment is limited. In those with MDD, psychological treatments or combination with maintenance antidepressants were shown to reduce the risk of relapse (of depression).47
Considerations for continuing or discontinuing antidepressants after 6-month maintenance treatment
Once the course of treatment is completed, in discussion with the patient, decide if medication can be discontinued, taking into account individual factors such as:
History of relapse(s)
Adverse effects
Any ongoing or anticipated psychosocial stressors
Comorbid mental health conditions
Degree of social support, including family
Patient preference
Gradually reduce the dose of antidepressant medications to minimise discontinuation symptomsb and risk of relapse. Patients can be made aware that discontinuation is often associated with distinctive symptoms (e.g. electric sensations, dizziness, depersonalisation), which usually occurs within hours or days of reducing doses or stopping the medication.48
b. Some international guidelines prefer the term ‘withdrawal symptoms’, as this reflects the potential for physical dependence to develop when antidepressants are taken for weeks to months. This ACG uses ‘discontinuation symptoms’, acknowledging its familiarity to clinicians in the local context.
Use of benzodiazepines in primary and generalist care
Recommendation 7: Do not routinely prescribe benzodiazepines as first-line treatment for GAD.
While the onset of action is faster compared to SSRIs or SNRIs,49 prescribing benzodiazepines requires careful clinical assessment and judgment to weigh the benefits and risks for each patient. Due to the potential for dependence and tolerance, this can lead to problems like misuse and addiction, and serious withdrawal symptoms.50,51
Short-term use of benzodiazepines can be considered in GAD management within primary and generalist care for severe acute anxiety. Their role in treatment-resistant GAD is beyond this ACG’s scope.
There are limited studies supporting use of benzodiazepines as an adjunct for increased anxiety during the initial weeks of antidepressant therapy. Alternative options should be considered first, such as initiating the antidepressant at a low dose, non-pharmacological interventions, and/or hydroxyzine. In some patients, despite alternative strategies, short-term benzodiazepine use can be considered for distressing symptoms if required.
Benzodiazepines with anxiolytic action include alprazolam, bromazepam, diazepam, and lorazepam.
Principles of prescribing benzodiazepines
Assess the patient for history of substance abuse, current use of opioid medications and alcohol (or other central nervous system depressants), and presence of respiratory disease. Clinicians should consider the risk of daytime sedation and cognitive impairment, particularly in the elderly. If prescribed, use the lowest effective dose for the shortest duration of time. Aim for short-term use (up to 2–4 weeks) and as-needed dosing.51 Educate the patient on proper use and review for signs of problems due to dependence or tolerance. Consider specialist assessment if there is inadequate relief from short-term use, or difficulties in reducing or stopping benzodiazepine use.
Patient communication points on benzodiazepines in GAD
|
c. The ACG should be read alongside regulatory guidance on prescibing, documentation, and referral to a specialist, such as the Lisence Conditions for Outpatient Medical Service Licensees: Prescribing and Supplying Benzodiazepines and Other Hypnotics.
Supplementary Materials
Supplement 1: A guide to SSRI and SNRI selection for GAD
Supplement 2: Switching between SSRI and SNRI medications
Supplement 3: GAD management considerations for perinatal populations
Supplement 4: GAD management considerations for children and adolescents
Expert group
Chairpersons
Dr Chua Yu Cong Eugene, Family Medicine (NHGP)
Dr Michael Yong Kian Hui, Psychiatry (NUHS)
Members
Mr Desmond Ang Toon Sze, Psychology (KTPH)
Dr James Cheong, Family Medicine (C3 Family Clinic @ Aljunied Crescent)
Ms Cecilia Chng Mui Lee, Nursing (NUH)
Dr Sulaiha Binte Ithnin, Family Medicine (SHP)
Dr Khin Saw Myint, Internal Medicine (NUH)
Ms Sheila Koh Siok Yen, Psychology (SHP)
Dr Lee Yik Voon, Family Medicine (Lee & Tan Family Clinic and Surgery)
Ms Emily Liew Kai Suen, Pharmacy (IMH)
Dr Low Bee Lee, Psychiatry (Mt Elizabeth Novena Specialist Centre)
Dr David Tan Jee Ooi, Family Medicine (NUP)
Dr Tay Xin Ying, Pharmacy (SGH)
Mr Adrian Toh, Psychology (Singapore Psychological Society)
Dr Yeo Cheng Hsun Jonathan, Family Medicine (Family Medicine Clinic Chinatown)
Mr Yin Hao, Nursing (IMH)
Dr Zhou Yi, Internal Medicine (SGH)
The Expert Group would like to thank the co-chairs of the major
depressive disorder (MDD) ACE Clinical Guidance (ACG), for their inputs
and review of this ACG:
Dr Koot David, Family Medicine (SHP)
Adj Asst Prof Mok Yee Ming, Psychiatry (IMH)

Related ACGs and Other related resources
Major depressive disorder – achieving and sustaining remission
National Mental Health and Well-being Strategy (2023)
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Generalised anxiety disorder – easing burden and enabling remission. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2025. Available from: go.gov.sg/acg-gad
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.