
Promoting smoking cessation and treating tobacco dependence ACG
Last updated 19 May 2026
ACE Clinical Guidelines (ACG) provide concise, evidence-based recommendations to inform specific areas of clinical practice and serve as a common starting point nationally for clinical decision-making.
Published on 21 Feb 2025
Overview
This ACE Clinical Guideline (ACG) highlights the importance of consistent support to aid smoking cessation, even for individuals who have previously quit successfully. The ACG provides evidence-based recommendations on advising all smokers on effective methods to help them quit and assessing their willingness to quit, individualised behavioural support and pharmacological treatment, timely follow-up and interventions to prevent relapse. QR codes to I Quit resources are interspersed where appropriate and a handy guide on NRT options is also included.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Ask all patients about tobacco use and maintain an up-to-date record of their status.
Advise all people who smoke that effective methods to help them quit are available and assess willingness to quit based on their response.
Individualise behavioural support to maximise engagement and adherence to the quit plan.
Offer combination NRT (long-acting nicotine patch and short-acting NRT) or varenicline, alongside behavioural support.
Follow up within the initial weeks after the quit date.
Consider interventions to prevent relapse, such as extending pharmacological treatment and advising on coping strategies.
Download the ACG, reference and EtR
Smoking cessation ACG (Feb 2025) [PDF]
Smoking cessation references (Feb 2025) [PDF]
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the smoking cessation EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Smoking cessation EtR framework (Feb 2025) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guidance (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
In Singapore, tobacco smoking is a leading cause of death and disability from lung diseases and cancer,1 and imposes a significant economic burden.2–4 Even small decreases in smoking rates can have a major impact on disease burden and societal costs, making smoking cessation the most cost-effective medical intervention among people who smoke.5,6 Behavioural support and medications greatly increase the chances of successful quitting. Without such support, 95% of quit attempts will fail.7
Most people who want to quit smoking will pass through repeated cycles of short-term abstinence and relapse before achieving long-term abstinence. This underscores the importance of providing consistent support to aid smoking cessation, even for individuals who have previously quit successfully. General practitioners, community pharmacists, and other healthcare professionals in primary care settings are well-positioned to offer this support as they have frequent and important opportunities to identify people who smoke, provide advice and help them quit.7
The evidence-based recommendations in this guideline can be incorporated into, and implemented with, practical and systematic approaches like the 5As, ABC or 2As frameworks.a These frameworks have been shown to increase the promotion of smoking cessation by healthcare providers to their patients and achieve long-lasting quit rates.8–10
aMethods for supporting smoking cessation:
5As – Ask about smoking, Advise on the benefits of cessation, Assess motivation to quit, Assist stop attempts, and Arrange follow-up;
ABC – Ask about smoking, Briefly advise to quit and offer Cessation support;
2As – Ask about smoking and Act to help all tobacco users quit.
Recommendation 1: Ask all patients about tobacco use and maintain an up-to-date record of their status.
Timely identification of people who smoke enables the provision of appropriate support and interventions to quit, thereby alleviating the risk, symptoms or progression of related complications. After establishing the baseline smoking status of a patient, maintaining an up-to-date record of their smoking status can alert other healthcare professionals to the patient’s risk status, and prompt the delivery of smoking cessation interventions or other preventive care.11
Asking all patients about tobacco use at least annually can be a good starting point for maintaining an up-to-date smoking status record (i.e. current smoker, ex-smoker or never smoker). For patients who have recently quit smoking (i.e. less than 1 year from quit date), it is important to ask more frequently about their smoking status, as their risk of relapse is high (see Recommendation 5).
Additionally, enquire about smoking status or exposure to secondhand smoke when clinically appropriate, such as when a patient presents with new symptoms associated with secondhand smoke (e.g. lower respiratory tract infections, nasal irritation, ear infections, atopic dermatitis, worsening asthma control), especially those recorded as non-smokers.
When a patient is identified to be currently smoking, review their clinical history of established comorbidities and ask them about:
Degree of nicotine dependence (can be assessed with a scoring tool, such as the Fagerstrom scoring tool)
Any history of quit attempts
Any withdrawal symptoms during previous quit attempts
Any previous treatment for smoking cessation (e.g. self-initiated nicotine replacement therapy [NRT])
Identifying patients who vape and approaches for vaping cessation Vaping is the act of inhaling and exhaling aerosols from a device that heats liquid chemicals. Vaping devices (including e-cigarettes) can contain nicotine and other additives known to be linked to cancer, lung disorders, and negative effects on cardiovascular health. Furthermore, many vaping devices allow users to customise the product, including increasing nicotine uptake – with levels of toxicants that can vary significantly between and across brands and sometimes reach higher levels than tobacco smoke.12 Healthcare professionals are well-positioned to opportunistically ask patients whether they vape when asking them about smoking status, regardless of whether they are current smokers (i.e. dual users), ex-smokers or never smokers. Additional questions to consider asking include the type of e-cigarettes used and the frequency of vaping.13,14 People who vape should be advised about the positive reasons to quit (e.g. health, financial, environmental impact) and informed of the risks associated with continuing to vape.14 While the approach to vaping cessation is similar to smoking cessation management, calculating the appropriate dose of NRT for vaping cessation can be challenging due to the unknown nicotine levels in different e-liquids. Guidelines suggest that the dosing for combination NRT in smoking cessation can be extrapolated for vaping cessation.14–16 People who vape can join I Quit. For patient information, including useful resources on the reasons to quit and risks of vaping, click here As vaping is illegal in Singapore, individuals may be hesitant to disclose their vaping status and patterns, potentially impeding vaping cessation efforts. However, healthcare professionals are not obligated to report cases of vaping to the authorities. Letting patients know this could provide reassurance, enhancing the likelihood of obtaining an accurate record of vaping status and maximising chances of their participation in vaping cessation. |
Recommendation 2: Advise all people who smoke that effective methods to help them quit are available, and assess willingness to quit based on their response.
Studies have shown that offering assistance to people who smoke was associated with more quit attempts than directly advising them to stop smoking, soliciting intentions to quit, and reinforcing smoking harms.17 This may be due to such advice generating resistance and reducing the likelihood of smokers asking for assistance.18
Offering assistance in a non-confrontational way may help establish a more favourable rapport and be more effective in quitting attempts.19,20 This approach uses the person’s response to the offer to implicitly assess willingness to quit and guide the next steps. By adapting the interaction based on each individual’s response, healthcare professionals can more effectively engage people who smoke at different contemplation stages (see Figure 1).
For more examples of information tailored to different stages, click here
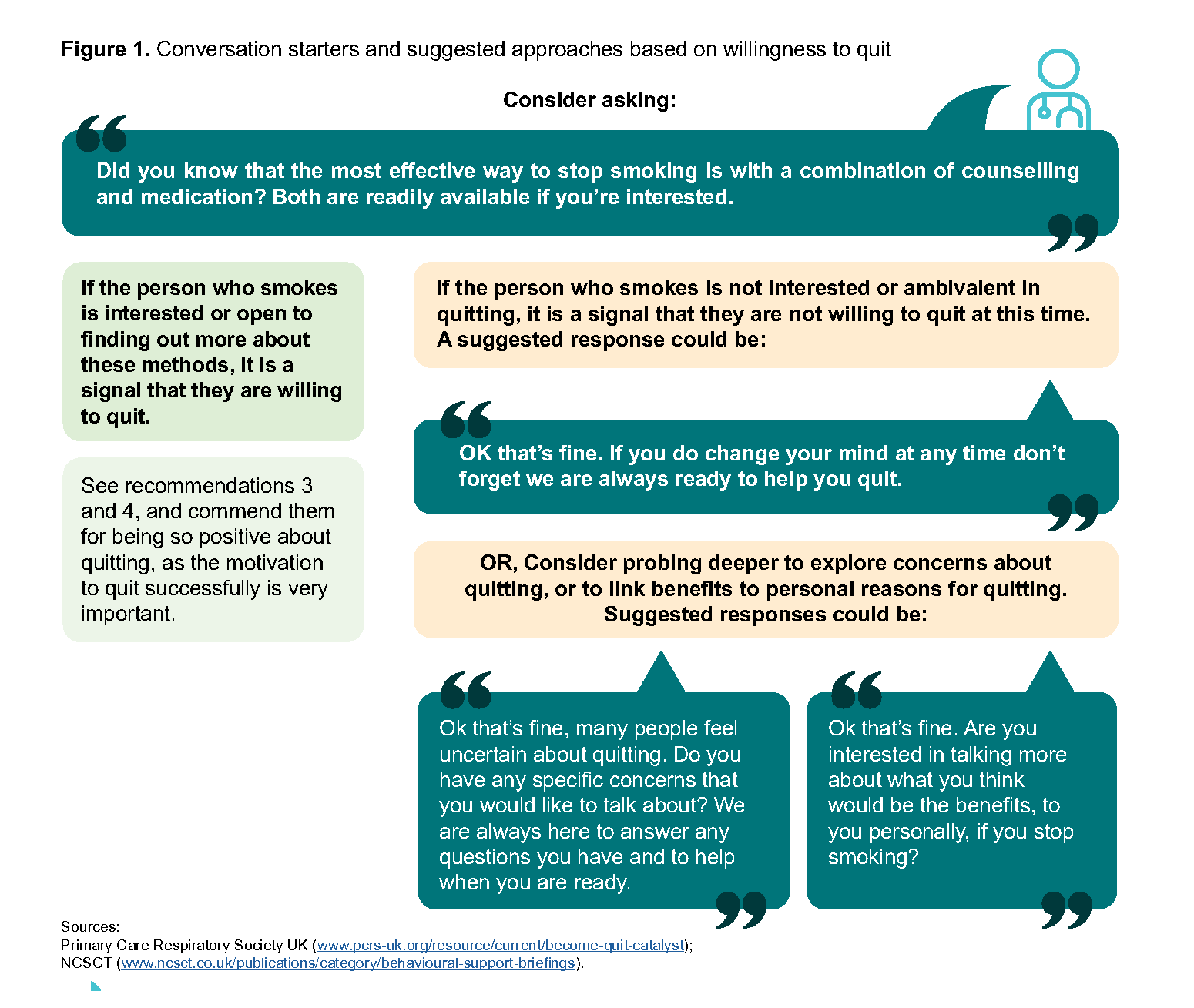
Figure 1. Conversation starters and suggested approaches based on willingness to quit
Notepad: People interested in quitting smoking but who do not have plans to do so within the next month In 2023, about half (46.5%) of the local population of daily smokers indicated an intention to quit. However only 18.2% of them planned to do so within the next 12 months.21 For people who have expressed interest or willingness to quit smoking, consider asking when they plan to stop. If they do not plan to stop within the next month, they may be classified as being in the contemplation stage and may have some reservations about making the final commitment to quit.22 These people may benefit from additional motivation such as showing your support and offering solutions to obstacles or mental blocks. |
Recommendation 3: Individualise behavioural support to maximise engagement and adherence to the quit plan.
Behavioural support strategies
Evidence indicates that providing behavioural support to people who smoke increases their chances of quitting.23
Every person who smokes has unique smoking habits, triggers, and motivations. While several components and modes of delivering behavioural support are effective,23–25 offering personalised behavioural support that addresses the specific needs and challenges of each person is more likely to resonate with them. This approach leads to greater engagement with, and adherence to, the quit plan, ultimately increasing the likelihood of successful quitting. Components of behavioural support include:26,27
Addressing barriers to quitting
Informing people who smoke of the effects of nicotine withdrawal (which may still occur despite receiving pharmacological treatment)
Identifying reasons and situations that trigger smoking
Advising on strategies to overcome or avoid triggers
Encouraging the support of family and friends
Setting a quit date
For patient resources on tips and strategies to stop smoking, click here and here
Obtaining support from external smoking cessation services
To ensure that all people who smoke are provided with adequate behavioural supportmthat meets their needs and preferences, consider utilising external smoking cessation services (e.g. I Quit, community pharmacies etc.), especially when on-site capacity is limited. Personalised quit plans are provided for all people who smoke, with the option to receive counselling and reminders through text messages, telephone calls or face- to-face sessions.
For more information on the I Quit programme, click here or call up a trained Quit Consultant at 1800 438 2000
Setting a quit date
Although setting a quit date is effective in helping people who smoke to quit, incorporating elements of high-quality goal setting to prepare them for the quit date can increase the chances of successful quit attempts:28
Encourage all people who smoke to commit to stop smoking at one go on or before a particular date (see the box below on “Abrupt quitting”)
Set a quit date that is most appropriate for the medication chosen (same day for NRT or one week from starting varenicline)
Consider the person who smokes’ values and preferences when agreeing on a quit date (e.g. avoiding stressful periods where they may have to cope with many things in their work or personal life)
If possible, ensure that the person who smokes agrees on a quit date that is scheduled within 14 days of the smoking cessation counselling
Notepad: Abrupt quitting Advising people who smoke to quit in one go increases the chances of quitting and is more effective for long-term abstinence, compared to a gradual reduction of cigarette consumption before quitting.29,30 Here is an example of advice to quit in one go: "It is best not to cut down the number of cigarettes you smoke before your Quit Date, as each one may become more important to you. Smoking your fewer cigarettes more intensely will also not make your quitting any easier than if you were to quit all at once."27 |
Recommendation 4: Offer combination NRT (long-acting nicotine patch and short-acting NRT) or varenicline, alongside behavioural support.
Pharmacological treatment should be offered in conjunction with behavioural support to all non-pregnant adult smokers who are willing to quit. As noted in Recommendation 3, behavioural support plays an important role in the success of smoking cessation by addressing an individual’s psychological triggers, habits and motivations. Combination NRT and vareniclineb are the most effective pharmacological treatments for helping people to quit smoking compared to placebo, and have similar effectiveness and safety profiles.31,32 Pharmacological treatment in specific subgroups, such as pregnant smokers, adolescents, or smokers with unsuccessful quit attempts or who have relapsed, is discussed later in this section.
Combination NRT
NRT is recommended for all people who smoke due to its effectiveness in helping them quit regardless of nicotine dependence.c Combination NRT works by using a long-acting form of NRT (e.g. patch), to help relieve baseline nicotine cravings and minimise withdrawal symptoms, with a short-acting form (e.g. lozenge, gum or mouth spray), to help with breakthrough cravings. Combination NRT is 27% more effective than any single-form NRT in helping people to quit smoking, with minimal differences in the risk of serious adverse effects – which are rarely experienced.33,34 As there does not appear to be a difference in efficacy between various types of short-acting NRT,33 use shared decision-making to select the type, based on the individual smoker’s values and preferences (see Table 1). For example, a person who attends many work meetings may prefer using lozenges for their subtlety, while someone who wants to ease withdrawal symptoms rapidly may prefer using the mouth spray for its faster onset of action.
Varenicline
Varenicline works by alleviating symptoms of craving and withdrawal, and by reducing the satisfaction derived from smoking. Varenicline is the most effective pharmacological monotherapy for smoking cessation, improving the likelihood of quit rates by 36% compared to bupropion and 25% for single-form NRT.32 Despite initial safety concerns of higher risks for neuropsychiatric or cardiac serious adverse effects, there appears to be no significant difference between varenicline and placebo, and serious adverse effects are rare.32,35,36 Mild to moderate severity nausea is the most common side effect experienced by people taking it to quit smoking.
Notepad: Other pharmacological strategies Bupropion Bupropion is an alternative pharmacological treatment that is effective in helping people to quit smoking compared to placebo. However, it is 25% less likely to help smokers quit compared to either varenicline or combination NRT and is associated with higher trial dropouts due to adverse effects compared to placebo 37 (common adverse effects are dry mouth and gastrointestinal disturbance, including nausea and vomiting). Bupropion is currently registered in Singapore for the treatment of major depressive episodes (i.e. off-label use for smoking cessation). Combining different treatments The combination of varenicline and NRT increases the likelihood of quitting smoking by 27–36% compared to using varenicline alone, and by 84% compared to NRT alone,38–41 but concerns about cost and possible increase in non-severe side effects may limit acceptance by people who smoke. There may be no difference in quit rates between the combination of bupropion and varenicline compared to varenicline alone, and the combination of bupropion and NRT compared to NRT monotherapy.37 |
Shared decision-making when selecting pharmacological treatment and duration
When selecting between pharmacological treatments, it is important to provide information on the medication options, including their mechanisms of action, potential side effects (see Table 1) and success rates (see Figure 2) for smoking cessation. Additionally, it is essential to understand the preferences, values and lifestyle of the individual who smokes to tailor the decision to their specific needs and circumstances. Involving the person who smokes in the decision-making process, even if some treatments have lower efficacy, can enhance adherence and commitment to the quit plan. If they prefer to use NRT monotherapy or bupropion together with behavioural support, advise them that these options are less likely to help them quit, compared to combination NRT or varenicline.
bAlthough registered locally for smoking cessation, varenicline is currently unavailable due to supply disruptions at the time of publication.
cGovernment subsidy is currently available to people who smoke with a Fagerstrom score of ≥3.
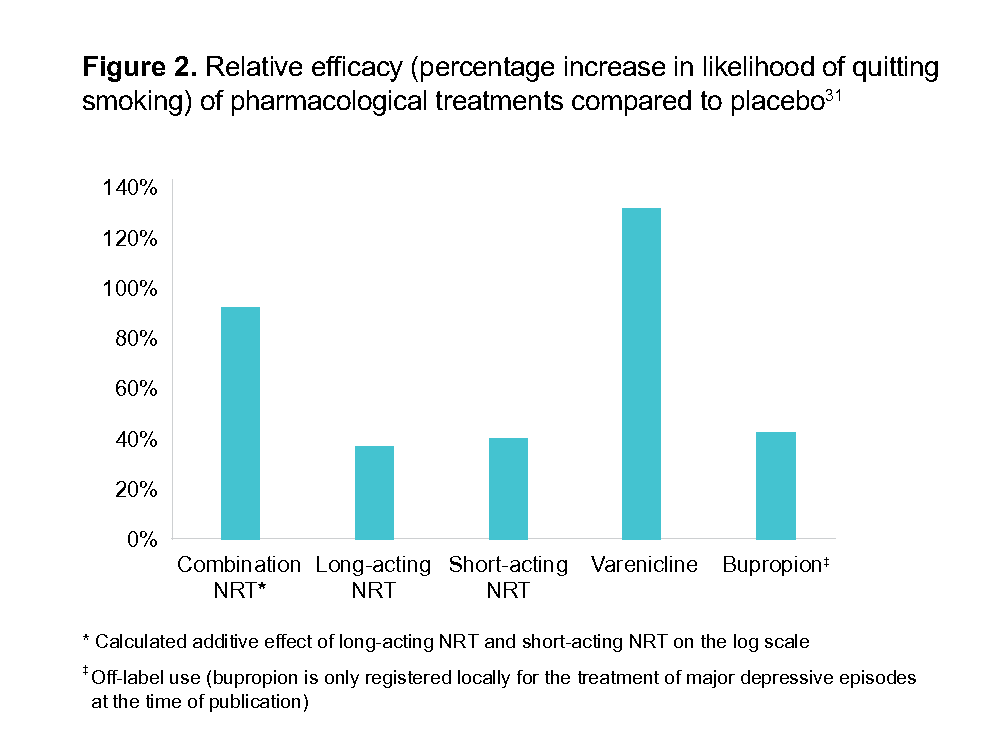
Figure 2.Relative efficacy (percentage increase in likelihood of quittingsmoking) of pharmacological treatments compared to placebo
Evidence regarding e-cigarettes(EC) for smoking cessation The overall evidence on the efficacy of EC as an intervention for smoking cessation remains uncertain due to mixed evidence and methodological concerns of the trials. Additionally, studies have shown that people who smoke traditional cigarettes who quit smoking with EC were eight times more likely to continue using EC after the trial compared to those who were allocated NRT, signalling continued nicotine dependence.42 Use of e-cigarettes is illegal in Singapore |
Smoking cessation for specific subgroups
Tailoring a smoking cessation strategy to the individual person’s needs and circumstances is essential to maximise chances of quitting. Advising specific subgroups of smokers may require additional considerations, due to the varying evidence of pharmacological treatment efficacy (see Figure 3), and should be underpinned by a shared decision-making approach, as described above.
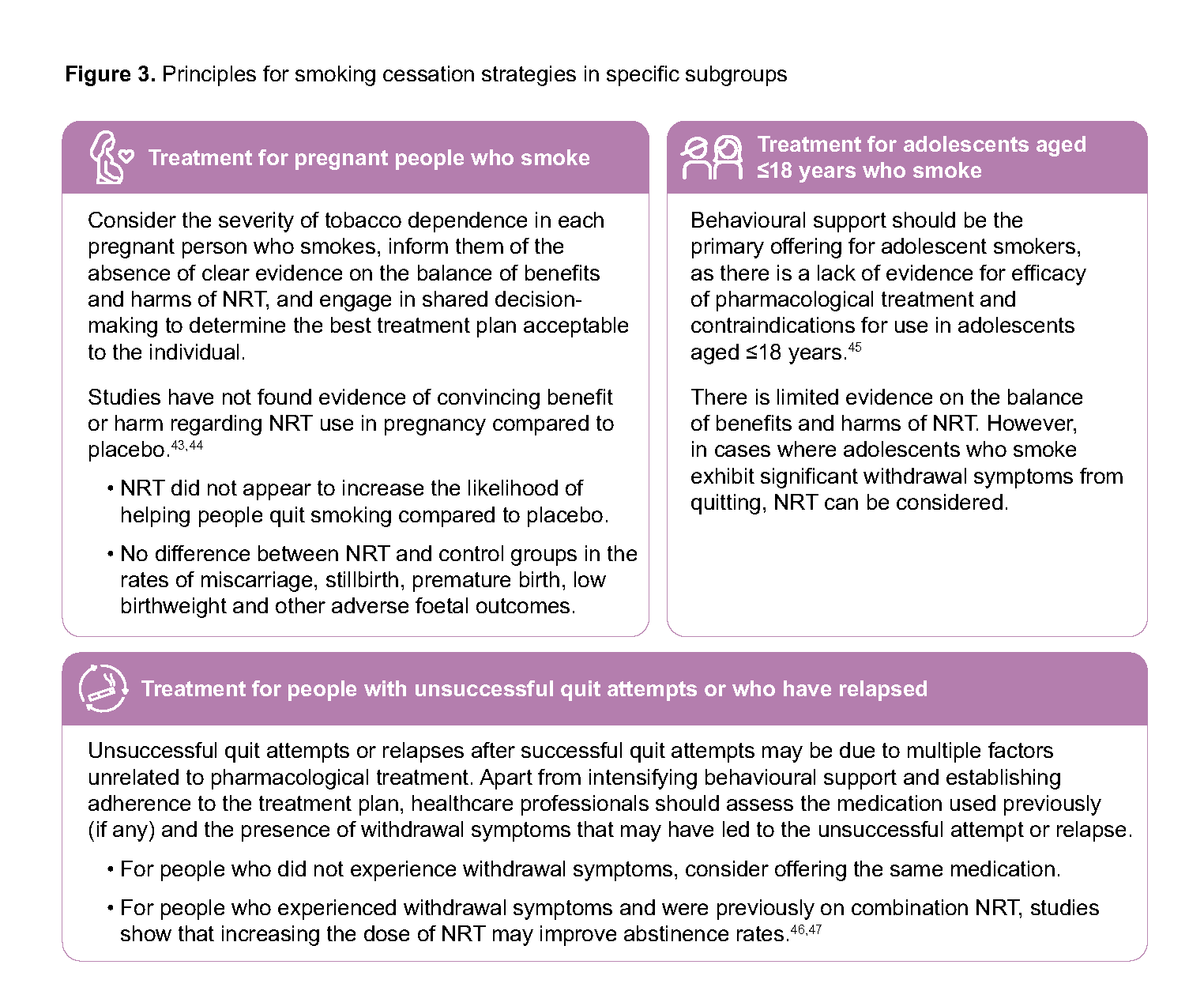
Figure 3.Principles for smoking cessation strategies in specific subgroups
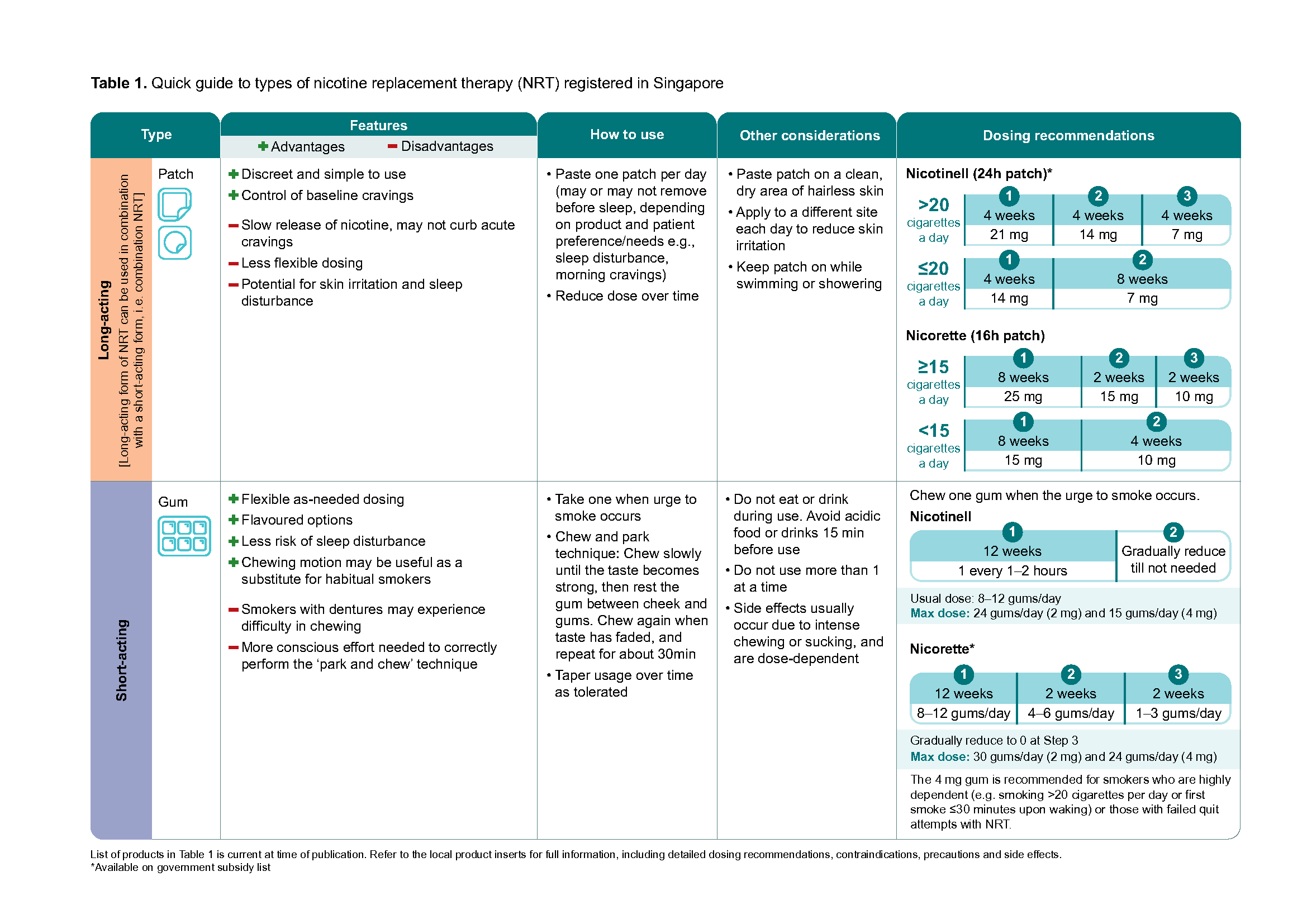
Table 1.Quick guide to types of nicotine replacement therapy (NRT) registered in Singapore - part1
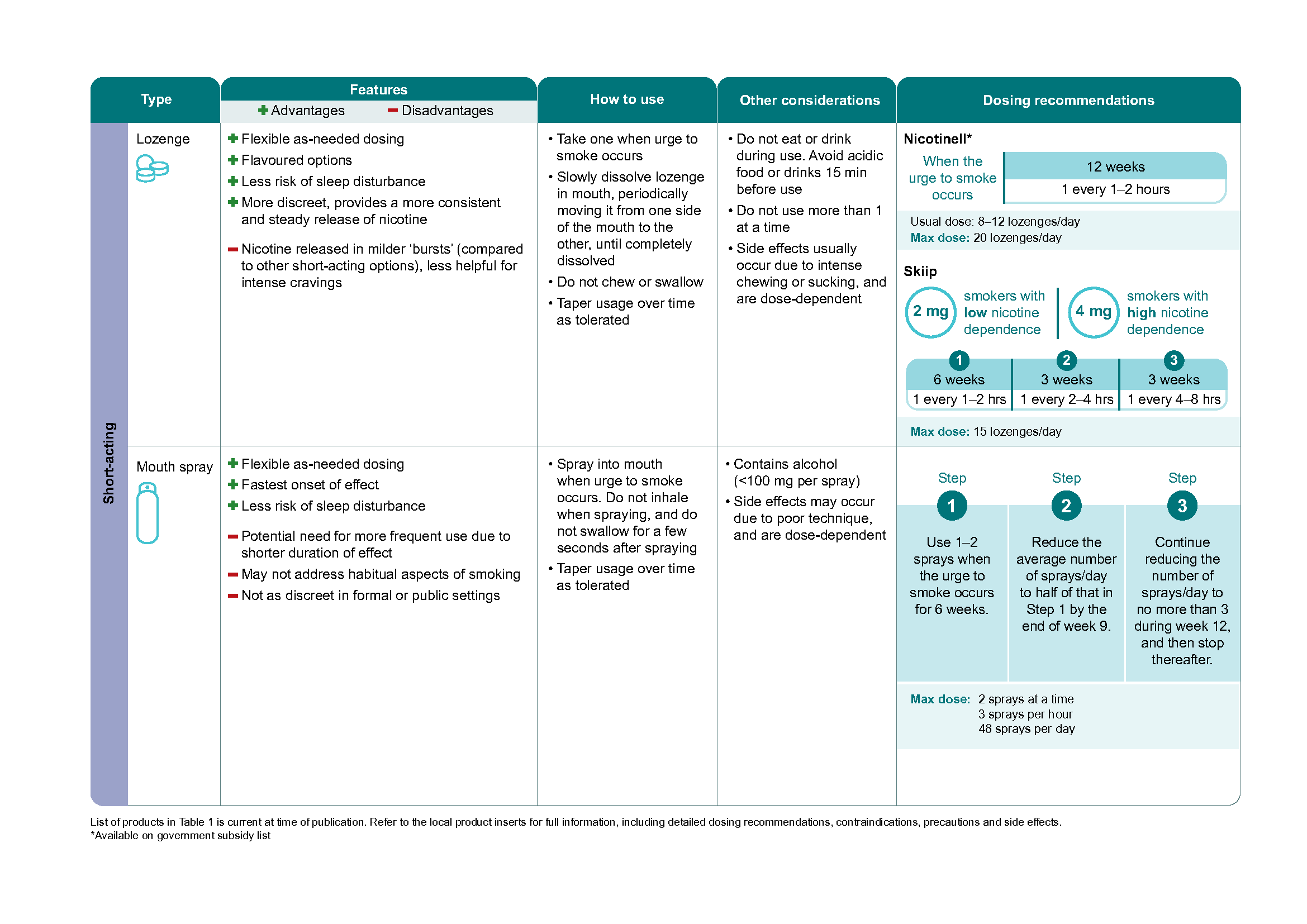
Table 1.Quick guide to types of nicotine replacement therapy (NRT) registered in Singapore -part2
Click here for the larger version of the image.
Recommendation 5: Follow up within the initial weeks after the quit date.
Frequency and mode of follow-ups
The risk of relapse is highest in the first few weeks after quitting due to nicotine withdrawal symptoms, which can surface a few hours after smoking the last cigarette. 48,49 Therefore, it is important to follow up (see “Monitoring parameters during follow-up”) with the patient within 1–2 weeks of the quit date, or within 4 weeks if doing so sooner is not feasible. This can be done in-person or over the telephone, by healthcare professionals, clinic staff or I Quit counsellor.
Monitoring parameters during follow-up
Smoking status
Frequency of slip-ups/lapses
Withdrawal symptoms
Adherence and presence of adverse effects from pharmacological treatment
History of sick days
Presence of smoking triggers (events that cause smokers to crave a cigarette)
Risk of relapse (may be predicted by asking patients about the amount of time spent with urges to smoke or the strength of urges to smoke)50
Patients at higher risk of relapse (e.g. multiple previous unsuccessful attempts, very high nicotine dependence, concurrent addictions, concerning social circumstances, etc.) or higher risk of complications from smoking (e.g. pregnant patients, severe cardiovascular or respiratory complications, etc.) should be prioritised for earlier follow-up if it is within the means of the healthcare professional. Regular follow-up beyond the initial weeks should also be planned. Studies suggest that the risk of relapse may remain high throughout the first two years of quitting,51 including a meta-analysis reporting that while the impact of pharmacological treatment on smoking abstinence at 12 months is beneficial, the proportion of people who benefit from medications decreases.52
Notepad: Effect of smoking cessation on other medications Smoking induces the activity of certain cytochrome P450 enzymes (e.g. CYP1A2) involved in the metabolism of some medications such as clozapine, olanzapine, warfarin or clopidogrel. After quitting smoking, decreased enzyme activity may result in slower metabolism of these medications and a consequent increase in serum concentrations. This applies also to patients who have quit smoking and are using NRT, as these drug interactions are caused by components of cigarette smoke other than nicotine. Consider reviewing the dose or use of these medications when clinically necessary.53 |
Recommendation 6: Consider interventions to prevent relapse, such as extending pharmacological treatment and advising on coping strategies.
Extending the duration of pharmacological treatment
There is limited evidence on optimal duration of pharmacological treatment. However, if risk of relapse is a concern, extending the duration can help.54,55 For people who smoke who are at increased risk of relapse (e.g. those who experience severe withdrawal symptoms towards the end of the medication regimen), engage in shared decision-making to understand their profile, values and preferences regarding potentially extending the duration of pharmacological treatment.
Coping strategies
Overcoming withdrawal symptoms
It is important to educate a person before and after their target quit date about possible physical and psychological withdrawal symptoms they may experience upon quitting and how to overcome them to prevent relapse (see Figure 4).
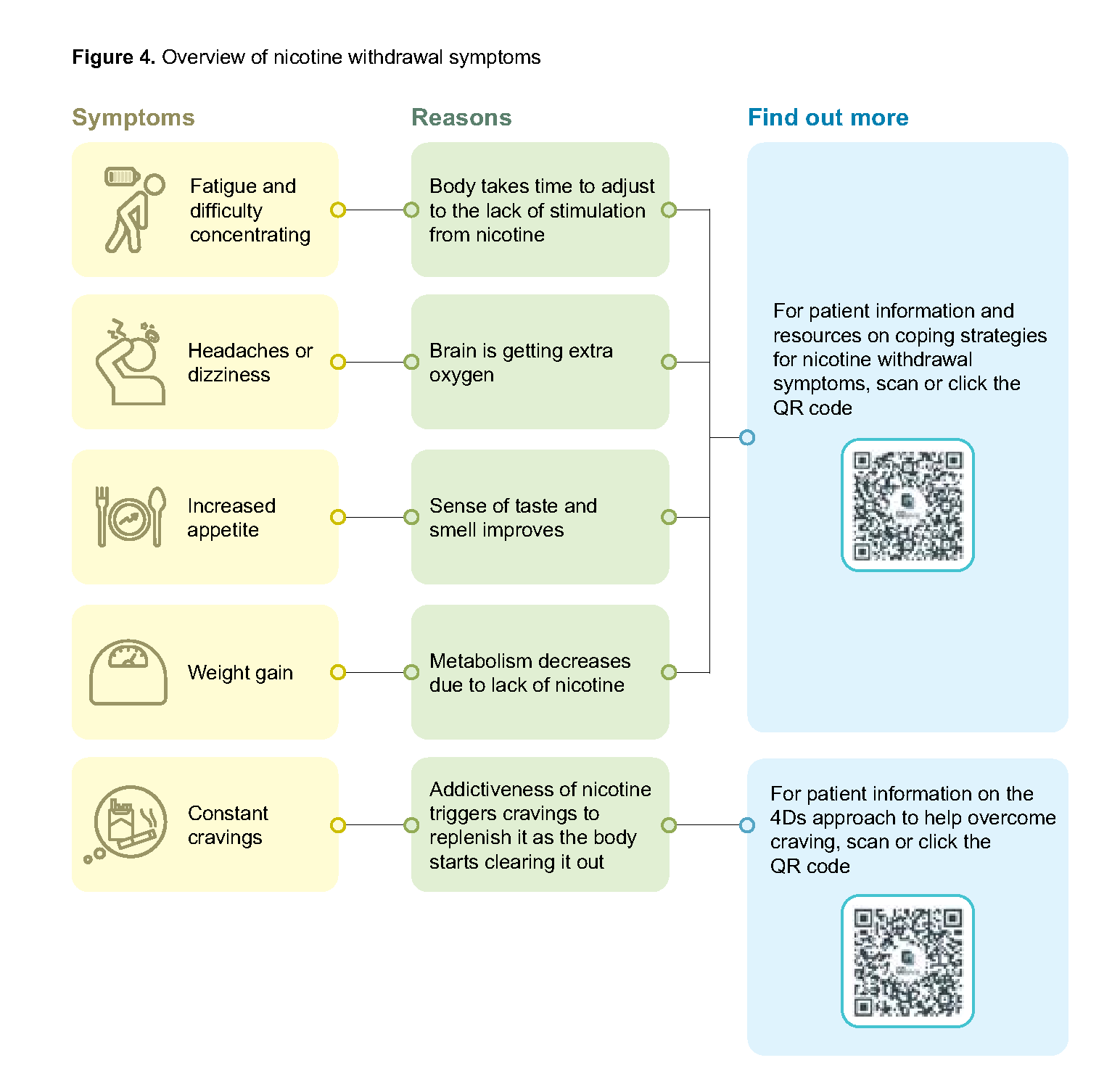
Figure 4.Overview of nicotine withdrawal symptoms
Recognising and coping with smoking triggers
Other than withdrawal symptoms, triggers can be an obstacle to maintaining abstinence from smoking. Offering support to identify and manage triggers unique to each person who smokes (e.g. drinking alcohol, emotional stress, social situations with other smokers) plays a key role in preventing relapse. These triggers can be managed by avoiding them and replacing them with positive habits to break the old routines that led to smoking.
For patient information on overcoming triggers, click here
Handling lapses and/or relapses
A “lapse” or a “slip-up” is an isolated smoking episode that occurs after at least 24 hours of abstinence and is followed by a resumption of the quit attempt. A relapse refers to the resumption of regular smoking after a period of abstinence.56 Although lapses often lead to relapses, it is important for lapses to be reframed as learning opportunities rather than being considered failures, which is how patients usually see them.57 After a relapse, consider the following steps: a review of factors contributing to the relapse, a reassessment of the smoking cessation plan, and the need to re-engage with support services. For patients who have relapsed, offer encouragement, reiterate the benefits of cessation, and consider advising them to quit again immediately.58
For patient information on handling lapses, click here
Expert group
Chairpersons
Dr Jason Chan, Primary Care (NHGP)
Dr Camilla Wong Ming Lee, Pharmacy (MOH)
Members
Mr Benjamin Chee Toh Ming, Health Promotion Board(MOH)
Ms Valerie Chua, Nursing (Frontier Healthcare Group)
Dr Joanne Khor, Primary Care (NUP)
Ms Kng Kwee Keng, Pharmacy (TTSH)
Ms Grace Kng Li Lin, Pharmacy (Watsons)
Dr Rachel Lim, Primary Care (SHP)
Dr Lambert Low Tchern Kuang, Psychiatry (IMH)
Adj A/Prof Puah Ser Hon, Respiratory and Critical Care Medicine (TTSH)
Ms See Chue Win, Nursing (AIC)
Adj A/Prof See Kay Choong, Respiratory and Critical Care Medicine (NUH)
Dr Sharon Shen Fengli, Primary Care (EH Medical Family Clinic [Bukit Batok])
Ms Daphne Tan Sze Ling, Pharmacy (NUH)
Dr Nelson Wee, Primary Care (Silver Cross Medical [Holland Village])
Dr Ryan Wong Chung Kiat, Primary Care (OneDoctors Family Clinic [Holland Village])
Feedback
Click here to give us feedback on this ACG.
Related ACGs
Chronic obstructive pulmonary disease – diagnosis and management
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Promoting smoking cessation and treating tobacco dependence. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2025. Available from: go.gov.sg/acg-smoking
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties