
Venous thromboembolism — treating with the appropriate anticoagulant and duration ACG
Last updated 26 May 2026
Published on 28 May 2018
Last Updated on 16 May 2024
Overview
This ACE Clinical Guideline (ACG) provides evidence-based recommendations on selecting an appropriate anticoagulant and treatment duration for different patient groups with venous thromboembolism (VTE), such as patients from the general population (including those with severe renal impairment or liver disease) and those with active cancer. Guideline on when to extend therapy is also provided.
First published in 2018, the ACG on VTE treatment has been updated to incorporate the latest evidence where relevant.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Start anticoagulation as soon as possible for patients with confirmed proximal DVT or PE, unless contraindicated.
For patients from the general population, use a DOAC for at least 3 months as the preferred anticoagulant for VTE treatment; consider warfarin as an alternative if DOACs are not suitable.
For patients with cancer needing VTE treatment, use apixaban, edoxaban, rivaroxaban, or LMWH for the initial and treatment phases for at least 6 months; LMWH is preferred if the patient has gastrointestinal cancer.
Download the ACG and reference
VTE - Treating with the appropriate anticoagulant and duration (May 2024) [PDF]
A supplementary guide on switching between anticoagulants is included.
VTE - Treating with the appropriate anticoagulant and duration – references (May 2024) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent: This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Venous thromboembolism (VTE) is a serious medical condition that covers deep vein thrombosis (DVT) and pulmonary embolism (PE). Globally, patients face a 30-day mortality risk of 5% for PE and 3% for DVT following diagnosis. 1,2 Although the annual incidence of VTE in Asia (ranging from 13.8 to 19.9 per 100,000 people) is lower than the rest of the world, VTE prevalence is increasing over time likely due to population ageing, higher number of surgeries, and higher cancer rates. 3 As VTE has long-term complications that adversely affect quality of life and often leads to substantial healthcare utilisation, this ACG aims to guide healthcare professionals to optimise the treatment of VTE with an appropriate anticoagulant and treatment duration.
Treatment initiation
Recommendation 1: Start anticoagulation as soon as possible for patients with confirmed proximal DVT or PE, unless contraindicated.
The risk of thrombus extension is highest in the first few days after VTE is diagnosed. 4 Therefore, starting anticoagulation as soon as possible is crucial to prevent extension, VTE recurrence, morbidity, and death. Absolute contraindications for anticoagulation include severe coagulation defects, severe thrombocytopaenia, uncontrollable active bleeding, and acute haemorrhagic stroke. For these patients, temporary insertion of an inferior vena cava filter is usually considered. 5–9
Notepad: Isolated distal DVT Following distal DVT diagnosis, the decision to initiate anticoagulation therapy depends on considerations such as:
A short course of anticoagulation may be preferred for patients with any of the above.5 However, monitoring with serial imaging may be sufficient or preferred for those with transient/reversible risk factors (e.g., surgery, trauma, immobilisation, bed confinement, long-haul flight, pregnancy, or oestrogen therapy). 5,10 |
Choice of anticoagulation therapy
Anticoagulants for VTE treatment include direct oral anticoagulants (DOACs), warfarin, low molecular weight heparin (LMWH), and unfractionated heparin (UFH). When selecting an appropriate anticoagulant, consider patient factors, medication properties, patient preferences, and cost. Figure 1 summarises selection criteria and treatment duration, and Table 1 summarises key medication characteristics.
Recommendation 2: For patients from the general population, use a DOAC for at least 3 months as the preferred anticoagulant for VTE treatment; consider warfarin as an alternative if DOACs are not suitable.
DOACs are the oral anticoagulant of choice for most patients with VTE in the general population. DOACs (apixaban, dabigatran, edoxaban, and rivaroxaban) are as effective as warfarin in preventing VTE recurrence, with the added benefit of reducing the likelihood of bleeding outcomes. 11 Other advantages of DOACs over warfarin include fewer drug and dietary interactions, and fixed dosing. Warfarin should be considered when DOACs are not suitable (see Figure 1 for examples of when DOACs are not suitable and for warfarin prescribing considerations).
There is insufficient evidence to recommend one DOAC over another as there are no head-to-head trials comparing DOACs. Practical considerations, such as the need for initial parenteral anticoagulation, would inform the choice of DOAC (see Table 1). While not commonly used locally, edoxaban is registered in Singapore for VTE treatment and listed in this ACG where appropriate, for completeness.
Notepad: Patients at the extremes of body weight The pharmacological effects of anticoagulants may be altered by body weight, as this affects medication absorption, distribution, and elimination. Evidence for patients who are underweight is limited 12,13 and closer monitoring for signs and symptoms of bleeding is recommended, especially while on DOACs (warfarin and LMWH can also be considered, as their anticoagulation effects can be feasibly monitored). Consider specialist referral for patients who are underweight (e.g., those <40 kg). For patients who meet the definition for obesity,* evidence suggests that treatment considerations can be similar to those of the general population.14 Consider specialist referral for patients who have undergone bariatric surgery. |
* For Asian populations, obesity is defined as body mass index (BMI) ≥27.5 kg/m2. Pharmacokinetic data has shown that in patients weighing ≥120 kg, apixaban and dabigatran have reduced systemic exposures, while rivaroxaban has higher systemic exposure than patients in the general population.15
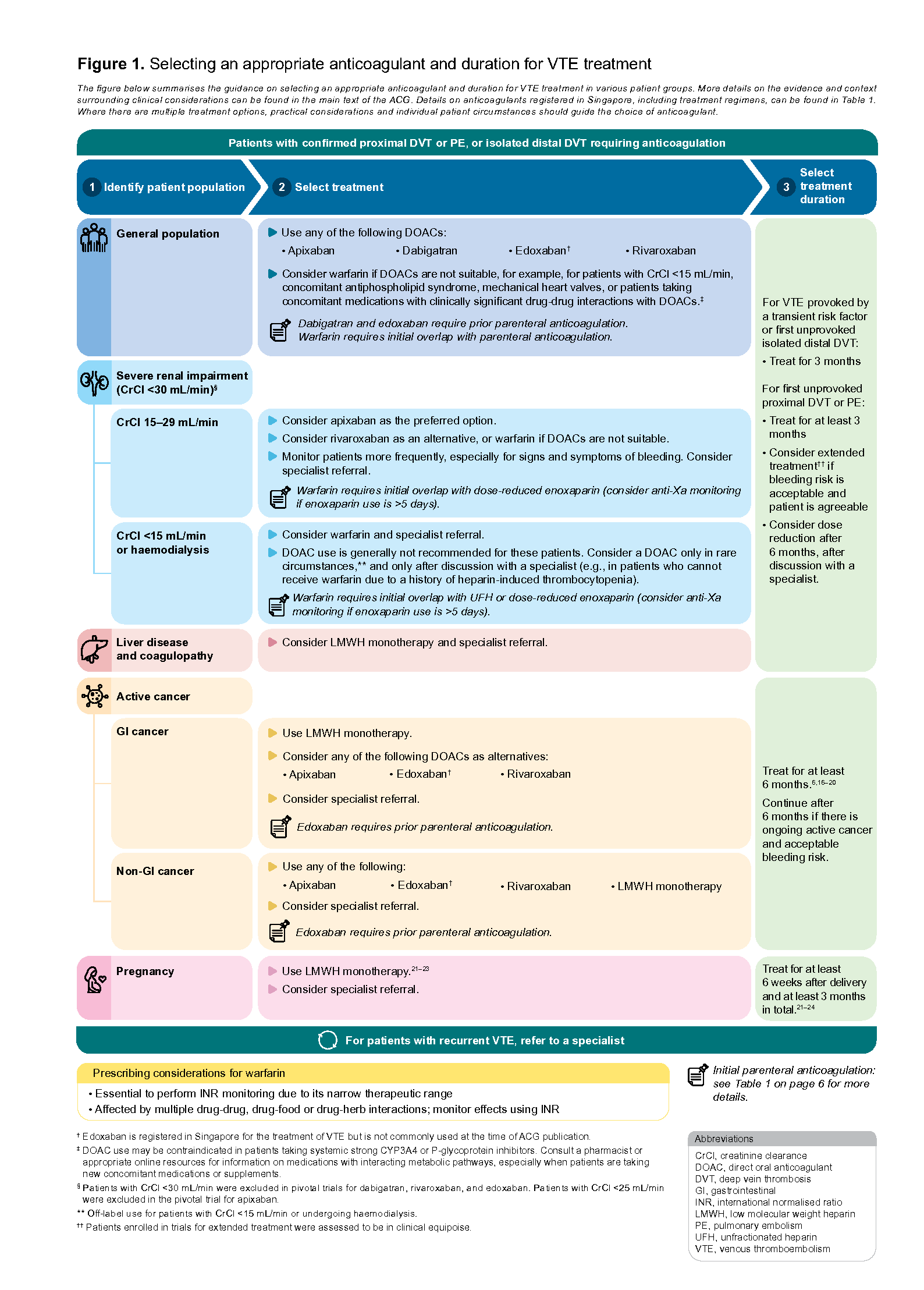
Figure 1.Selecting an appropriate anticoagulant and duration for VTE treatment
Click here for the enlarged image of the above figure.
Patients with severe renal impairment
Evidence from observational studies indicates that apixaban is associated with fewer rates of VTE recurrence and fewer bleeding events compared to warfarin for patients with CrCl 15–29 mL/min.7,25 Limited evidence on rivaroxaban in patients with CrCl 15–29 mL/min suggests similar rates of VTE recurrence compared with warfarin and no increase in major bleeding with decreasing renal function. 26 There are no clinical studies for edoxaban in patients with CrCl 15–29 mL/min at the time of ACG publication. Product information leaflets state that apixaban and rivaroxaban may be used with caution in patients with CrCl 15–29 mL/min, based on pharmacokinetic data. On balance, apixaban can be considered as the preferred option when treating VTE for patients with CrCl 15–29 mL/min.
LMWH monotherapy is not recommended as LMWH is renally excreted and accumulates in renal failure.27 Patients with CrCl <30 mL/min treated with therapeutic enoxaparin have elevated levels of anti-Xa and an increased risk of a major bleeding.28,29 Therefore, consider anti-Xa monitoring if dose-reduced enoxaparin is used for more than five days as an initial overlap with warfarin.
UFH monotherapy is also not recommended. Despite its minimal renal excretion and short half-life, UFH is impractical for prolonged use. UFH is usually reserved for patients undergoing invasive procedures, thrombolysis, or those with high bleeding risks as it requires close laboratory monitoring to achieve therapeutic anticoagulation.30
As renal impairment increases the risk of VTE and bleeding events,31 patients with reduced renal function may require dose adjustments (see Table 1) or more frequent monitoring. When considering switching from a DOAC to warfarin in patients with renal impairment, INR should be checked early (see Supplementary guide “Switching between anticoagulants”), especially for patients on dabigatran, which is primarily cleared renally.
Patients with liver disease and coagulopathy
Patients with chronic liver diseases have a delicate balance between procoagulant, anticoagulant, and fibrinolytic systems; loss of this balance may result in haemorrhage or thrombosis depending on their concomitant risk factors. 31 The fragility of this balance and limitations of coagulation tests to accurately reflect bleeding risk increase the complexity of treating VTE in these patients.32
LMWH monotherapy can be considered for these patients. 33 Although DOACs such as apixaban, edoxaban, and rivaroxaban can be used for patients with Child Pugh-A cirrhosis, they are contraindicated for patients with liver disease and coagulopathy. While warfarin is not contraindicated in patients with liver disease and coagulopathy, it is less suitable as the INR may not accurately reflect antithrombotic effect.34
Duration of treatment
Continue anticoagulation for at least three months to prevent thrombus extension and VTE recurrence for the general population (including patients with renal impairment, or liver disease and coagulopathy). A shorter duration of four to six weeks has been shown to double the risk of recurrent VTE compared to a treatment duration of at least three months, and may be insufficient for active treatment aimed at suppressing the acute episode of VTE.34 Treatment beyond three months may be needed for some patients, especially those at increased risk of VTE recurrence. The risk of VTE recurrence depends on the presence and nature of provoking factors (see Figure 2).35,36 Unprovoked VTE has a higher risk of recurrence than provoked VTE (see Figure 2) and may require extended treatment if bleeding risks are low or moderate.5
If extending treatment, use the same anticoagulant unless there are reasons for switching, for example, from a DOAC to warfarin if renal function deteriorates (see Supplementary guide “Switching between anticoagulants”).
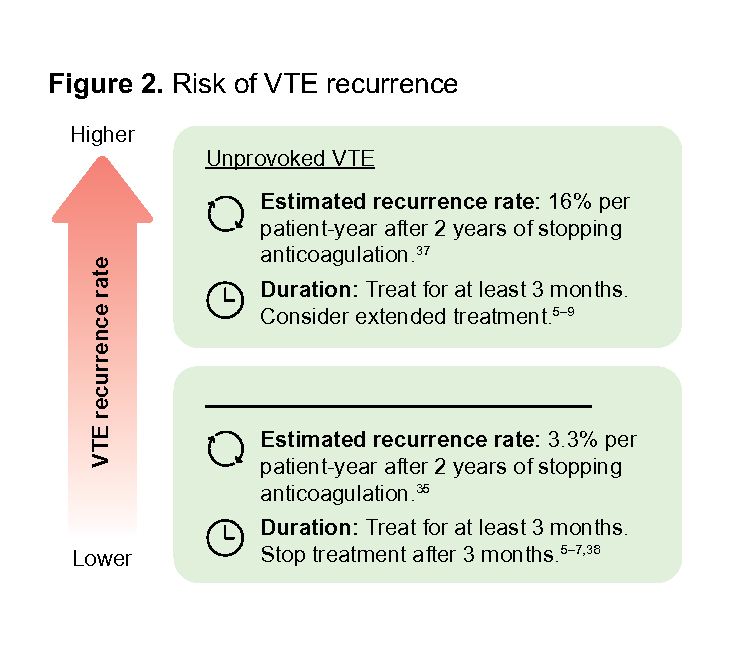
Figure 2. Risk of VTE recurrence
Shared decision-making: As extended treatment usually implies that anticoagulation will continue indefinitely, assess and discuss the risks and benefits of extended treatment with the patient. For patients with first unprovoked proximal DVT or PE wishing to stop anticoagulation after three months, consider low-dose aspirin unless contraindicated.5–7,9 Aspirin is less effective than anticoagulants, but more effective than no treatment, in preventing VTE recurrence.5–7 Discuss the benefits and risks of stopping anticoagulation and initiating aspirin with these patients. |
Notepad: Frequency of review for patients on extended treatment All patients on extended treatment, including those with cancer, should be reviewed at least once a year and when clinically indicated to assess for any change that may necessitate adjustments in the management (such as the choice or dose of the medication).5,7,9 Check for:
|
Recommendation 3: For patients with cancer needing VTE treatment, use apixaban, edoxaban, rivaroxaban, or LMWH for the initial and treatment phases for at least 6 months; LMWH is preferred if the patient has gastrointestinal cancer.
In Asia, the incidence of VTE is substantially higher in patients with cancer than in the general population, with cancer being a major risk factor.40 Wiithout appropriate anticoagulation, about 3 in 10 patients with active cancer will experience recurrence within a year.41
Apixaban, edoxaban, rivaroxaban, and LMWH are more effective than warfarin for preventing recurrent VTE in patients with cancer.42 Apixaban, edoxaban, and rivaroxaban are also more effective than LMWH in preventing recurrent VTE,42,43 but may have a higher risk of clinically relevant non-major bleeding (CRNMB).a The increase in bleeding risk is seen especially in patients with gastrointestinal cancer using edoxaban or rivaroxaban.44 Based on local expert opinion, apixaban, edoxaban, and rivaroxaban may also have higher bleeding risks in patients with genitourinary cancer.
Consider potential drug interactions with anti-cancer therapies – LMWH is preferred for patients using concurrent anti-cancer medications which have significant drug interactions with apixaban, edoxaban, or rivaroxaban.
Shared decision-making: For patients in whom cancer has progressed, consider their wishes and quality of life before extending treatment. If a LMWH was chosen initially, offer apixaban, edoxaban or rivaroxaban as an acceptable alternative if a patient requires anticoagulation but wishes to stop daily injections after six months.16,45 |
Notepad: Patients who are in cancer remission VTE treatment for patients who are in remission is similar to that for the general population (see Recommendation 2), with the risk of VTE becoming comparable to that of patients without cancer after two years of remission.46 While evidence on treatment duration for these patients is lacking, three to six months is an appropriate starting point for decision-making, to be tailored to the patient’s individual circumstances. |
a The International Society on Thrombosis and Haemostasis (ISTH) defines CRNMB as any sign or symptom of haemorrhage (e.g., more bleeding than would be expected for a clinical circumstance, including bleeding found by imaging alone) that does not fit the criteria for the ISTH definition of major bleeding, but does meet at least one of the following criteria: requiring medical intervention by a healthcare professional, leading to hospitalisation or increased level of care, or prompting a face to face (i.e., not just a telephone or electronic communication) evaluation.47
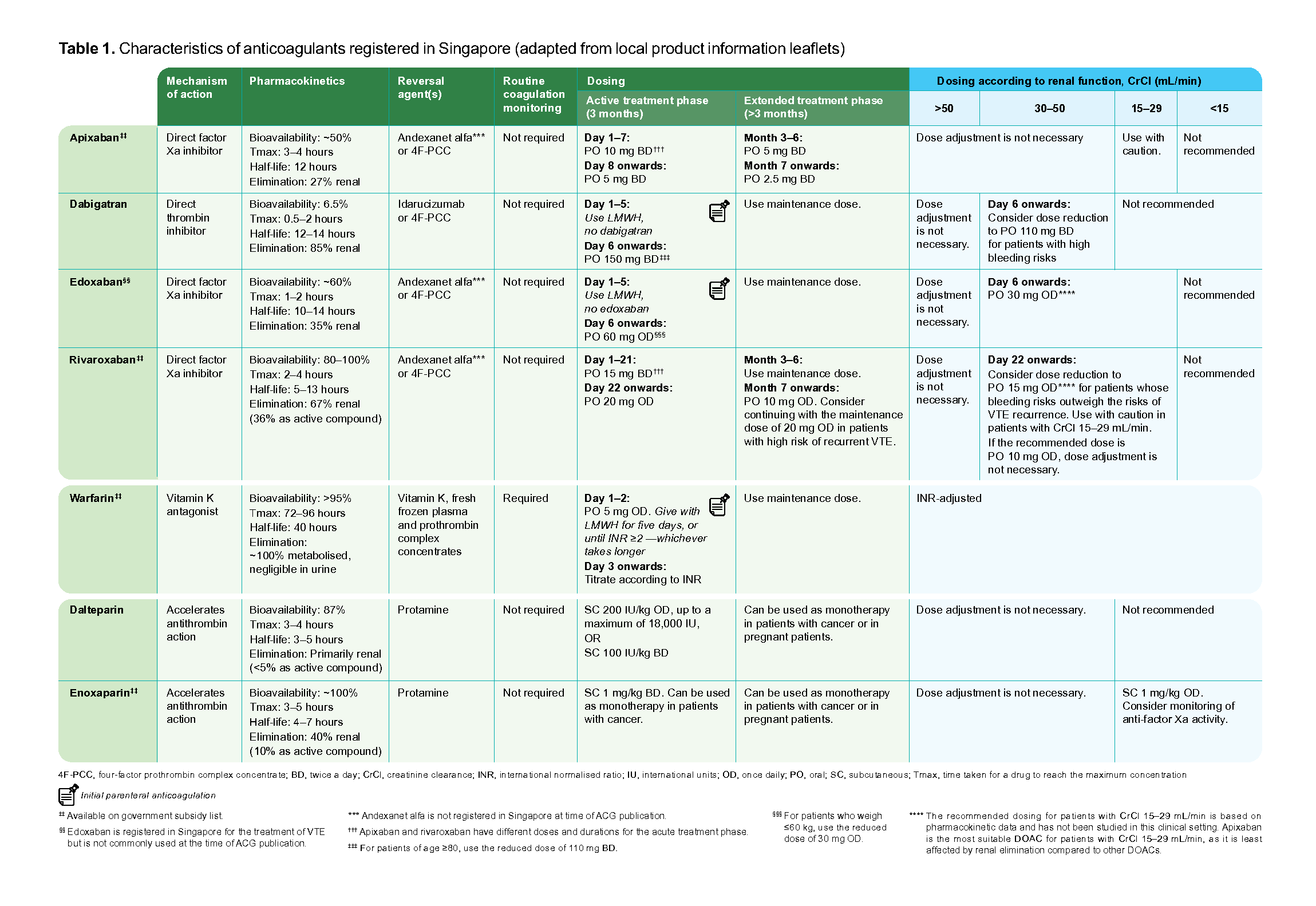
Table 1. Characteristics of anticoagulants registered in Singapore (adapted from local product information leaflets)
Click here for the enlarged image of the above table
Supplementary guides
Expert Group
Lead discussant
Dr Chee Yen Lin, Haematology (NUHS-NCIS)
Chairperson
Clin Prof Ng Heng Joo, Haematology (SGH)
Members
Clin Prof Lee Lai Heng, Haematology (SGH)
Clin A/Prof Tay Jam Chin, Internal Medicine (TTSH)
A/Prof Doreen Tan, Cardiology Specialist Pharmacist (NUS/NUHCS)
Dr Lim Ziliang, Family Medicine (NHGP)
Dr Sim Kok Ping, Family Medicine (Frontier Healthcare)

Feedback
Click here to give us feedback on this ACG.
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Venous thromboembolism — treating with the appropriate anticoagulant and duration. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2024. Available from: go.gov.sg/acg-venous-thromboembolism-goal
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.