
Mild and moderate atopic dermatitis (eczema) – a journey from flare to care ACG
Last updated 19 May 2026
ACE Clinical Guidelines (ACG) provide concise, evidence-based recommendations to inform specific areas of clinical practice and serve as a common starting point nationally for clinical decision-making.
Overview
This ACE Clinical Guideline (ACG) provides guidance on diagnosis, severity assessment and management of mild and moderate atopic dermatitis (AD), including topical and non-pharmacological interventions in adults and children. The ACG also covers proactive therapy, systematic assessment of treatment response, and principles of management of secondary bacterial infection. Supplementary materials are available, including a drug table on topical anti-inflammatories and a photo repository.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Diagnose AD through history taking and clinical examination, focusing on key features such as skin itchiness, dryness, personal or family history of atopic diseases, disease chronicity, lesion morphology and distribution.
Assess AD severity based on extent, frequency and intensity of clinical manifestations, and patient- or caregiver-reported impact on quality of life.
Review potential triggers for AD and advise on how to minimise exposure.
For patients with mild or moderate AD, advise liberal moisturiser use as baseline therapy, and
Prescribe topical corticosteroids (TCS) as first-line anti-inflammatory treatment for active lesions.
If a non-steroidal alternative is required or preferred, consider topical calcineurin inhibitors (as second- line) or topical phosphodiesterase 4 inhibitors (as third-line).
For patients with recurring AD flares (e.g. 2-3 flares/month), prescribe proactive therapy of topical anti-inflammatory treatments to areas of skin prone to flare recurrences.
For patients with inadequate treatment response, assess and address possible factors before modifying treatment.
Do not routinely give oral corticosteroids for AD, except as a short course for:
Rescue therapy for acute, severe flares, or
Bridging therapy to systemic treatment.
For secondary infection of AD, continue patient’s topical anti-inflammatory treatments alongside appropriate antimicrobial agents.
Avoid triple combination products of TCS, antibiotics and antifungals in AD patients with suspected or clinically evident bacterial infection.
Download the ACG and references in PDF
Mild and moderate atopic dermatitis (eczema) – a journey from flare to care (Feb 2026) [PDF]
Mild and moderate atopic dermatitis references (Feb 2026) [PDF]
EtR Framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the major depressive disorder EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Mild and moderate atopic dermatitis EtR framework with summary of findings
Request for a hardcopy
Click here
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guidance (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Atopic dermatitis (AD) is a common chronic inflammatory skin condition characterised by dry skin with recurrent episodes of itching and inflammation. It arises from a complex interplay of genetic predisposition, immune dysfunction and environmental factors, leading to impaired skin barrier function and heightened inflammatory responses.1 The clinical course of AD typically alternates between remission and relapses with symptoms ranging from mild dryness and irritation to severe itch, inflammation and lichenification. In Singapore, AD affects approximately 13.1% of people with higher rates in children (20.6%) than adults (11.1%).2 A substantial proportion of children with AD will continue to have the condition throughout their lives.
This ACE Clinical Guideline (ACG) provides evidence-based recommendations for managing mild and moderate AD to prevent disease progression to more severe cases that require specialist intervention (Figure 1). With appropriate therapeutic interventions and comprehensive care routines, many patients can achieve disease control and maintain healthy, flare-free skin. The focus of this ACG is primary care settings where there are numerous opportunities to provide impactful counselling and early interventions that can significantly improve patient outcomes and quality of life.
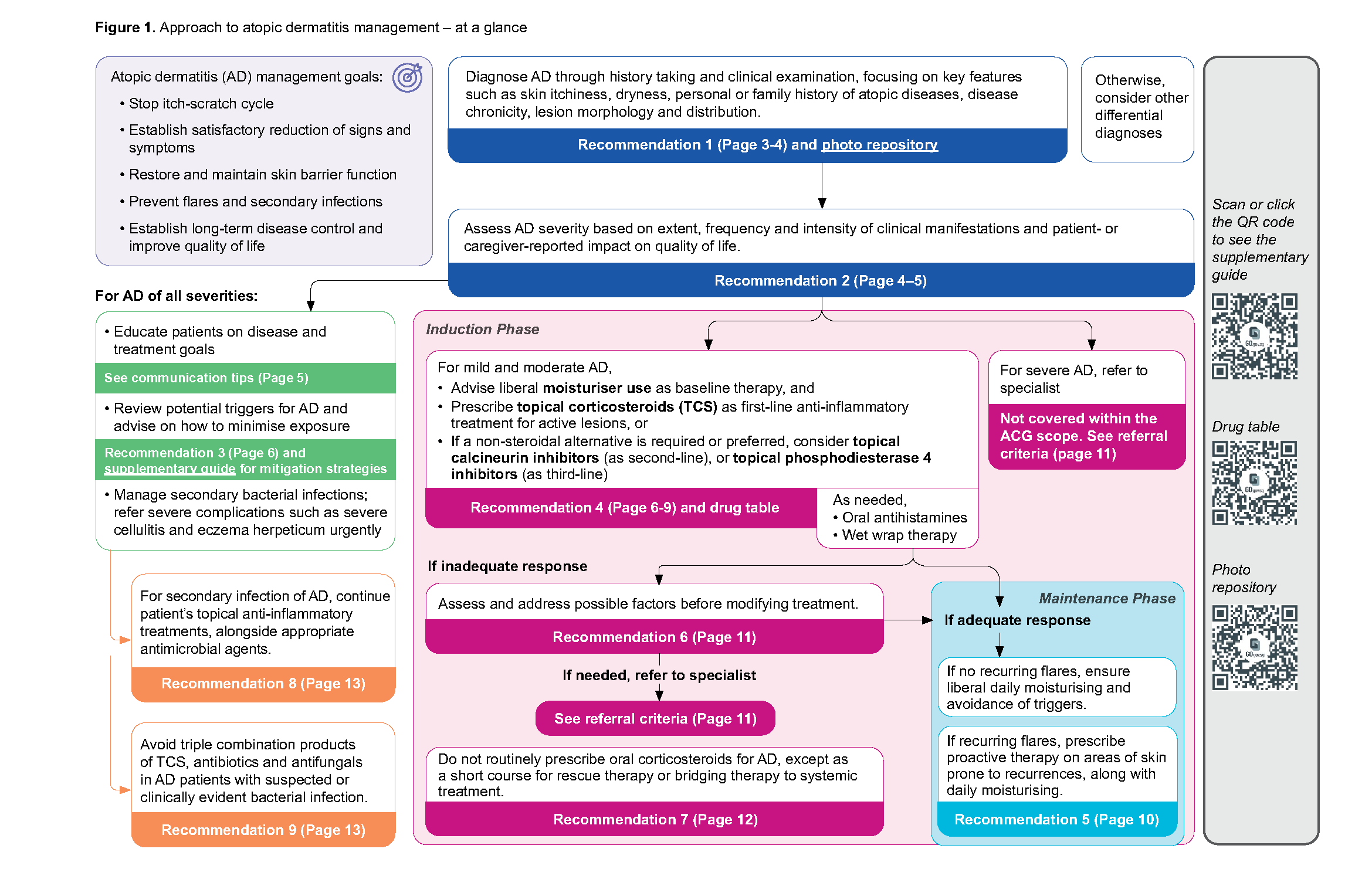
Click here for larger version of the image
Supplementary guide, Drug table, Photo repository
Diagnosis and severity assessment
Recommendation 1: Diagnose AD through history taking and clinical examination, focusing on key features such as skin itchiness, dryness, personal or family history of atopic diseases, disease chronicity, lesion morphology and distribution.
AD is a clinical diagnosis and it relies on recognising key clinical features through careful history taking and physical examination.
History taking should focus on the two most prominent symptoms: skin itch (present in 94% of patients) and dryness (73% of patients). Explore personal or family history of atopic diseases (e.g. asthma, allergic rhinitis and allergic conjunctivitis) which are present in 53% of people with AD.5,6 Identifying individual triggers is important during history taking, as these can vary significantly between patients and may include environmental factors, allergens, stress, or specific irritants (refer to Recommendation 3). Clinicians can establish chronicity by checking age of onset, frequency and duration of previous episodes (if any), their specific characteristics and triggers, followed by examining skin for any signs of long-term inflammation (see ‘chronic lesions’ below).
Notepad: Are blood tests (e.g. sIgE), routine food allergy tests, and skin biopsies necessary for AD diagnosis?
|
Morphology and distribution of AD lesions
The morphology of AD varies with disease chronicity:
Acute lesions: typically present as erythema in lighter skin tones, and may appear violaceous, grey or brown in darker skin tones.1 Lesions may manifest as papules, vesiculopapules and plaques, often accompanied by exudates or crusting.7
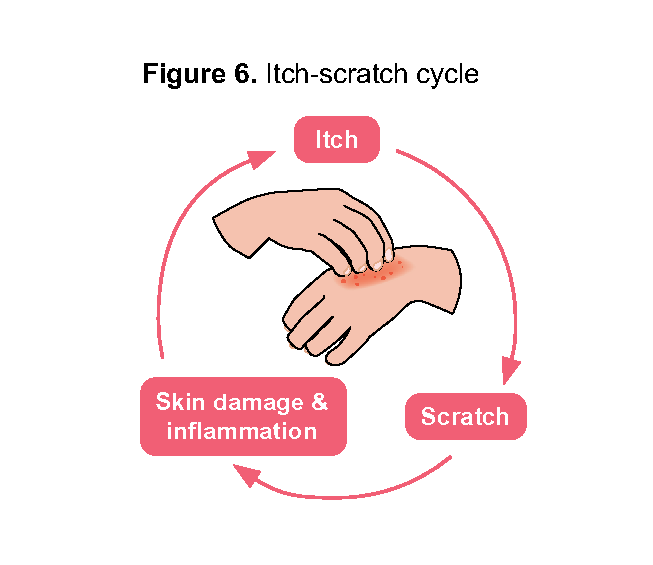
Chronic lesions (developed from persistent scratching): may present as lichenified plaques or prurigo nodules.7 After lesions have healed, patients may present with post inflammatory hyper- or hypopigmentation.6,8
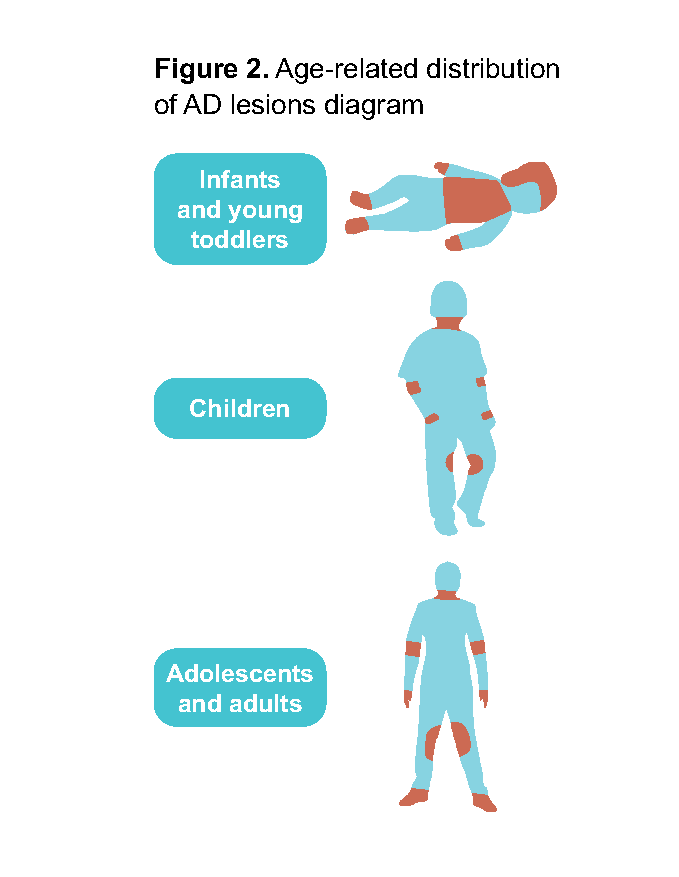
The distribution of lesions typically follows an age-related and symmetrical pattern (Figure 2), though there may be some overlap between age groups:
Infants and young toddlers (under 2 years): scalp and face, commonly spreading to trunk and extremities (often extensor involvement).6,7
Children (2–12 years): neck and flexural areas, with higher prevalence in periorbital and auricular areas, and the ventral aspects of wrists (less cheeks, chin or forehead involvement than infants).5-7
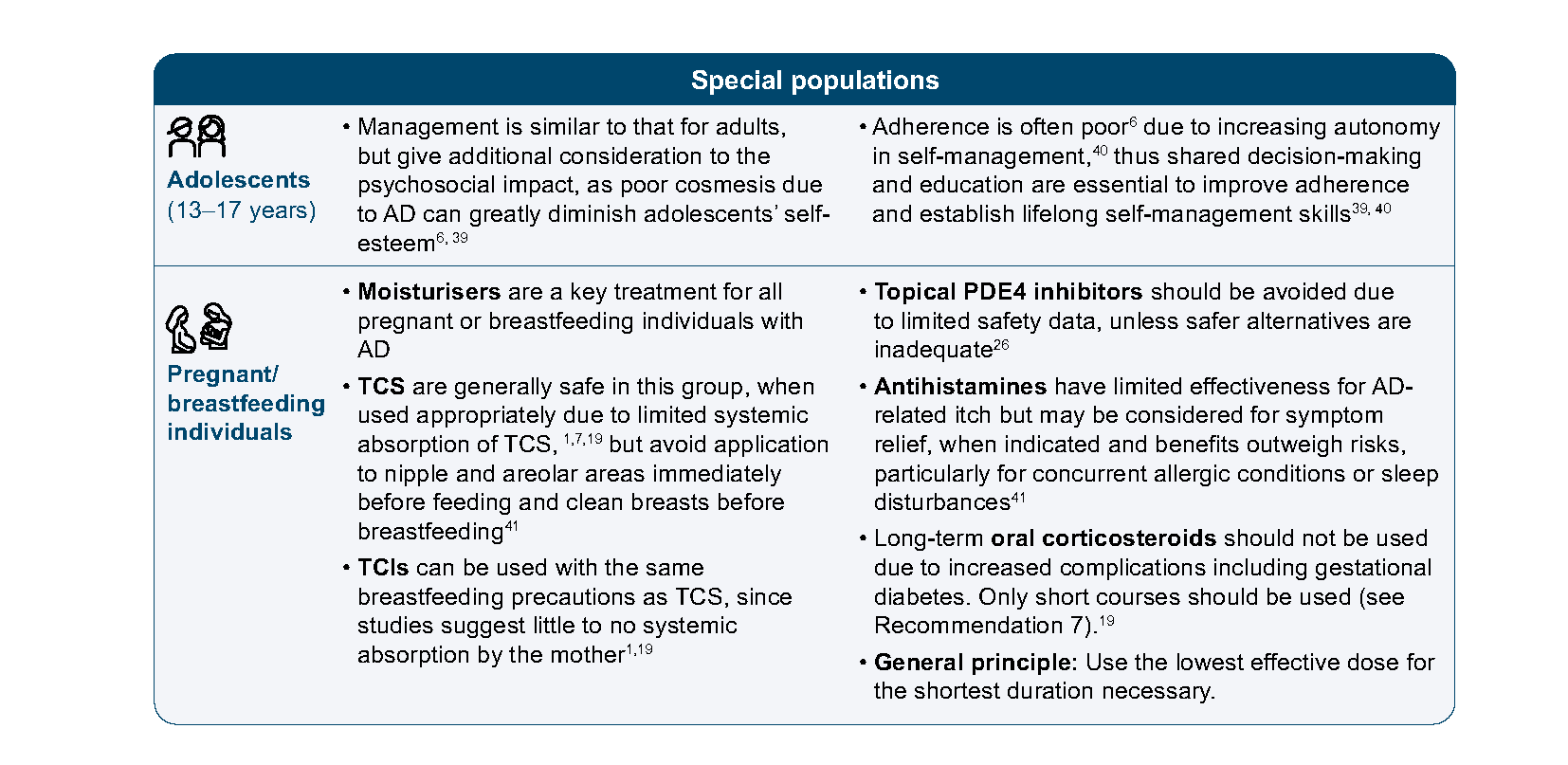
Adolescents (13–17 years) and adults: predominantly flexural areas in addition to face, neck and distal extremities. Distribution may be less typical and appear in localised areas like nipples, hands, or feet.5,6
It is important to note that, AD may present differently in Asian patients compared to non-Asians, including more psoriasiform variants (presenting with clearer demarcation, more prominent scaling and lichenification).8–10 They also show increased prevalence of prurigo nodularis and follicular prominence11, with greater involvement of truncal, extensor, scalp and auricular areas.5
Several conditions can mimic AD and require careful differentiation, including irritant and allergic contact dermatitis, psoriasis, seborrheic dermatitis, scabies or dermatophyte infections.1
Photo repository on common presentation of AD in different skin tones
Diagnostic criteria
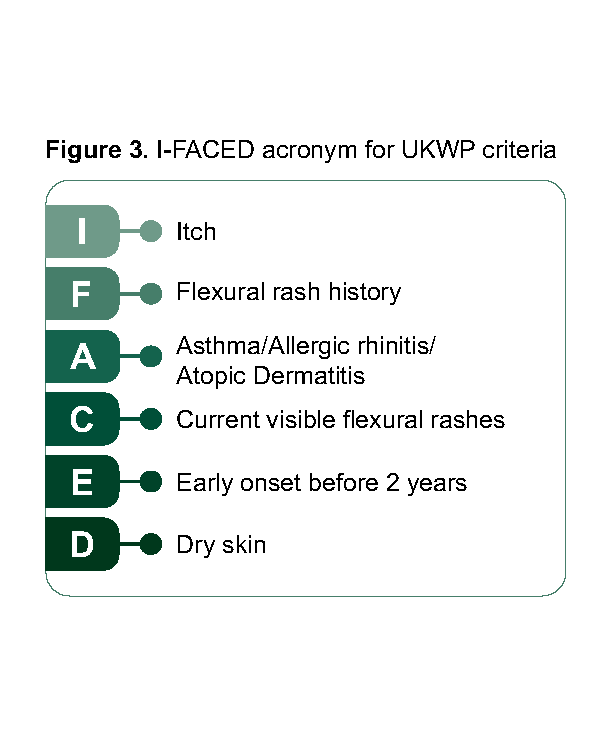
The clinical manifestations of AD can vary widely due to factors such as patient age, disease severity and chronicity, making it difficult to adopt a single set of diagnostic criteria as gold standard in routine clinical practice. Among the most validated and widely cited are the United Kingdom Working Party (UKWP)12–14 and Hanifin and Rajka15 criteria, though both have limitations as detailed in Supplementary guide and should be used in conjunction with comprehensive assessment. Given some practical utility of the UKWP criteria in primary settings, this guideline has developed the I-FACED acronym (Figure 3) to support recall and facilitate application in clinical practice.
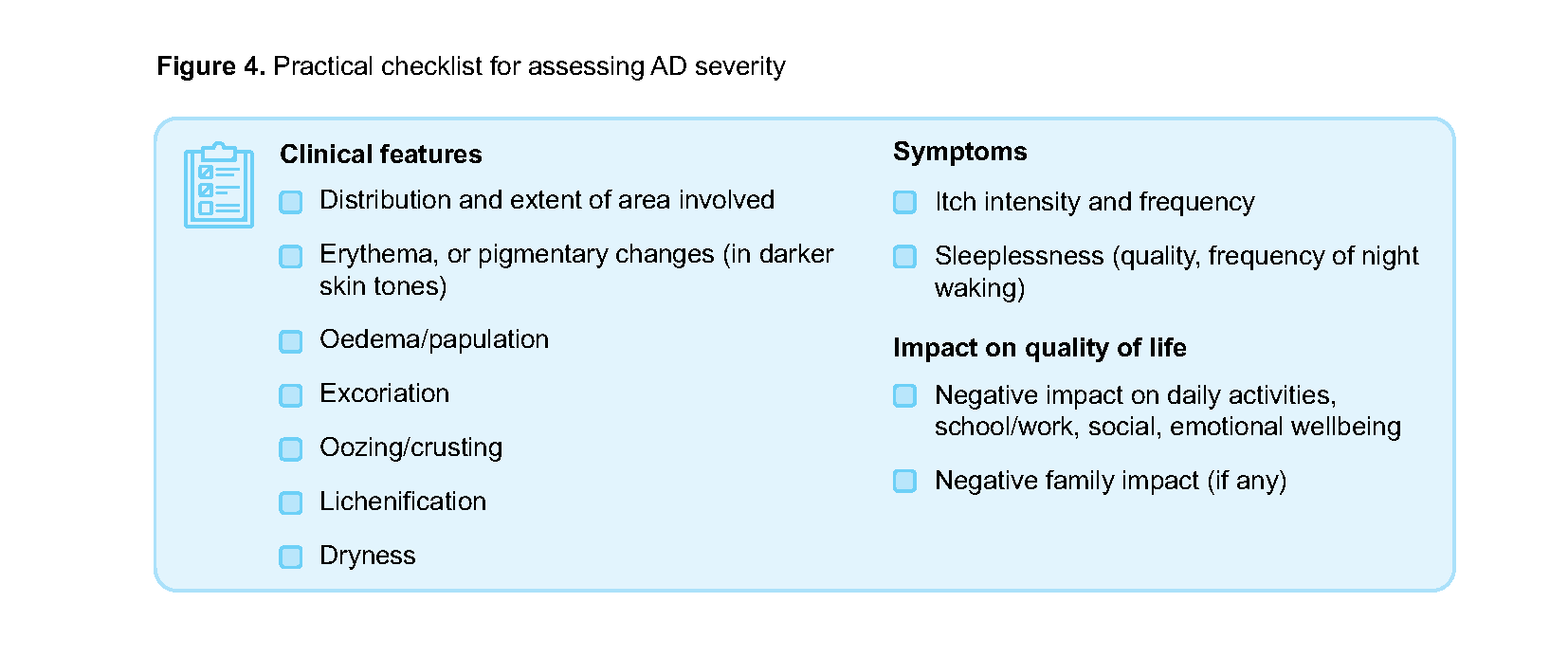
Recommendation 2: Assess AD severity based on extent, frequency and intensity of clinical manifestations, and patient- or caregiver-reported impact on quality of life.
AD severity can be classified using criteria adapted from NICE guidelines16 (Table 1) and comprehensively assessed using a practical checklist derived from validated scoring tools such as EASI, SCORAD and DLQI (Figure 4). Although these tools allow detailed assessment, time constraints and patient burden may limit their routine use. Therefore, they are positioned as optional tools (Supplementary guide) that may be used for detailed assessment when necessary.
Table 1. Adaptation from NICE severity definition
Skin and physical severity | Impact on quality of life | |
|---|---|---|
Mild | Areas of dry skin, infrequent itching (with or without small areas of inflammation) | Little impact on everyday activities, sleep and psychosocial wellbeing |
Moderate | Areas of dry skin, frequent itching, inflammation (with or without excoriation and localised skin thickening) | Moderate impact on everyday activities and psychosocial wellbeing, frequently disturbed sleep |
Severe | Widespread areas of dry skin, persistent itching, inflammation (with or without excoriation, extensive skin thickening, bleeding, oozing, cracking and alteration of pigmentation) | Severe limitation of everyday activities and psychosocial functioning, nightly loss of sleep |
Once severity is assessed, the goals of treatment are to control flares and to maintain remission (Figure 5).
Use clear and empathetic communication when explaining the disease course and management. Setting realistic expectations helps build trust and encourages adherence to treatment plans which improves quality of life for both patients and their caregivers.
Communication tips to educate patients and caregivers
|
Click here to access patient education leaflets on AD: Adults, caregivers of young children, common questions on AD
Avoidance of triggers
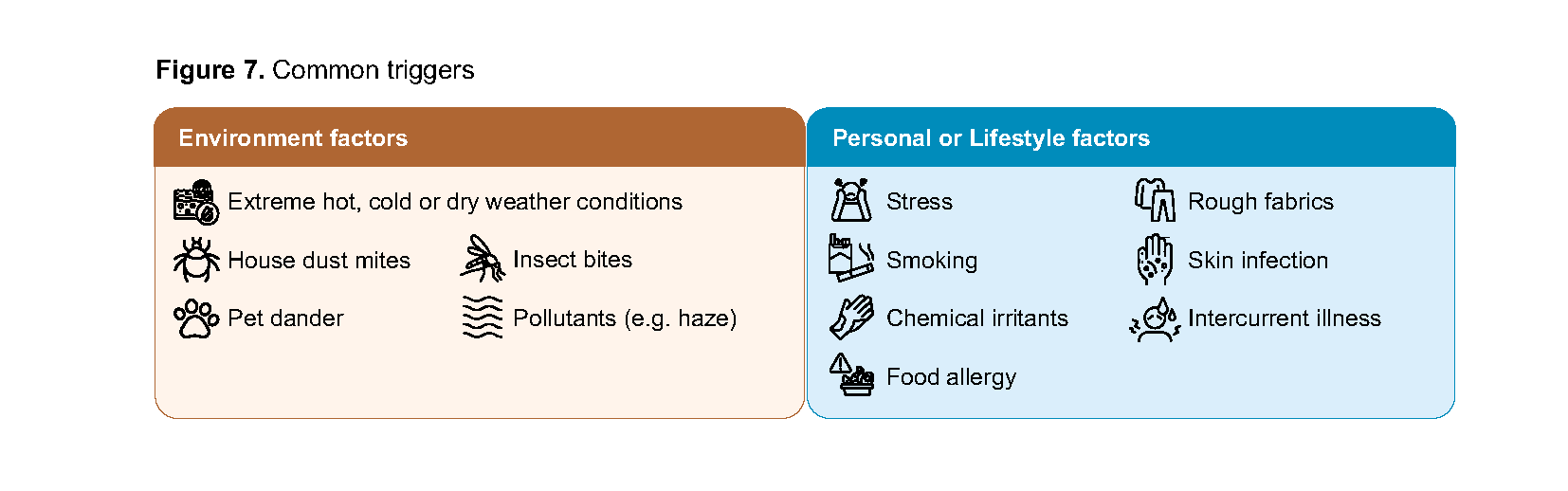
Recommendation 3: Review potential triggers for AD and advise on how to minimise exposure.
Provide tailored counselling to address factors that may trigger or worsen AD. Complete elimination may be feasible for some triggers (e.g. contact allergy), but impractical for others like dust or pollutants, which can typically be minimised rather than avoided entirely. Suspected food allergies require careful evaluation before dietary modifications, to avoid nutritional deficiencies from unnecessary food elimination. Common triggers are outlined below (Figure 7). Refer to Supplementary guide for mitigation strategies.
Pharmacotherapy for mild and moderate AD
Recommendation 4: For patients with mild or moderate AD, advise liberal moisturiser use as baseline therapy, and; 1) Prescribe topical corticosteroids as first-line anti-inflammatory treatment for active lesions 2) If a non-steroidal alternative is required or preferred, consider topical calcineurin inhibitors (as second- line) or topical phosphodiesterase 4 inhibitors (as third-line).
Moisturisers as baseline therapy
Moisturisers are the cornerstone of AD management and recommended for all patients with AD, regardless of disease severity. They are generally well-tolerated, safe and provide multiple benefits such as preventing skin dryness and restoring skin barrier, thereby reducing AD signs and symptoms and decreasing flare frequency.17
Moisturiser prescribing essentials
Selection and Quantity | Application technique and frequency |
|
|
Topical anti-inflammatory treatment for active
AD lesions For active AD lesions or flares, prescribe a suitable topical anti-inflammatory in addition to moisturisers. Topical corticosteroids (TCS) remain the first-line treatment due to their strong and well-established efficacy. The choice of TCS (vehicle and potency), should be tailored to the anatomic site and clinical severity (Table 2), balancing therapeutic benefit with potential local side effects (skin atrophy, striae, telangiectasia).6 Risks of local side effects increases with higher potency TCS, application to thin-skinned areas, occlusion, or long-term continuous use.
Topical calcineurin inhibitors (TCIs) (e.g. pimecrolimus and tacrolimus) are alternatives if non-TCS options are preferred. The topical anti-inflammatory potency of TCIs is broadly comparable to low- and moderate-potency TCS20,21 (see drug table for more details). TCIs are generally well tolerated except for a transient burning or stinging sensation upon application. Despite FDA black box warnings based on high doses of systemic calcineurin inhibitors in animal studies, long-term studies have found no evidence for increased cancer risk in humans.22,23
Topical phosphodiesterase-4 inhibitors (PDE4i), such as crisaborole, are a newer class of non-TCS anti-inflammatory therapy. They work by down-regulating inflammatory cytokine production and reducing skin inflammation, and are effective in reducing AD signs and symptoms compared to placebo.24 Recent head-to-head trials showed moderate potency TCS had greater efficacy in reducing AD signs and symptoms compared to crisaborole,25 while differences between crisaborole and TCIs were not statistically significant25–29 (see drug table and Evidence-to-Recommendation summary of findings). Given the limited evidence on PDE4i efficacy versus TCS and TCIs; similar tolerability issues and cost concerns; and it being less accessible in primary care settings, consider PDE4i when conventional treatments (TCS or TCIs) are unsuitable or not tolerated. Topical PDE4i are generally well tolerated except for a transient burning or stinging sensation.
Drug table of topical anti inflammatories
Table 2. Factors to consider when choosing topical anti-inflammatory treatments
TCS | TCIs* | Topical PDE4i | |
|---|---|---|---|
Age limit | No age limit | Pimecrolimus 1% cream: ≥3 months Tacrolimus 0.03% ointment: ≥2 years; 0.1% ointment: ≥16 years | Crisaborole 2% ointment: ≥3 months |
Sensitive skin areas (face, neck, flexures, groin) | Use low potency for shortest possible duration | Suitable | Suitable |
If patients present with fear or concerns about TCS side effects | Address misconceptions and emphasise safety of appropriate use (see notepad on ‘Addressing steroid phobia’) | Suitable if steroid phobia cannot be resolved | Suitable if steroid phobia cannot be resolved |
Product formulation | Various formulations (solution, lotion, cream, ointment); in tubes and tubs | Cream/ointment; smaller tubes | Ointment; smaller tubes |
Cost/availability | Low cost, generics widely available | Higher cost, less widely available | Higher cost, not widely available |
*Individual medications in the TCIs class are listed according to age limit
Click here to access HealthHub content for patient education leaflets on application technique on:
While disease severity, patient age and anatomical site (Table 3) are useful for guiding treatment selection, clinicians should also consider other patient factors, treatment history, cost and availability. Clinicians may refer to the comparative efficacy drug table in conjunction with these recommendations to inform treatment decisions.
Table 3. Initial topical treatment selection guidance
Age | Topical anti-inflammatory | Site | Mild AD | Moderate AD | Severe AD |
|---|---|---|---|---|---|
Adult (>12 years) | TCS (First-line) | Body | Low to moderate potency | Moderate to high potency | High to ultra high potencyc |
Thin skina | Low potency for shortest duration possible | ||||
Non-TCSb (Only if TCS unsuitable) | Any site | Pim / PDE4i | Pim / Tac 0.03 / Tac 0.1 / PDE4i | Tac 0.1 (≥16 years) | |
Children (≤12 years) | TCS (First-line) | Body | Low potency | Moderate potency | High potencyc |
Thin skina | Low potency for shortest duration possible | ||||
Non-TCSb (Only if TCS unsuitable) | Any site | Pim / Tac 0.03 / PDE4i | |||
Mod, moderate; PDE4i, topical phosphodiesterase 4 inhibitor which is currently only crisaborole 2% ointment; Pim, pimecrolimus 1% cream; Tac 0.03, tacrolimus 0.03% ointment; Tac 0.1, tacrolimus 0.1% ointment; TCS, topical corticosteroids
a Thin skin areas include the periorbital region, face, scalp, neck, flexures, and groin.
b Minimum approved ages for pimecrolimus 1% cream is ≥ 3months; tacrolimus 0.03% ointment is ≥2 years; 0.1% ointment is ≥16 years; crisaborole 2% ointment: ≥3 months. Individual medications in the TCIs class are listed alphabetically, not in order of preference.
c While severe AD may initially require the higher potency TCS, the concurrent use of systemic therapies or phototherapy may permit the stepping down to lower potencies as adjunctive therapy, under specialist advice.
Addressing steroid phobia A local qualitative study revealed that most patients with steroid phobia placed great value on their own experiences and expressed the need to be emotionally validated and understood. Many reported deteriorating doctor-patient relationships when their concerns were dismissed.30 Talking points when addressing patients’ steroid phobia:
If steroid phobia persists despite repeated counselling efforts by primary care professionals, consider referring to a dermatologist, particularly in patients with moderate or severe AD. |
Notepad: Topical JAK inhibitors Topical JAK inhibitors such as ruxolitinib are a novel class of non-steroidal topical anti-inflammatory with demonstrated efficacy in reducing AD severity.20 Common side effects include nasopharyngitis and upper respiratory tract infections.31 All JAK inhibitors carry a black box warning due to associations with increased risk of cancer, thromboembolism, adverse cardiovascular events and serious infections. Safety data is available up to 52 weeks, but long-term data beyond this period remains limited.1,31,32 The medication is currently not registered in Singapore for use in AD. |
While topical anti-inflammatories are the main treatment options for AD, other adjunctive therapies exist, although the evidence supporting their effectiveness is generally limited.
Oral antihistamines Oral antihistamines have limited effectiveness as AD-related itch is predominantly driven by non-histamine mediated pathways.33 Studies demonstrate weak antipruritic effects of oral antihistamines (chlorpheniramine, cetirizine, levocetirizine, loratadine, fexofenadine, and hydroxyzine) for AD.34–36 However, they may provide benefits as adjuvant therapy in concurrent urticaria or allergic rhinitis (where histamine plays a key role). Additionally, first-generation antihistamines may be more useful than second-generation antihistamines for patients experiencing itch-induced sleep disturbances due to their more sedating properties, though this benefit must be weighed against potential anticholinergic side effects including drowsiness, dry skin and mouth, urinary retention and increased fall risk.34 |
Wet wrap therapy Wet wrap therapy (WWT) may be considered for patients with moderate or severe AD refractory to standard application of topical treatments. While evidence is limited, studies of WWT suggest some efficacy in improving AD severity.1,37,38 Moisturisers or TCS are suitable topical agents for use with WWT (Table 4). Safety data for the use of TCIs and topical PDE4 inhibitors under occlusion with WWT remains limited, therefore specialist dermatological advice is essential before using these agents in WWT.1,16 Commonly recommended duration ranges from one hour to maximum overnight.1,17 Click here for WWT patient leaflets |
Table 4. Considerations for implementation of WWT
Assessing patients’ suitability for WWT | Suitable for:
| Less suitable for:
Avoid use in:
|
Potential adverse effects | Generally well-tolerated with mild local adverse effects like skin maceration, folliculitis or other skin infections.1,38 Though TCS efficacy increases under occlusion, studies indicated no significantly higher risk of steroid-related systemic adverse effects.38 | |
Resources required | Additional time and nursing support to educate patients or caregivers on proper wrapping techniques and monitoring of adverse effects | |
Recommendation 5: For patients with recurring AD flares (e.g. 2–3 flares/month), prescribe proactive therapy of topical anti-inflammatory treatments to areas of skin prone to flare recurrences.
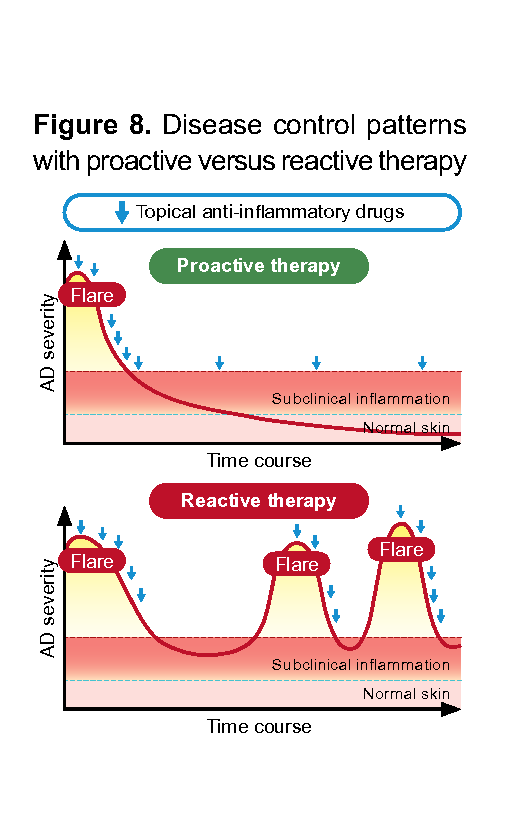
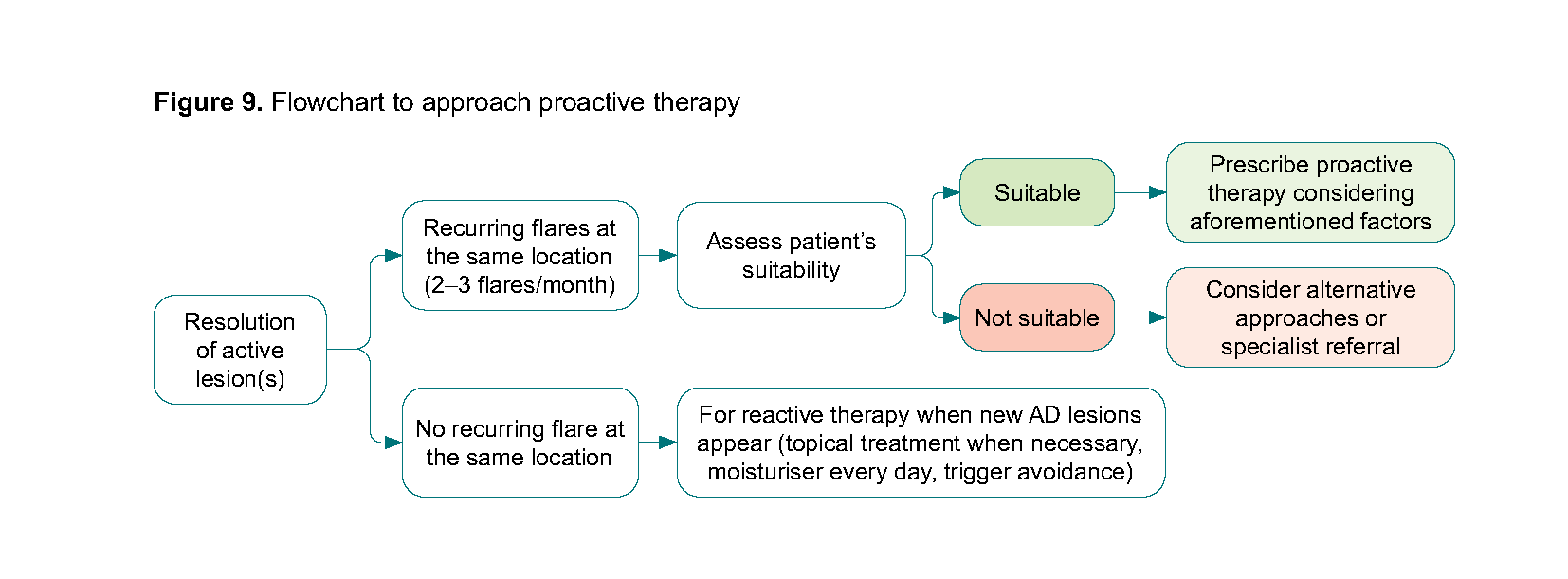
Proactive therapy is a prevention-focused strategy that reduces flare frequency and maintains long-term control by continuing intermittent topical anti-inflammatory treatment on recurrently relapsing skin areas, even after initial AD flare has been controlled. Studies of patients with moderate-severe AD and recurring flares showed that proactive therapy significantly reduced relapse risk with generally low risk of adverse effects, compared to reactive treatment (Figure 8).28,37,42 Based on expert experience, patients with recurring AD flares (2–3 flares per month) affecting the same specific locations, regardless of overall disease severity, will likely benefit from proactive therapy.
Factors to consider when prescribing proactive therapy (Figure 9): |
|---|
Patient suitability assessment:
|
Patient education:
|
Proactive treatment regimen:
|
Monitoring and assessment:
|
Discontinuation of proactive therapy:
|
For patients with moderate or severe AD refractory to topical treatment, phototherapy and systemic options including oral conventional immunosuppressants, oral JAK inhibitors, and monoclonal antibodies have been shown to improve AD severity (no treatment hierarchy implied).45, 46 Patients requiring such therapies should be referred to specialists treating severe AD, such as dermatologists, allergists or relevant specialists.
Notepad: Role of complementary therapies Topical anti-inflammatory treatments remain the mainstay of AD management. Clinicians might be asked about the efficacy of complementary therapies such as probiotics47–49 and polynucleotide injections.50 These therapies currently have limited evidence for routine use in AD treatment. They may incur additional cost without established clinical benefit in AD management and should not replace established topical therapies. Patients wishing to proceed with these complementary therapies should be counselled adequately about the additional costs and limited evidence of clinical benefit. |
Recommendation 6: For patients with inadequate treatment response, assess and address possible factors before modifying treatment.
When evaluating inadequate treatment response, defined as a lack of satisfactory improvement in AD signs, symptoms or impact on quality of life after 2 weeks, clinicians should systematically consider different factors (see below) before modifying treatment.
Confirm diagnosis and exclude complicating factors | Assess treatment-related factors | Assess patient-related factors |
| Assess:
| Assess:
|
Most patients with mild and moderate AD can be effectively managed in primary care.
Consider specialist referral for the following situations:
Uncertain diagnosis (including suspected allergic contact dermatitis with unidentifiable allergen requiring patch testing)
Unsatisfactory response to topical treatments in primary care such as:
Flare persisting for more than 2 to 4 weeks after appropriate treatment
Flares still occurring frequently after 3–6 months of proactive therapy
Significant adverse effects or poor tolerance to topical treatment(s)
Extensive (e.g. >10%) body surface area affected
Significant impact on quality of life (including social or psychological problems)
Severe complications such as skin infections requiring intravenous antibiotics and antivirals (e.g. severe cellulitis, eczema herpeticum), and erythrodermic flare – refer to emergency department
Recommendation 7: Do not routinely give oral corticosteroids for AD, except as a short course for; 1) Rescue therapy for acute, severe flares, or 2) Bridging therapy to systemic treatment
Oral corticosteroids (OCS) are not recommended for routine use in the mild and moderate management of AD. Although they provide rapid symptom relief, benefits are short-lived, and disease activity typically rebounds after discontinuation.1,19,51 Long-term or repeated use carries significant risks such as infection, hypertension, glucose intolerance, weight gain, gastritis, reduced bone mineral density, and adrenal suppression.52 Reliance may also delay the initiation of more appropriate and effective long-term treatment.
OCS is strongly discouraged in children due to the additional risk of growth retardation.52,5
Short courses of OCS may be considered for rescue therapy during acute, severe flares - defined as episodes with widespread inflammation, persistent itching and significant impairment of quality of life (following NICE severity definition) - or as bridging therapy while initiating slower-acting systemic treatments.51,54 When prescribed, clinicians must communicate temporary benefits and risks through shared decision-making, emphasising adherence to prescribed duration and need for effective long-term alternatives.
Practical prescribing considerations for OCS
|
OCS, oral corticosteroids; OD, once daily
Management of AD with secondary bacterial infection
Patients with AD are predisposed to skin infections due to multiple factors such as skin barrier. skin barrier disruption, inflammation, bacterial colonisation and dysbiosis of skin flora.55 Scratching also disrupts the skin barrier and may allow entry of pathogens. It may be challenging to distinguish between an AD flare and infected AD as both can present with erythema, weeping, and worsening skin symptoms.56
Notepad: Recognising AD with secondary bacterial infection AD with secondary bacterial infection typically presents as lesions with honey-coloured crusting, oozing or weeping, pain, failure to respond to standard AD therapy or rapidly worsening AD.56 Systemic signs such as fever and malaise may indicate more severe infection.56 Most cases can be managed similarly to impetigo. Less commonly, secondary cellulitis or skin abscesses may develop and require more intensive treatment.55 Click here to access photo repository on secondary infection of AD |
Bacterial infection in AD is mostly commonly caused by Staphylococcus aureus (S. aureus), followed by Streptococcus pyogenes (S. pyogenes).56 Skin swabs are not necessary in most cases, as bacterial colonisation is common in AD patients regardless of infection status,57 and routine swabbing of AD patients with suspected infection could lead to inappropriate antibiotic prescribing.56 If infection worsens, consider a skin swab to check for other causative organisms or resistant strains.19,56
Recommendation 8: For secondary infection of AD, continue patient’s topical anti-inflammatory treatments alongside appropriate antimicrobial agents.
For this ACG’s management of secondary bacterial infection of AD, antimicrobial agents refer to either antiseptics or antibiotics.
In general, the patient’s anti-inflammatory treatments (TCS or TCI) should be continued alongside appropriate antimicrobial agents during episodes of infected AD, including severe viral infections such as eczema herpeticum.19,56 Both TCS and TCIs have been shown to reduce S. aureus colonisation, increase microbial diversity, and reduce scratching by managing the underlying inflammation.55 Evidence of effectiveness for antimicrobial agents (antibiotics or antiseptics) in combination with topical anti-inflammatories in infected AD remains limited. For topical antibiotics, studies show significant reduction in S. aureus isolation rates, but only modest improvements over TCS alone in overall disease signs and symptoms.58
Clinicians should weigh the need for antimicrobial treatment against the risk of contributing to antimicrobial resistance. AD flares can clinically mimic skin infection,56 making it difficult to distinguish between inflammatory f lares and actual bacterial infections. As such, infections may be incorrectly diagnosed when none is present, resulting in unnecessary antimicrobial prescribing. Clinicians must carefully assess whether an infection is truly present before prescribing antimicrobials.
When the decision to treat as a secondary AD infection has been reached:
Topical antiseptics may be used to reduce microbial load, although resistance may develop with prolonged use. Evidence supporting their use in infected AD is limited and derived from a few small trials.17, 21, 58 Staphylococcus resistance to antiseptics is emerging (to triclosan, and to a lesser extent to chlorhexidine and octenidine, whilst povidone-iodine has limited evidence of antimicrobial resistance).59,60 Nevertheless, antiseptic resistance is less common than antibiotic resistance.
Topical antibiotics, if indicated, should be used judiciously. When antibiotics are necessary, select narrow spectrum agents with appropriate duration (e.g. 5 to 7 days); widespread, prolonged or indiscriminate antibiotic use escalates antibiotic resistance. Global surveillance data indicate only 80% fusidic acid susceptibility and 98% for mupirocin.61 For mild impetiginised AD, topical fusidic acid may treat S. aureus and S. pyogenes skin infections, while topical mupirocin should be reserved for confirmed methicillin-resistant S. aureus (MRSA) where infection has worsened.56
Dual combination creams (TCS plus suitable topical antimicrobial) may reduce treatment regimen complexity and support patient adherence.
Systemic antibiotics are indicated for severe or widespread infected AD, or when patients are systemically unwell.56
If the response to initial treatment course is suboptimal and symptoms persist, reassess the diagnosis and management plan, and consider escalating care, such as a skin swab to guide targeted antibiotic choice, or referral.56
Notepad: Differences between antiseptics and antibiotics Antiseptics are topical agents with broad-spectrum activity against bacteria, fungi and some virus through non-specific mechanisms.36 They have a lower risk of developing resistance due to multiple mechanisms of action.59 Examples are benzalkonium chloride, clioquinol, chlorhexidine, hydrogen peroxide, povidone-iodine, octenidine and triclosan. Antibiotics can be delivered in many ways (orally, intravenously, topically, etc) and specifically target bacteria through targeted molecular mechanisms to kill (bactericidal) or inhibit growth (bacteriostatic).36 This specificity of action makes bacterial resistance development more likely.59 |
Recommendation 9: Avoid triple combination products of TCS, antibiotics and antifungals in AD patients with suspected or clinically evident bacterial infection.
Products containing a combination of TCS, antibiotics and antifungals should be avoided:
Inappropriately high potency TCS: The TCS components in locally available products, such as betamethasone dipropionate 0.05% are typically high-potency formulations. This may be unnecessarily potent for many AD patients, increasing the (avoidable) risk of local side effects such as skin atrophy, especially without proper monitoring.
Limited role of gentamicin: Products containing aminoglycosides like gentamicin, have poor penetration and limited bactericidal activity against S. aureus and S. pyogenes, without synergistic combinations with beta-lactams.64,65 As such, they are not suitable as a monotherapy for treating common gram-positive skin infections.
Risk of contact dermatitis: Topical aminoglycosides commonly found in these combinations, such as gentamicin and neomycin, have been shown to cause contact dermatitis in some individuals, potentially worsening the existing skin condition.64, 65
Unnecessary antifungal component: Most bacterial infections in AD do not require concurrent antifungal treatment. Their use potentially exposes patients to unnecessary medication, given the limited evidence supporting topical antifungals in AD patients.66
ACG supplementary guides
Drug table on topical anti-inflammatories (Feb 2026) [PDF]
Atopic dermatitis photo repository (Feb 2026) [PDF]
Expert group
Chairpersons
Clin Assoc Prof Mark Koh Jean Aan, Dermatology (KKH)
Dr Michael Warren Lim, Family Medicine (NUP)
Members
Clin Assoc Prof Chan Poh Chong, Paediatrics (NUH)
Dr Roland Chu, Dermatology (Loke Skin Clinic)
Dr Goh Tze Chien Kelvin, Family Medicine (Northlink (Woodlands) Clinic)
Ms Helena Hor, Pharmacy (Watson’s Personal Care Stores Pte Ltd)
Ms Huang Xiaoling, Pharmacy (NSC)
Dr Mohana D/O Rajakulendran, Paediatrics (Petite Practice)
Adj Assoc Prof Nisha Su Yien Chandran, Dermatology (NUH)
Dr Suraj Kumar, Family Medicine (Drs Bain & Partners)
Dr Tan Hwee Mian Jane, Family Medicine (SHP)
Ms Wang Yu Yan, Nursing (NSC)
Dr Nelson Wee, Family Medicine (Silver Cross Medical)
Dr Yeap Youwen, Family Medicine (NHGP)
Dr Yew Yik Weng, Dermatology (NSC)
For more information on the Expert Group composition and other details, click here.

Feedback
Click here to give us feedback on this ACG.
Other related resources
Patient education aid – common questions on atopic dermatitis (Feb 2026) [PDF]
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Ministry of Health, Singapore. 2026. Available from: go.gov.sg/acg-ad Agency for Care Effectiveness (ACE). Mild and moderate atopic dermatitis (eczema) – a journey from flare to care. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2026. Available from: go.gov.sg/acg-ad
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.