
Foot assessment in patients with diabetes mellitus ACG
Last updated 26 May 2026
Published on 06 Jun 2019
Last Updated on 08 Aug 2024
Overview
This ACE Clinical Guideline (ACG) highlights the importance of regular foot assessment in patients with diabetes mellitus to identify and manage risk of developing diabetic foot ulcers. The ACG offers evidence-based recommendations on assessing active diabetic foot conditions, components of foot assessment, management based on risk stratification findings (including frequency of review and referral needs), and patient education.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Check for presence of active diabetic foot conditions in all patients with diabetes mellitus.
Use foot assessment findings to determine the risk of developing a diabetic foot ulcer, corresponding review frequency, and need for referral.
Educate all patients with diabetes mellitus regularly on lifestyle, regular foot assessment, foot care and appropriate footwear, to reduce risk of developing diabetic foot ulcers.
Download the ACG and references
Foot assessment in patients with diabetes mellitus (Aug 2024) [PDF]
Foot assessment in people with diabetes mellitus references (Aug 2024) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional
Introduction
Diabetes mellitus is a major global health concern. It is associated with macro- and microvascular complications, including DFU. DFU precede about 85% of lower extremity amputations1 and are associated with mobility loss, poorer quality of life, and decreased overall productivity.2 In Singapore, almost five lower extremity amputations occur every day on average in patients with diabetes mellitus.3 Regular foot assessment is recommended to identify and manage the risk of developing DFU, with the frequency of assessment depending on patient’s risk category.4–11
In Singapore, almost five amputations occur every day on average in patients with diabetes mellitus.
About 85% of amputations could be avoided through regular foot assessment.
Foot assessment
Recommendation 1: Check for presence of active diabetic foot conditions in all patients with diabetes mellitus.
Foot assessment for patients with diabetes mellitus begins with checking for presence of active diabetic foot conditions, such as infection, acute Charcot neuro-osteoarthropathy, or limb ischaemia. If present, immediate treatment or referral may be warranted depending on the type of condition identified (see Figure 1 below). In patients without active diabetic foot conditions, assess the patient’s risk of developing DFU and stratify accordingly (see Recommendation 2).
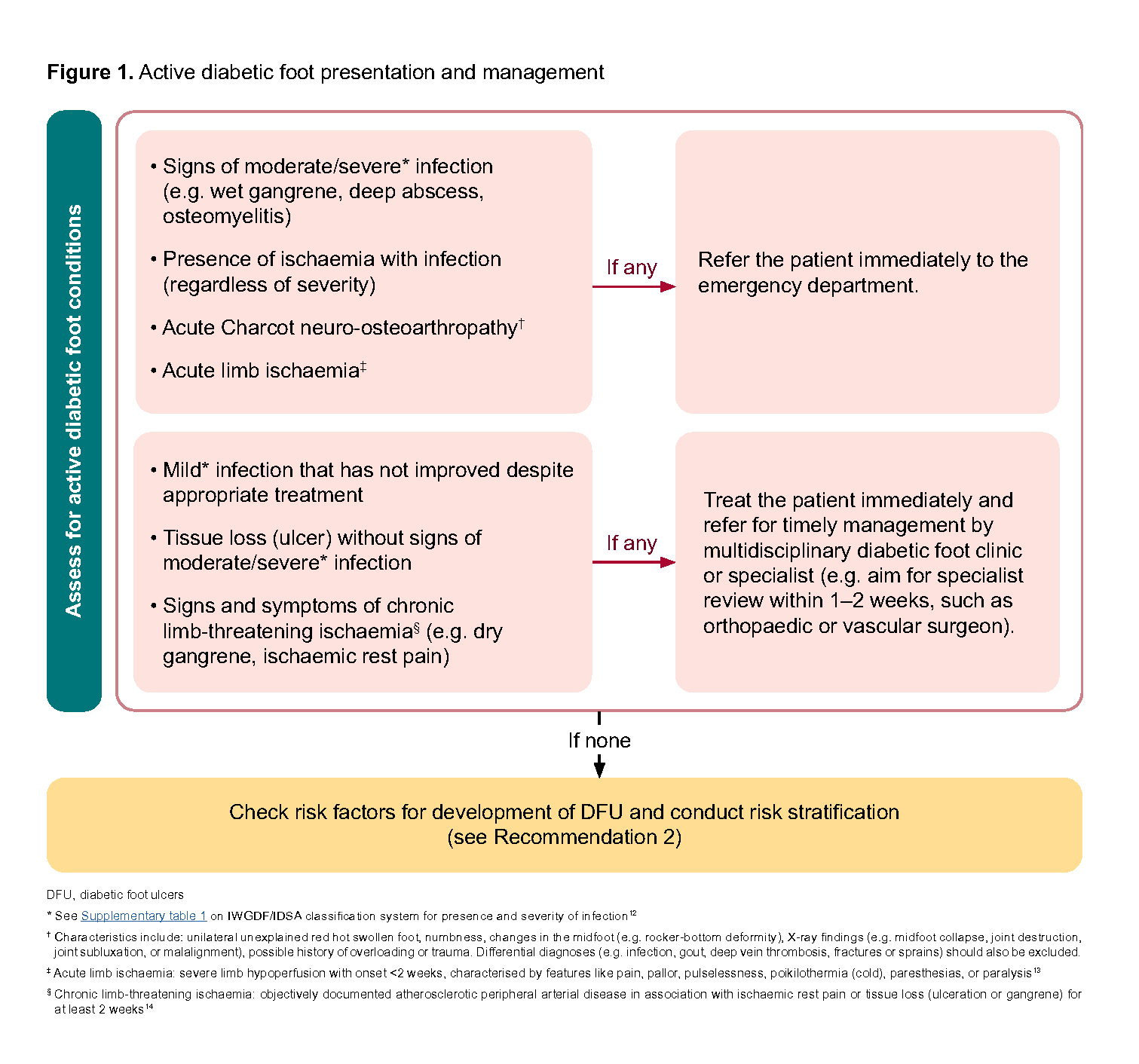
Figure 1. Active diabetic foot presentation and management
Recommendation 2: Use foot assessment findings to determine the risk of developing a diabetic foot ulcer, corresponding review frequency, and need for referral.
A comprehensive foot assessment includes medical history, physical examination of the feet (including tests), symptoms assessment, and review of other risk factors for the development of DFU. Foot assessment findings are used to categorise a patient’s risk of developing DFU and inform risk-based management decisions, such as referral and frequency of review.
Risk stratification
Assess patients without active diabetic foot conditions for factors that increase their risk of developing DFU and manage according to their assigned risk category.
Factors used for stratifying risk of developing DFU are: 4–11
• Previous foot ulcer or amputation
• Estimated glomerular filtration rate persistently <15 ml/min/1.73m2 over at least three months (including patients on dialysis)
• Clinical findings (including objective tests) of:
Callus
Deformity
Peripheral arterial disease (PAD)
Neuropathy
See Figure 2 for details of factors contributing to risk stratification, risk categories for the development of DFU, and associated actions (e.g. review frequency). Figure 3 summarises the steps involved in conducting a foot examination and performing main objective tests.
Notepad: Practice point If any of the factors contributing to risk of developing DFU cannot be assessed reliably to inform risk stratification, assume the risk factor to be present. Example: a patient with cognitive impairment who is unable to engage in objective tests for neuropathy can be assumed to have the neuropathy risk factor for risk stratification. |
Other factors of foot assessment
While not directly contributing to risk stratification, other factors inform overall management needs, referral requirements, and patient education. These include:
• Glycaemic control
• Smoking
• Foot care and footwear
• Skin integrity (e.g. corns, callus requiring intervention, blisters)
• Toenail condition (e.g. ingrown toenail, moderate fungal nail)
• Lacking caregiver support or inability to self-care (e.g. significant arthritis, cognitive or visual impairment, inability to maintain personal hygiene or self-check feet for problems)
Notepad: Importance of comprehensive management Foot assessment is only one component of diabetes management and its associated conditions (refer to type 2 diabetes mellitus management ACG). For example, patients with PAD require comprehensive cardiovascular management including optimisation of glycaemic control, blood pressure (refer to hypertension ACG), and lipid profile (refer to lipid management ACG), smoking cessation (if applicable), and initiation of antiplatelet therapy, if indicated. ACGs on other areas of diabetes management and relevant associated conditions can be found here under “Related ACGs”. |
Referral
Referral to specialists, podiatrists, or other healthcare professionals may be required based on findings from foot assessment. Patients who are stratified to be at moderate or high risk of developing a DFU could be referred if additional assessment or intervention is needed.
Patients lacking self-care ability (e.g. significant arthritis, cognitive or visual impairment, inability to maintain personal hygiene or self-check feet for problems) or have limited/absent caregiver support may require referral to relevant services (e.g. primary care nursing, podiatry or social services) where available.
Additional considerations for referral are:
Clinical findings | Referral speciality |
|---|---|
Deformity • Pain or functional impairment due to significant deformity • Charcot neuro-osteoarthropathy as suggested by clinical or X-ray findings (e.g. midfoot collapse, joint destruction, joint subluxation, or malalignment) | Consider referring to orthopaedics** |
PAD • Clinical findings that may benefit from further assessment or vascular intervention, comprising of: - Objective tests (e.g. TBPI or ABPI) - Symptoms (e.g. vascular claudication, ischaemic rest pain, ulcer) | Consider referring to vascular especially if symptomatic** |
Neuropathy • Severe or worsening symptoms (e.g. pain despite appropriate analgesia) in typical diabetic neuropathy • Atypical features suggesting non-diabetic neuropathy or atypical forms of diabetic neuropathy (e.g. acute onset, asymmetrical distribution, motor deficits worse than sensory deficits, or non-length dependent features such as involvement of both hands and feet at the same time or hands prior to involvement of feet15) | Consider referring to neurology** |
Skin/nails • Pre-ulcerative skin lesion (e.g. corn or callus requiring podiatric treatment, blister or fissure, tinea pedis) • Pathological toenail (e.g. ingrown toenail, moderate fungal nail) | Assess need for podiatry referral†† |
** Can be guided by referral pathways to the relevant specialties or services as per institution protocols, where available
†† Low-risk or stable skin and toenail conditions of the foot may not need referral to podiatry. Please see “Podiatry referral criteria” developed as part of the HealthierSG care protocol on diabetes mellitus for more details (see Diabetes Mellitus HealthierSG care protocol) or scan QR code on the right.
Click here to the right for podiatry referral criteria in the diabetes mellitus HealthierSG care protocol
Review
Conduct comprehensive foot assessment at least once a year for all patients with diabetes mellitus. Carry out more frequent review for patients in the moderate-risk (every six months) and high-risk categories (every three to four months), focusing the assessment on factors that contributed to that risk classification. For example, for a patient with a moderate risk of developing DFU because of thick callus requiring treatment, review after six months for any change in status of callus and then again at one year for a comprehensive foot assessment.
Each review is also an opportunity for the healthcare professional providing care at that point (e.g. nurse, doctor, or podiatrist) to:
• Visually inspect the feet for any visible lesion
• Check on the patient’s understanding of good practices (see Recommendation 3), and
• Reinforce the importance of foot care and appropriate footwear (see Recommendation 3)
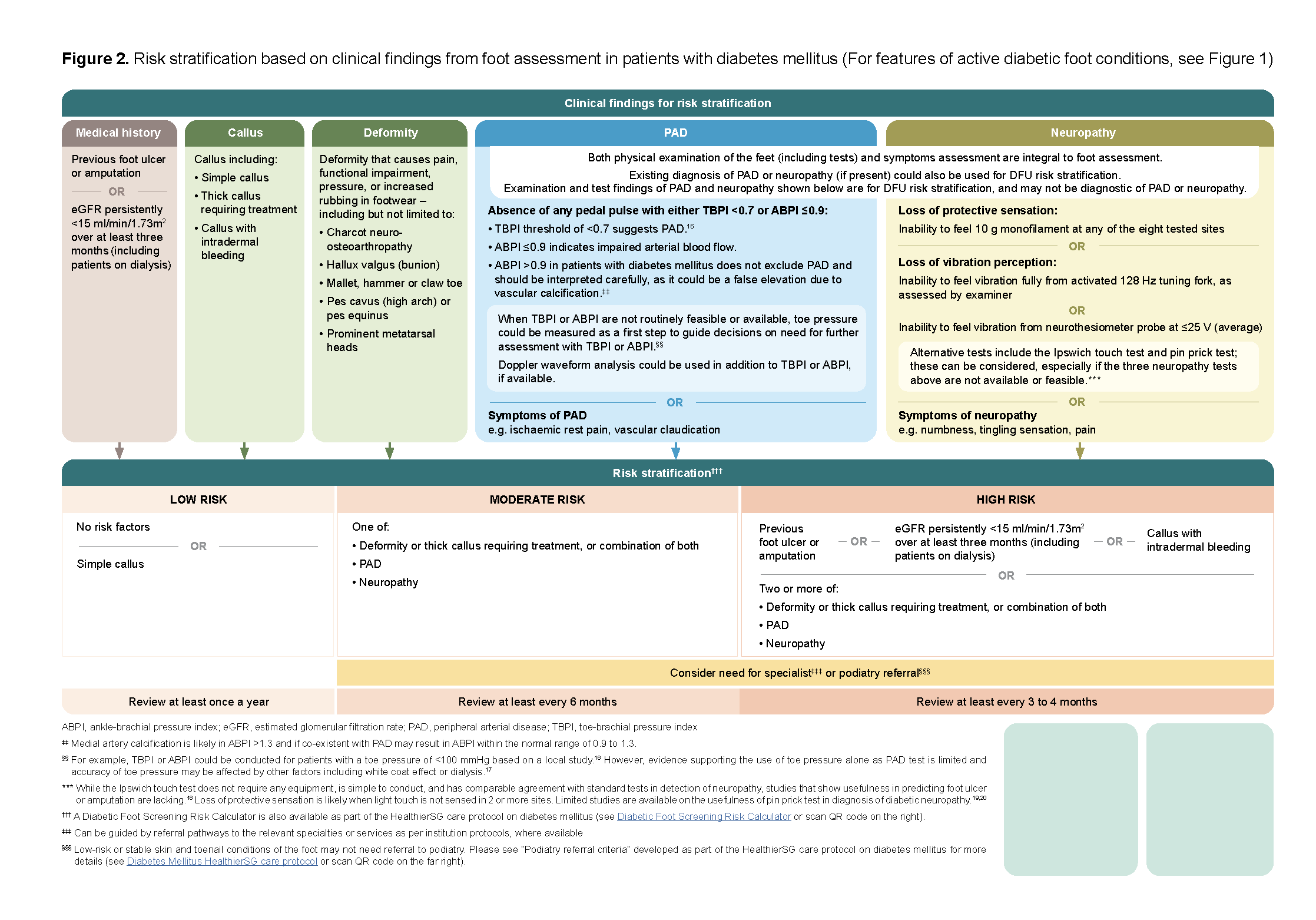
Figure 2. Risk stratification based on clinical findings from foot assessment in patients with diabetes mellitus (For features of active diabetic foot conditions, see Figure 1)
Click here for larger version of the image
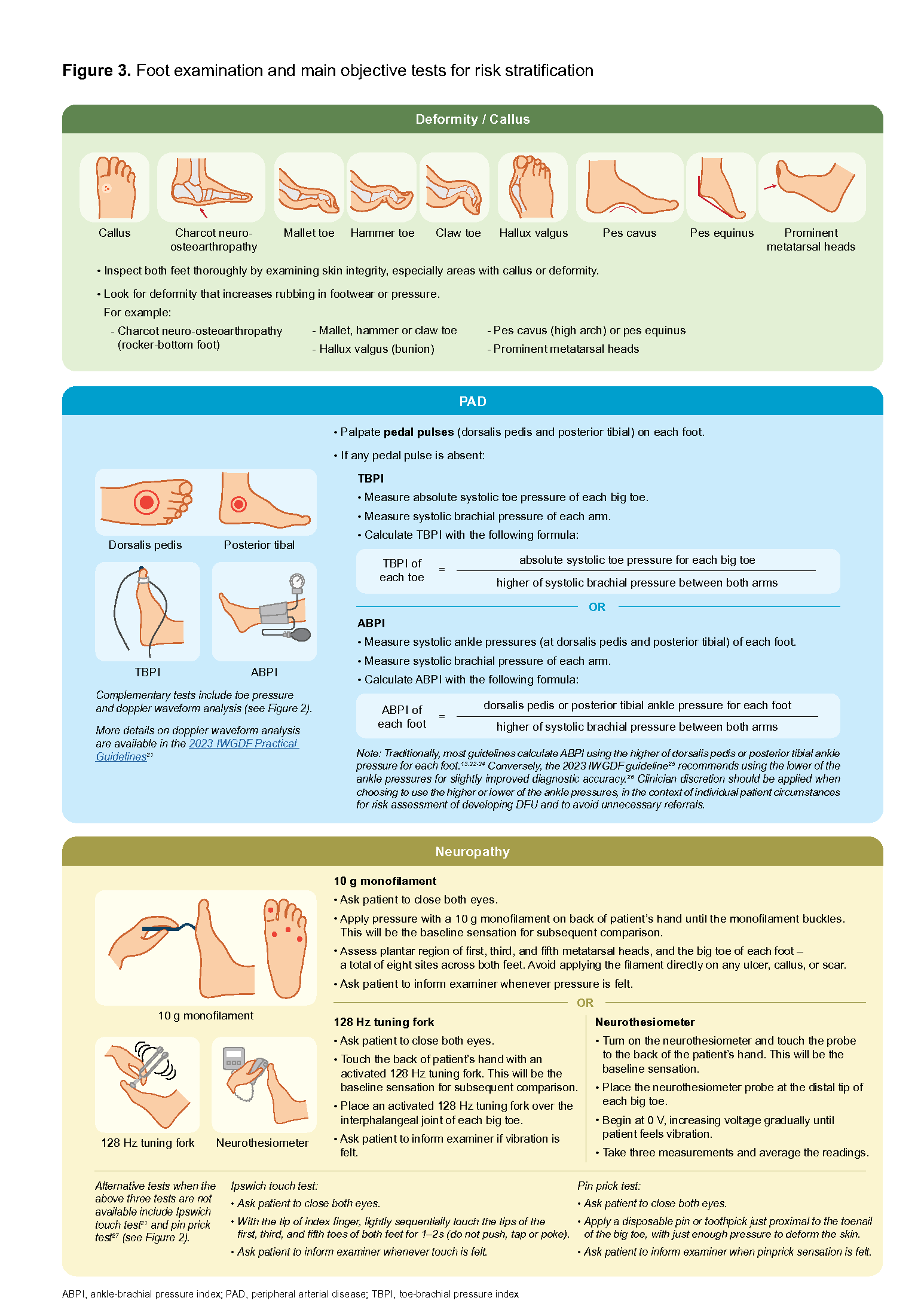
Figure 3. Foot examination and main objective tests for risk stratification
Click here for larger version of the image
Patient education
Recommendation 3: Educate all patients with diabetes mellitus regularly on lifestyle, regular foot assessment, foot care and appropriate footwear, to reduce risk of developing diabetic foot ulcers.
Advise patients on sustained lifestyle interventions to maintain optimal glycaemic control, such as eating a healthy balanced diet, maintaining a healthy weight, exercising regularly and quitting smoking (smoking increases lower extremity amputation risk by 40% in people with diabetes mellitus28). For more details, please refer to the ACG “Type 2 diabetes mellitus – personalising management with non-insulin medications”. Patients who require more comprehensive support for lifestyle modifications may also be referred to other resources or healthcare professionals for multidisciplinary care, as appropriate.
Regularly educate patients on the importance of good foot care and appropriate footwear (see Figure 4), in addition to their risk stratification result and recommended follow up frequency
This is a general guide designed to complement, and not replace, education or advice provided by a healthcare professional; tailor advice to the individual patient’s needs.
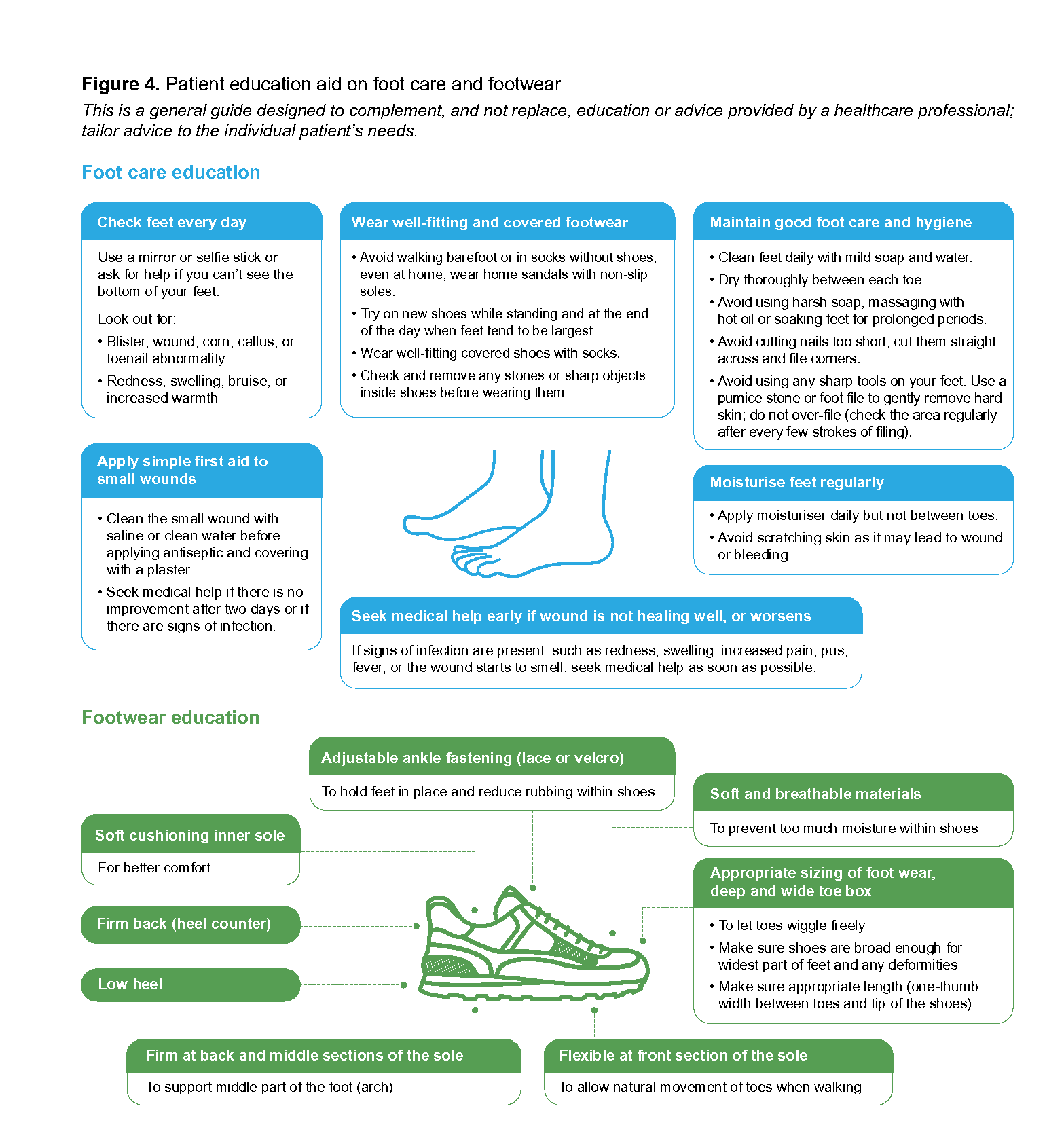
Figure 4. Patient education aid on foot care and footwear
Click here for larger version of the image
Expert group
Chairpersons
Dr Elaine Tan, Family Medicine (NHGP)
Dr Julian Wong, Vascular Surgery (The Vascular and Endovascular Clinic)
Members
Dr David Carmody, Endocrinology (SGH)
Adj A/Prof Chan Yee Cheun, Neurology (NUH)
Dr Cheah Ming Hann, Family Medicine (NUP)
Ms Marine Chioh, Nursing (AIC)
Ms Foo Mei Ching, Nursing (SHP)
Ms Chelsea Law Chiew Chie, Podiatry (KTPH)
A/Prof Inderjeet Singh Rikhraj, Orthopaedic Surgery (SKH)
Dr Donna Tan Mui Ling, Family Medicine (NHGP)
Mr Tan Liang Sheng, Podiatry (NUP)
Dr Brindha Balakrishnan, Family Medicine (SHP)
Dr Theresa Yap, Family Medicine (Yang & Yap Clinic & Surgery)
Dr Liew Huiling, Endocrinology (TTSH)
Acknowledgements
The Expert Group advising on this ACG is listed on the last page of the guideline. In addition, we would like to thank the following healthcare professionals for providing inputs as part of the ACG update:
Adjunct Associate Professor Glenn Tan, Adjunct Assistant Professor Muhd Farhan Bin Mohd Fadil, Ms Melissa Susan Phua, Ms Tiffany Chew Wen Ying, Dr Timothy Quek Peng Li, Dr Hong Qian Tai, Clinical Associate Professor Tay Jam Chin, Assoc Prof Chong Tze Tec, Dr Dharmaraj Rajesh Babu.
Feedback
Click here to give us feedback on this ACG.
Related ACGs
Type 2 diabetes mellitus — personalising management with non-insulin medications
Gestational diabetes mellitus — an update on screening, diagnosis, and follow-up
Hypertension — tailoring the management plan to optimise blood pressure control
Other related resources
Diabetic Retinal Photography (DRP) Screening Technical Reference Guide
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Foot assessment in patients with diabetes mellitus. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2024. Available from: go.gov.sg/acg-dfa
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.