
Osteoporosis: diagnosis and management ACG
Last updated 20 May 2026
Published on 15 August 2025 (updated, see below for version history)
Overview
This ACE Clinical Guideline (ACG) provides evidence-based recommendations on risk assessment, timely diagnosis, optimal treatment, and indications for specialist referral in adults with osteoporosis. It covers pharmacological management options, with a focus on antiresorptive and anabolic therapies, and is complemented by a supplementary guide on additional treatment options. Non-pharmacological interventions, including adequate calcium and vitamin D supplementation, regular physical activity and smoking cessation, are also addressed.
First published in 2018, the ACG on osteoporosis has been updated in 2025 to incorporate the latest evidence where relevant. Notably, the 2025 ACG introduces locally derived intervention thresholds for patients with osteopenia, based on an in-house Markov model contextualised to the Singapore healthcare setting. A supplementary guide detailing the methodology for the economic evaluation underpinning these thresholds is also available.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
1.Determine the need for bone mineral density testing in people with risk factors for osteoporosis or fragility fractures, particularly all post menopausal women, and men ≥65 years of age.
2.Optimise lifestyle management for all patients at risk of osteoporosis or fragility fractures, including calcium and vitamin D intake through diet and supplementation as appropriate.
3a.Diagnose osteoporosis and initiate treatment for patients with current or past fragility fracture, or a BMD (measured by central DXA) T-score ≤-2.5.
3b.Consider initiating treatment for people with a BMD (measured by central DXA) T-score between -1.0 and -2.5 and who are at high risk of fractures.
4.For patients in whom pharmacological treatment is indicated:
Use oral alendronate or risedronate (or IV zoledronate if available and preferred)
Consider using denosumab, if preferred and suitable for the patient
5.Consider anabolic agents as first-line treatment for patients at very high risk of fractures, with specialist input as needed.
6.Consider referring patients with clinically complex or unusual presentations to specialists for further assessment and management.
Refer to the Evidence-to-Recommendation (EtR) framework below for a summary of the factors underpinning the ACG’s recommendations
Download the ACG, references
Osteoporosis: diagnosis and management (Aug 2025) [PDF]
Osteoporosis: diagnosis and management references (Aug 2025) [PDF]
Request for a hard copy
ACG EtR framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the osteoporosis EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Osteoporosis: diagnosis and management EtR framework (Aug 2025) [PDF]
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent: This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Osteoporosis is a major public health concern due to its association with fragility fractures, leading to significant morbidity, loss of independence, and increased healthcare costs.1 As osteoporosis is largely asymptomatic until a fracture occurs, timely diagnosis and intervention are key to fracture prevention.
Between 2017 and 2022, the age-standardised incidence* of hip fracture-related hospitalisations in Singapore residents aged ≥50 years declined from 248 to 219 (females) and 125 to 106 (males) per 100,000,2 continuing an earlier reported trend.3 Over the same period and for the same age group (≥50 years), the age-standardised incidence of healthcare visits for fractures at other specific sites (vertebral, upper humerus, and wrist) has remained stable for females at about 708 per 100,000 residents, and increased in males from 289 to 323 per 100,000 residents.2 Nevertheless, the overall burden of fragility fractures remains substantial and crude fracture numbers continue to rise with population ageing, underscoring the need for early identification of at-risk patients and fracture prevention.
In primary care, recognising a patient’s risk of osteoporosis or fragility fractures can enable appropriate diagnosis and management, keeping the patient fracture-free. This ACG provides recommendations on timely diagnosis of osteoporosis and optimal treatment to mitigate the growing burden of osteoporosis and its associated complications (Figure 1).
*The age-standardised incidences are calculated using the 2010 Singapore resident population aged 50 years and above as the reference population.
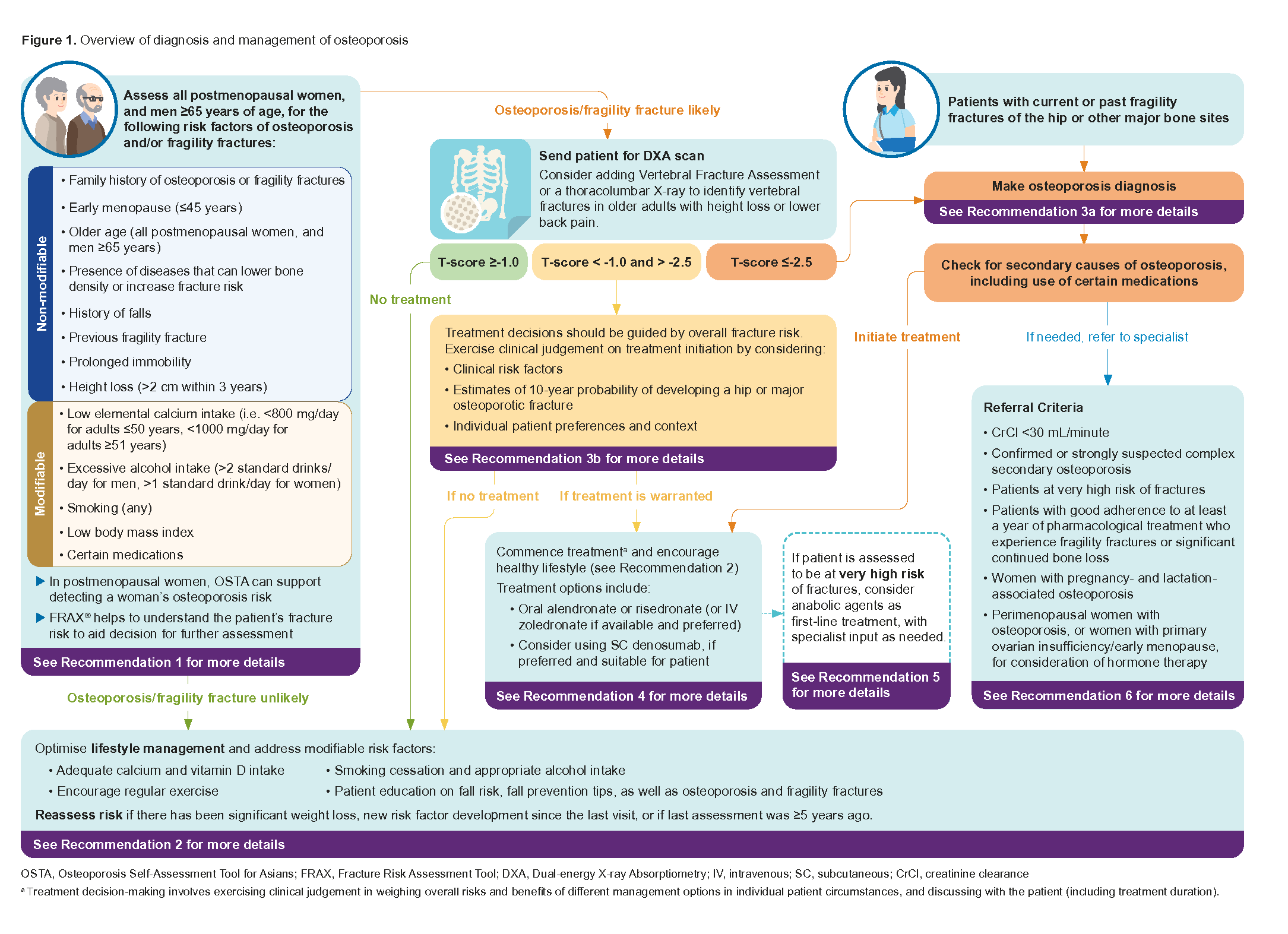
Figure 1. Overview of diagnosis and management of osteoporosis
Click here for larger version of the image
Risk identification for osteoporosis and fragility fracture
Recommendation 1: Determine the need for bone mineral density testing in people with risk factors for osteoporosis or fragility fractures, particularly all postmenopausal women, and men ≥65 years of age.
Recognising patients at risk of osteoporosis or fragility fractures† is key to identifying those who may benefit from further evaluation, counselling, and treatment. As age and sex are well-established risk factors for osteoporosis, further assessment of osteoporosis or fragility fracture risk should be prioritised for all postmenopausal women and men aged 65 years and older.‡
Several risk factors are associated with osteoporosis and fragility fractures (see Table 1) and can be used to guide decision-making on the need for further evaluation (e.g. with bone mineral density (BMD) testing).
Table 1. Risk factors for osteoporosis or fragility fractures
Non-modifiable | Modifiable |
|---|---|
|
|
bRefer to supporting text under Recommendation 3a for common secondary causes of osteoporosis, including use of certain medications.
A few risk assessment tools exist that can help identify individuals at risk of osteoporosis or fragility fractures. In Singapore, the Osteoporosis Self-Assessment Tool for Asians (OSTA)§ is commonly used to guide decisions on osteoporosis screening.5,6 The Fracture Risk Assessment Tool (FRAX®) has also been explored as a screening tool in the local population, but further studies are needed to validate its utility in determining the need for BMD testing.7
Osteoporosis Self-Assessment Tool for Asians (OSTA)
The OSTA is a simple age- and weight-based tool to estimate osteoporosis risk in postmenopausal women. 8,9 Based on the OSTA score, risk is stratified as shown in Figure 2:
High risk (score greater than 20): Proceed with Dual-energy X-ray Absorptiometry (DXA) scan, as the likelihood of osteoporosis (low BMD) is high.
Medium risk (score between 0 and 20): Consider DXA scan if any other risk factor(s) (see Table 1) for osteoporosis is present.
Low risk (score less than 0): Consider deferring DXA scan.
†See Recommendation 3a for the definition of fragility fractures and osteoporosis.
‡Possible osteoporosis risk should be explored in men younger than 65 years if they have significant risk factors such as use of steroids or anti-androgens, or medical conditions associated with bone loss such as hypogonadism or hyperthyroidism.
§OSTA has been validated for use in local postmenopausal women, but not for men in the local population. Thresholds may be updated as new evidence emerges.
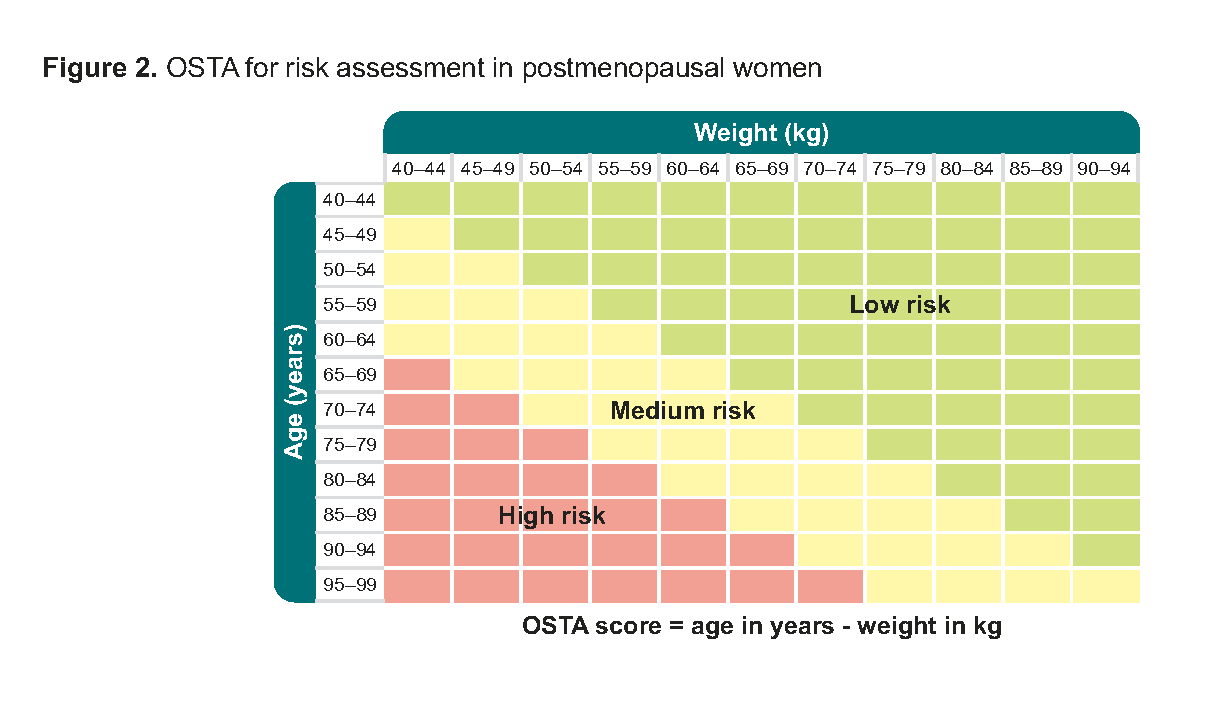
Figure 2.OSTA for risk assessment in postmenopausal women
Postmenopausal women initially classified as low risk on OSTA, should be reassessed if they experience significant weight loss, develop new clinical risk factors, or if their last assessment was five or more years ago.
Fracture Risk Assessment Tool (FRAX®)
The FRAX® tool assesses an individual’s fracture risk by estimating the 10-year probability of a hip fracture or major osteoporotic fracture using age, body mass index, and several other risk factors. 10
The 10-year probability of developing a fracture estimated by FRAX® should be interpreted in light of individual patient circumstances, as the parameters used by FRAX® in the calculation are not exhaustive. Although other fracture risk calculators are available, such as the Garvan fracture risk calculator or QFracture, FRAX® is recommended due to its multi-country validation and the availability of a Singapore model. 10,11
To access the FRAX® calculation tool, click here. Please manually select “Asia” > “Singapore” > “Singapore (Race)” in the country settings, as the default is set to the UK.
Lifestyle advice
Recommendation 2: optimise lifestyle management for all patients at risk of osteoporosis or fragility fractures, including calcium and vitamin D intake through diet and supplementation as appropriate.
A lifelong approach to bone health is essential, as peak bone mass is largely determined in childhood and early adulthood. 12 Inadequate calcium and vitamin D intake in younger years contributes to lower bone density later in life, increasing the risk of osteoporosis and fragility fractures in older adulthood. 12 While adequate calcium and vitamin D intake should be promoted across all ages, it is especially important for individuals identified to be at increased risk of osteoporosis or fragility fractures.
By promoting bone health as a lifelong priority, these lifestyle measures help reduce the risk of osteoporosis and fractures, ensuring better musculoskeletal function and quality of life at all ages (see Table 2). However, when pharmacological treatment is indicated, lifestyle measures alone are insufficient to treat osteoporosis and should be viewed as complementary.
Table 2. Lifestyle measures to support bone health in at-risk patients
Elemental calcium intake | |
1,000 mg/day for adults ≥51 years old13 800 mg/day for adults 19 to 50 years old13 | Encourage dietary sources such as dairy products, green leafy vegetables, tofu, and fortified foods. Supplementation may be needed if dietary intake is insufficient. Calcium and vitamin D supplements are taken together, to optimise calcium absorption. |
Vitamin D intake | |
Testing | |
Baseline serum 25(OH)D testing is recommended. Target serum 25(OH)D:14
| Repeat testing is generally unnecessary but may be considered in patients:
|
Loading | |
Not routinely required in primary care, but may be considered for:
| Common local loading regimen:d
|
Maintenance | |
Recommended maintenance therapy includes either:
| Following vitamin D loading, patients can be transitioned to long-term maintenance therapy. In individuals with vitamin D insufficiency (serum 25(OH)D 20–29 ng/mL), maintenance therapy can be initiated directly.14 |
Physical activity | |
|---|---|
Encourage regular weight-bearing, muscle-strengthening, and balance exercises. | and balance exercises. Examples include regular walking, elastic resistance band exercises, bodyweight and dumbbell exercises, and Tai Chi. |
Smoking and alcohol | |
Advise on non-excessive alcohol intake and smoking cessation (for more details, refer to the ACG “Promoting smoking cessation and treating tobacco dependence”). | Avoid excessive alcohol intake4 , which refers to:
|
Patient education and fall prevention | |
Educate on osteoporosis and fragility fractures, and promote measures to reduce fall risk. Click here to access the patient education aid “Osteoporosis: Know the Facts” | Explain impact of falls on health, mobility and independence. Information for patients is available here. Encourage fall prevention through these tips for patients:
|
c Defined as serum 25(OH)D <20 ng/mL or <50 nmol/L.
d Primary care practitioners may consult specialists if there is uncertainty about loading regimens.
Diagnosis and treatment initiation
Recommendation 3a: Diagnose osteoporosis and initiate treatment for patients with current or past fragility fracture, or a BMD (measured by central DXA) T-score ≤-2.5.
The diagnosis of osteoporosis is defined by either:
the presence of a fragility fracture or
a T-score of ≤-2.5 measured by a hip and/or spine DXA. 15–17
DXA is considered the gold standard for measuring BMD.9,15–19 BMD measurements of the hip and spine are widely accepted for diagnosing osteoporosis, while vertebral fracture assessment or thoracolumbar spine X-ray should be considered in older adults with height loss or lower back pain, to detect vertebral fractures.15
Once osteoporosis is diagnosed, a thorough clinical history and physical examination should be performed to assess for secondary causes. This includes a medication review to identify medications associated with osteoporosis or fragility fractures.
Laboratory tests can be considered to exclude secondary causes of osteoporosis (see Table 3).9,15
Secondary causes of osteoporosis include, but are not limited to:22
Type 1 diabetes mellitus (type 2 diabetes mellitus** is associated with increased fragility fracture risk, even though BMD is often normal or higher)
Vitamin D deficiency
Endocrine disorders (e.g. primary hyperparathyroidism, Cushing’s syndrome, hyperthyroidism)
Hypogonadism (including early menopause)
Renal insufficiency or failure
Rheumatoid arthritis
Malabsorption disorders (e.g. inflammatory bowel disease)
Haematologic malignancies
Anorexia nervosa
Chronic liver disease
Chronic obstructive pulmonary disease
Certain medications
Notepad: Fragility fracture A fracture (such as but not limited to the vertebra, hip, femur, pelvis, humerus, or wrist) that occurs despite sustaining only minimal trauma (such as a fall from standing height or less) or no identifiable trauma. Asymptomatic vertebral fractures are common fragility fractures that may present as changes in the shape and size of the vertebral body, with or without vertebral height loss.20,21 Skull, facial bone, metacarpal, metatarsal and phalangeal fractures are not considered osteoporotic or fragility fractures |
Notepad: Common medications associated with osteoporosis or fragility fractures22,23
This list of medications is non-exhaustive. |
** Clinicians can consider adjustments to fracture risk calculation in the setting of type 2 diabetes mellitus
Table 3. Laboratory tests to identify common secondary causes of osteoporosis
Test | Clinical rationale | |
|---|---|---|
More commonly indicated | Creatinine | Chronic kidney disease is associated with increased fracture risk, and chronic kidney disease-mineral and bone disorder (CKD-MBD) may be seen in advanced stages of CKD. A baseline renal function can also inform treatment choice. |
Full blood count | Abnormalities might indicate the presence of malignancies, malabsorption, and rheumatoid arthritis. | |
Corrected calcium | Increased level might indicate primary hyperparathyroidism or malignancy; decreased level might indicate malabsorption or vitamin D deficiency. | |
25-hydroxy vitamin D | Establish baseline vitamin D level (aim for ≥30 ng/mL [≥75 nmol/L] for people diagnosed with osteoporosis and older persons at risk of falls).e | |
Others | Thyroid-stimulating hormone | Decreased levels might indicate hyperthyroidism or over-replacement with thyroxine. |
Erythrocyte sedimentation rate (ESR) | Elevated ESR in patients with symptoms and signs of inflammatory arthritis might suggest rheumatoid arthritis. A raised ESR in association with raised creatinine and anaemia might indicate haematologic malignancies such as multiple myeloma. | |
Alkaline phosphatase | Increased levels might indicate liver disease, Paget’s disease, recent fracture, vitamin D deficiency or other bone pathology. | |
Serum phosphatef | Abnormal levels might indicate vitamin D deficiency or renal phosphate wasting. | |
Spot urine calcium/ creatinine ratio | Elevated levels might indicate idiopathic hypercalciuriag | |
Serum total testosteroneh | Decreased levels might indicate hypogonadism but should be interpreted alongside sex hormone-binding globulin (SHBG) level to assess free testosterone levels. |
e Repeat testing may be considered for patients on parenteral treatment (e.g. intravenous zoledronic acid or subcutaneous denosumab), or assessing adherence to vitamin D supplementation.
f Fasting needed for more accurate results.
g Urinary calcium/creatinine level >0.6 (urine calcium and urine creatinine in mmol/L) suggests the need to do 24-hour urine calcium test.
h In men <70 years of age or in those with hypogonadal symptoms. Morning test and fasting recommended for more accurate results. Consider assessing SHBG if total testosterone is borderline or inconsistent with clinical findings.
Recommendation 3b: Consider initiating treatment for people with a BMD (measured by central DXA) T-score between -1.0 and -2.5 and who are at high risk of fractures.
While osteoporosis is defined by a T-score ≤-2.5 or the presence of a fragility fracture, individuals with low bone mass (T-score between -1.0 and -2.5) may still be at high risk of fractures and could benefit from treatment. The decision to initiate pharmacological therapy for patients with low bone mass should be based on overall fracture risk assessment rather than BMD alone, incorporating clinical risk factors (see Table 1), patient preferences and shared decision-making.15,24 In some cases, lifestyle modifications and ongoing monitoring may be sufficient.24
Notepad: Treatment decisions in the absence of DXA If DXA is unavailable or delayed, clinicians may initiate treatment without BMD results, particularly for patients with prior fragility fractures or multiple risk factors. In such instances, treatment decisions should be guided by fracture risk assessment and careful clinical judgment. |
How to assess fracture risk?
Fracture risk is influenced by various modifiable and non-modifiable risk factors (see Table 1). Risk factor information can be integrated via fracture risk prediction tools, such as FRAX®, to support clinical decision-making.25 Based on local fracture incidence and healthcare data, recommended clinical and cost-effective intervention thresholds have been developed by ACE for the Singapore population and summarised in Figure 3. See the supplementary material “Methodology used for economic evaluation of intervention thresholds for patients with osteopenia” for the evidence and Expert Group deliberations underpinning the recommended thresholds. Intervention thresholds should be interpreted in the context of the patient’s overall risk profile and not viewed as strict cut-offs. For example, when patients’ fracture risk exceeds the intervention threshold, clinicians should still weigh the benefit-risk balance for the individual patient and employ shared decision-making to determine whether or not to initiate treatment.
Monitoring and reassessment
For individuals with low bone mass who are not started on treatment, optimisation of lifestyle management and periodic reassessment of fracture risk is recommended, particularly if they develop new fractures or there are changes in clinical risk factors (see Table 1).24 The decision on DXA scan intervals should be guided by the expected rate of BMD change and overall fracture risk assessment.†† Treatment should be reconsidered if fracture risk exceeds the age- and sex-specific intervention thresholds during reassessment or if a diagnosis of osteoporosis is made.
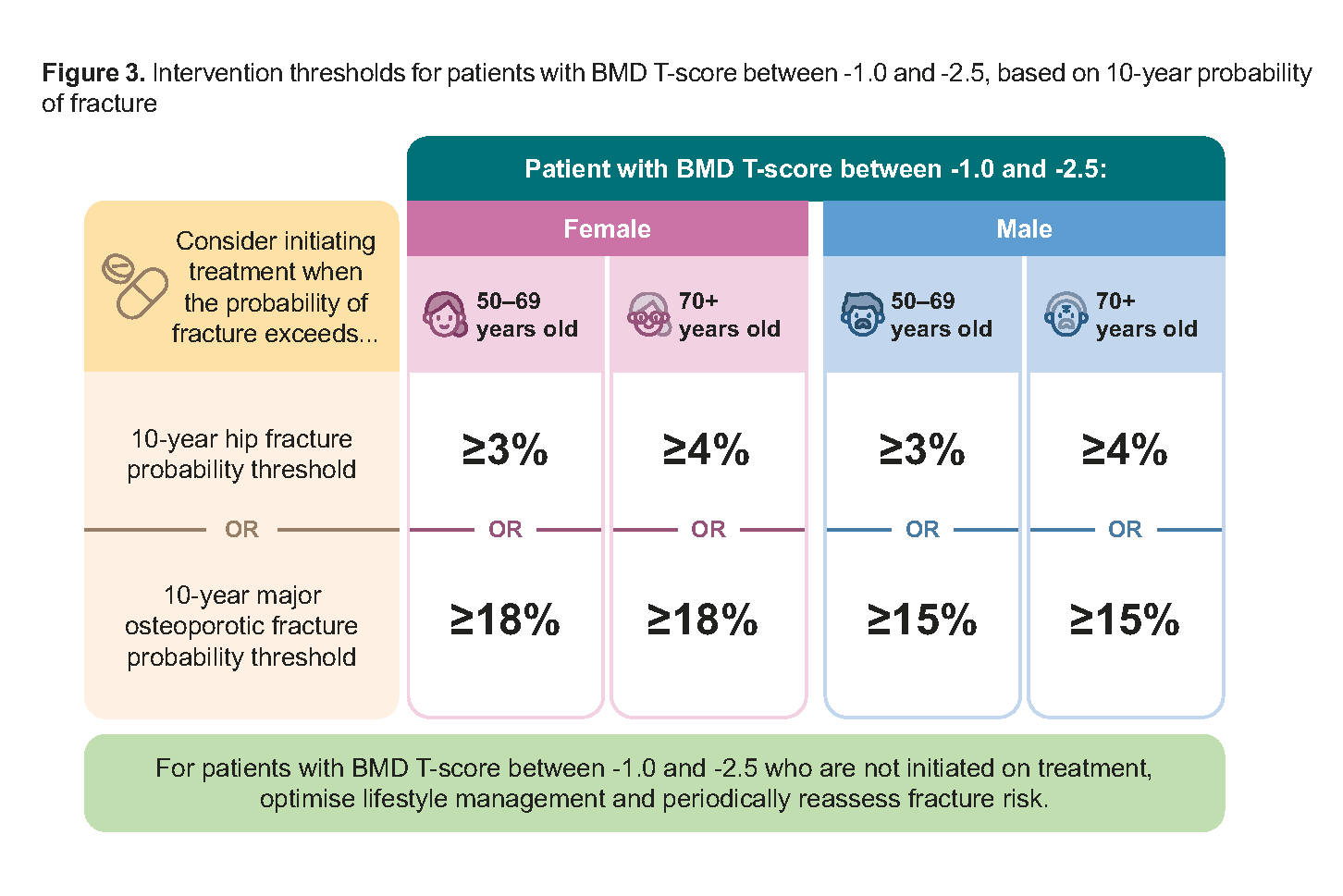
Figure 3. Intervention thresholds for patients with BMD T-score between -1.0 and -2.5, based on 10-year probability of fracture
Pharmacological treatment and specialist referral
Recommendation 4: For patients in whom pharmacological treatment is indicated: Use oral alendronate or risedronate (or IV zoledronate if available and preferred); Consider using denosumab, if preferred and suitable for the patient.
The choice of therapy should be based on effectiveness in fracture prevention, patient preference, comorbidities, renal function, and likelihood of adherence. Oral bisphosphonates are the preferred first-line treatment due to their effectiveness and cost-efficiency, with IV zoledronate as an alternative for those who cannot tolerate oral forms. Denosumab can also be considered when bisphosphonates are unsuitable or not preferred (see Table 4).9,15,26,27 However, discontinuation of denosumab requires careful transition (usually to a bisphosphonate), in order to prevent rapid rebound bone loss and associated increase in fracture risk, notably vertebral fractures.
Notepad: Additional treatment options Raloxifene, a selective oestrogen receptor modulator, may be considered in postmenopausal women, especially those with vertebral osteoporosis or elevated breast cancer risk. Menopausal hormone therapy (e.g. combined oestrogen-progestogen regimen or tibolone) may be considered in selected cases, such as younger postmenopausal women, or those with early menopause or primary ovarian insufficiency. Consider referral to a specialist for further evaluation and management (see Recommendation 6). See the supplementary material “Osteoporosis treatment options, in addition to antiresorptive and anabolic agents” for more information. |
†† Repeat DXA BMD measurements should be performed on the same machine or model, where possible, to improve accuracy and reliability when interpreting changes in BMD over time.
Table 4. Information on bisphosphonates and denosumab
Drug | Evidence of effectiveness in reducing risk of:15,28–31 | Contraindicationsj | Clinical considerations/precautionsj |
Alendronate, risedronate or ibandronatei (bisphosphonates, oral) |
|
| Advise patient to:
|
|---|---|---|---|
Zoledronatei (bisphosphonate, IV) |
|
|
|
Denosumabi (RANKL inhibitor, SC) |
|
|
|
CrCl, creatinine clearance; IV, intravenous; SC, subcutaneous; RANKL, receptor activator of nuclear factor kappa-beta ligand
i Bolding denotes availability on government subsidy list at the time of publication; underlining denotes availability on Healthier SG Medication List at the time of publication.
j Information on contraindications and clinical considerations/precautions were sourced from HSA-approved Package Inserts and UpToDate.32,33
Treatment monitoring
Baseline DXA scan should ideally be performed at treatment initiation. However, in patients with a history of fragility fractures, pharmacological treatment for secondary fracture prevention should not be delayed while awaiting BMD results, given the high risk of re-fracture within the first year. 34
Repeat DXA scan should be considered after 2 years of treatment to evaluate clinical effectiveness.
Subsequent DXA scans may be performed every 2 years to assess for significant DXA BMD deterioration (defined as a decline exceeding the least significant change or >4–5%) or the presence of new fractures.
Any fracture occurring while on medication, including asymptomatic vertebral fractures, should prompt reassessment of treatment strategy. Consider referral to specialist (see Recommendation 6).
Antiresorptive-associated risks and drug holidays
Antiresorptive drugs (bisphosphonates and denosumab) are highly effective in reducing fracture risk, with benefits that far outweigh the risks of long-term use. However, rare but significant side effects, including medication-related osteonecrosis of the jaw and atypical femoral fractures, can occur. While these risks are very low in osteoporosis treatment, clinicians should remain vigilant and counsel patients accordingly.
Medication-related osteonecrosis of the jaw
Medication-related osteonecrosis of the jaw (MRONJ) is characterised by exposed, non-healing bone in the jaw, typically following dental extractions or trauma.
Incidence
MRONJ is extremely rare in osteoporosis treatment with antiresorptive drugs, occurring in 0.001% to 0.05% patients per year.15,18,35–39
MRONJ risk is higher in patients with cancer taking antiresorptive drugs, especially those with multiple myeloma, prostate and breast cancer.15,18,35,38–42
Dental hygiene and clearance15,18,35,39,40,43
Before initiating antiresorptive treatment:
Obtaining dental clearance is not routinely necessary before initiating antiresorptive treatment for osteoporosis. However, an oral health assessment by a dental professional is advisable for patients at higher risk of MRONJ (e.g. patients with cancer undergoing treatment, immunosuppression, history of MRONJ or dental abscesses, concomitant periodontal disease, parenteral osteoporosis therapies) and for patients requiring invasive dental procedures (e.g. extractions, implants). It would be prudent to complete any dental procedures before starting antiresorptive treatment. In patients at high fracture risk, consider administering osteoporosis and dental treatments concurrently, where feasible. Overall, patients with poor oral health status are at increased risk of MRONJ and should be encouraged to maintain good oral hygiene.
During antiresorptive treatment:
Temporary discontinuation of bisphosphonates before invasive dental procedures is generally not required but may be considered for patients at higher risk of MRONJ. For patients on denosumab, invasive dental procedures may be timed at least 2 to 4 weeks before the next scheduled six-monthly injection to support mucosal healing.
Clinical decisions should prioritise individual risk assessment and preventive care, as there is no strong evidence that stopping treatment reduces MRONJ risk – and doing so must be balanced against the risk of fractures.
Atypical femoral fracture
Atypical femoral fracture (AFF) is characterised by low-trauma fractures of the femoral shaft. These fractures often present with prodromal thigh, hip, or groin pain weeks to months before the fracture occurs.15,18
Incidence
Risk of AFF increases with prolonged use of antiresorptive drugs, with cumulative incidence reaching approximately 0.1%, with Asians having a 4- to 5-fold higher risk compared to Caucasians.44
The likelihood of AFF rises significantly beyond 5 years of treatment, necessitating careful reassessment of continued therapy.44
Stopping antiresorptive therapy may reduce AFF risk, supporting the consideration of a drug holiday in long-term users (applicable to bisphosphonates only).15,18
Drug holiday for bisphosphonates
Re-evaluate patients 5 years after starting oral bisphosphonates or 3 years after IV zoledronate to determine if a drug holiday is appropriate.15,45 Drug holidays are generally recommended for patients at low fracture risk after long-term therapy to mitigate the risks of AFF and MRONJ, while still leveraging the residual fracture protection bisphosphonates provide after discontinuation.45 However, fracture risk should be reassessed periodically during the drug holiday, particularly in patients with risk factors such as declining BMD, new fractures or increased fall risk (see Figure 4).46–48
Notepad: Drug holiday for denosumab Drug holidays are not recommended for patients on denosumab, due to the risk of rapid bone loss and multiple vertebral fractures upon cessation.49 If denosumab needs to be stopped or delayed, a plan to transition to a bisphosphonate should be in place, where appropriate.50,51 |
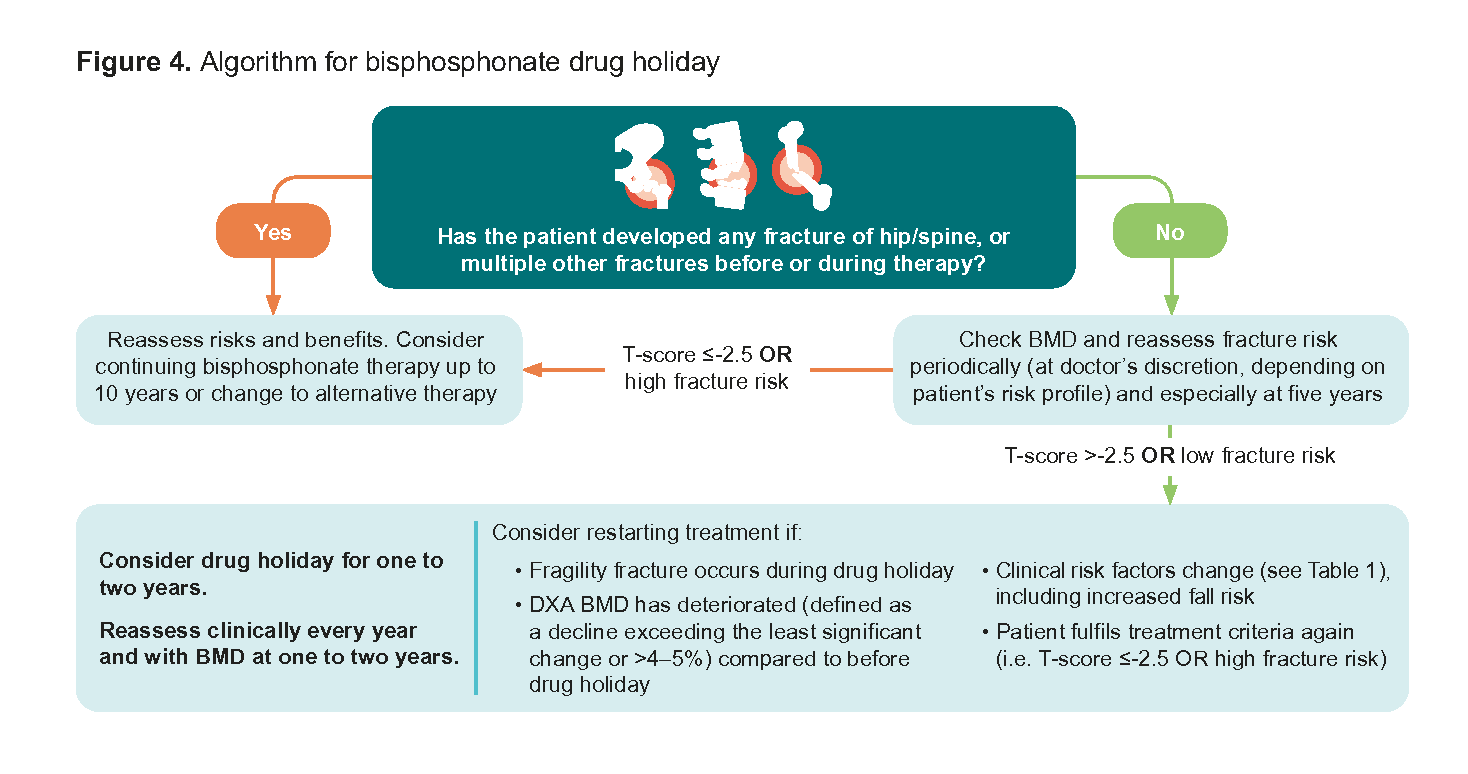
Figure 4. Algorithm for bisphosphonate drug holiday
Recommendation 5: Consider anabolic agents as first-line treatment for patients at very high risk of fractures, with specialist input as needed.
Anabolic agents have demonstrated greater benefit in reducing fractures among patients at very high risk of fractures, particularly when initiated before antiresorptive therapy.52 Teriparatide and romosozumab are potent osteoanabolic agents that actively stimulate new bone formation, unlike antiresorptive drugs that primarily slow bone loss.52,53 They have been shown to significantly reduce fracture risk (see Table 5)53–61 and should be reserved for patients at very high risk of fractures, defined as those with:
Very low BMD (T-score ≤-3.0), and
≥2 vertebral fractures or ≥2 fragility fractures
While anabolic agents are usually not a first-line treatment for osteoporosis due to cost, frequent injection requirements, and the availability of effective antiresorptive agents, they remain a key option for osteoporosis cases where fracture risk is highest.
Table 5. Information on teriparatide and romosozumab
Drug | Evidence of effectiveness in reducing risk of:53–61 | Contraindicationsl | Clinical considerations/precautionsl |
|---|---|---|---|
Teriparatidek (recombinant parathyroid hormone, subcutaneous) |
|
|
|
Romosozumab (humanised monoclonal antibody) |
Registered for treatment in postmenopausal women only |
|
|
SC, subcutaneous
k Bolding denotes availability on government subsidy list at the time of publication. Teriparatide biosimilars may be used in place of originator products.
l Information on contraindications and clinical considerations/precautions were sourced from HSA-approved Package Inserts and UpToDate.62,63
Recommendation 6: Consider referring patients with clinically complex or unusual presentations to specialists for further assessment and management.
Certain patients with osteoporosis may require specialist input due to complex underlying conditions, high fracture risk despite treatment or unique physiological considerations. Referral ensures appropriate diagnostic workup, optimised treatment strategies, and multidisciplinary care when needed.
Consider referring these patients to a specialist:
CrCl‡‡ estimated by Cockcroft-Gault equation <30 mL/minute§§
Confirmed or strongly suspected complex secondary osteoporosis (see Table 3)
Patients at very high risk of fractures*** (see Recommendation 5)
Patients who experience fragility fractures or significant continued bone loss while on treatment, despite good adherence to at least a year of pharmacological treatment†††
Women with pregnancy- and lactation-associated osteoporosis64
Perimenopausal women with osteoporosis, or women with primary ovarian insufficiency/early menopause, for consideration of hormone therapy
‡‡CrCl is preferred over eGFR to guide dosing regimens because eGFR may be overestimated in those with low muscle mass and underestimated in those with high muscle mass.
§§ Consider referring patients with severe renal impairment to distinguish osteoporosis from renal bone disease and ensure appropriate treatment selection.
*** Defined as having very low BMD (T-score <-3.0) and ≥2 vertebral fractures or ≥2 fragility fractures.
††† Central DXA BMD deterioration of >4-5%, or exceeding least significant change (LSC), compared to previous measurement. Monitoring with LSC assumes the patient’s repeat BMD measurement is conducted at the same centre as previous measurement. DXA centres are encouraged to calculate their own precision errors and LSCs according to the International Society of Clinical Densitometry standards.
Supplementary guides
Expert Group
Chairpersons
Adj A/Prof Bernard Thong, Rheumatology (TTSH)
Dr Derek Choong Shangxian, Family Medicine (SHP)
Members
Dr Alexis Ang Guat Cheng, Geriatric Medicine (CGH)
Dr Chan Kin Ming, Geriatric Medicine (Chan KM Geriatric & Medical Clinic, Gleneagles Medical Centre)
Dr Andre Tan Teck Huat, Endocrinology (AH)
Dr Chew Chee Kian, Endocrinology (TTSH)
Dr Cho Li Wei, Endocrinology (LW Cho Endocrine Clinic)
Dr Thomas FJ King, Endocrinology (CGH)
Dr Chua Yang, Obstetrics & Gynaecology (A Clinic for Women, Mount Alvernia Hospital)
Prof Yong Eu Leong, Obstetrics & Gynaecology (NUH)
Adj A/Prof Joyce Koh Suang Bee, Orthopaedic Surgery (SGH)
Dr Victor Seah, Orthopaedic Surgery (Pinnacle Orthopaedic Group)
Dr Christine Ng, Family Medicine (NUP)
Dr Kee Kok Wai, Family Medicine (NHGP)
Dr Kenneth Choo Wei Qiang, Family Medicine (NUS)
Dr Murshitha Shereen Bte Sayed Majunoon, Family Medicine (Raffles Medical Group)
Dr Yeo Cheng Hsun Jonathan, Family Medicine (Family Medicine Clinic Chinatown)
Dr Cheryl Tan Wei Yan, Pharmacy (NHGPh)
Ms Chan Shi Mun, Pharmacy (NUHS)
Ms Anna Purani d/o Raman Singarasoo, Nursing (SHP)
Ms Chan Cheuk Ying, Nursing (NHGP)
The Expert Group would like to thank the Chief Dental Officer, Ministry of Health, and the College of Dental Surgeons, Singapore, for their inputs to this ACG.
Version history
Osteoporosis: diagnosis and management
Version no. | Notes | Date of release |
|---|---|---|
1.0 | Publication of guideline | 7 November 2018 |
2.0 | Publication of updated guideline (incorporates the latest evidence where relevant and introduces locally derived intervention thresholds for patients with osteopenia) | 15 August 2025 |
Feedback
Click here to give us feedback on this ACG.
Other related resources
Patient education aid – osteoporosis: know the facts [PDF]
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Osteoporosis: diagnosis and management. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2025. Available from: go.gov.sg/acg-osteoporosis
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.