
Lipid management: focus on cardiovascular risk ACG
Last updated 22 May 2026
Published on: 15 Dec 2023 (amended, see below for version history)
Overview
This ACE Clinical Guideline (ACG) highlights lifestyle and pharmacological management for patients with hyperlipidaemia to reduce overall cardiovascular (CV) risk. The ACG offers evidence-based recommendations on tailoring the intensity of lipid lowering, with considerations by CV risk and other patient characteristics. Principles of managing statin-associated adverse effects are also discussed. An additional resource on the updated Singapore-modified Framingham Risk Score supplements the ACG.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Assess overall CV risk to inform initial and ongoing management of hyperlipidaemia.
Individualise management goals, including use of LDL-C targets, in the context of patient-specific risk factors.
Encourage and support healthy diet, physical activity, weight management, or smoking cessation, tailored to the patient’s circumstances.
Select intensive lipid-lowering therapy, using maximally-tolerated statin and adding ezetimibe as needed, for patients with:
Atherosclerotic cardiovascular disease (ASCVD);
Familial hypercholesterolaemia (FH).
Consider adding a PCSK9 monoclonal antibody or inclisiran for further risk reduction based on LDL-C level and clinical need.
Select a statin for patients with diabetes mellitus (DM), chronic kidney disease (CKD), or high 10-year CV risk (>20%). Consider adding ezetimibe for further risk reduction if needed.
Consider prescribing a statin for patients with 10-year CV risk between 10-20%, especially in the presence of risk enhancers.
Provide education and a lifestyle management plan for patients with 10-year CV risk below 10%; consider assessing risk enhancers for patients with borderline risk to discuss the clinical need for a statin.
For patients with elevated triglycerides (TG):
Assess and manage lifestyle-related and secondary causes;
At higher levels exceeding 4.5 mmol/L (400 mg/dL), consider fibrates to lower the risk of pancreatitis.
Encourage statin adherence by providing patient education, managing adverse effects, and optimising treatment to improve tolerability as needed.
Download the ACG and reference
Lipid management: focus on cardiovascular risk (Dec 2023) - v1.1 [PDF]
Lipid management: focus on cardiovascular risk references (Dec 2023) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Hyperlipidaemia is characterised by elevated lipid levels in the blood. Among Singaporean adults, hyperlipidaemia is a leading risk factor for atherosclerotic cardiovascular diseases (ASCVDs) such as myocardial infarction1 and ischaemic stroke.2 The goal of lipid management is to reduce the incidence or recurrence of ASCVD, especially coronary artery disease, through minimising accumulated exposure to low-density lipoprotein (LDL) cholesterol.
Individuals who may benefit from lipid-lowering pharmacotherapy can be identified through cardiovascular (CV) risk assessment. In addition to lifestyle intervention, statins are the main class of medications used to reduce lipid levels and ASCVD risk. Non-statin lipid-lowering medications are additional options for patients who require intensive lipid lowering or are unable to tolerate statins. This guidance provides evidence-based recommendations to optimise management of hyperlipidaemia by assessing overall CV risk and the clinical need for lipid-lowering medications, especially for healthcare professionals working in primary care settings.
Approach to lipid management – at a glance
Lipid management is a component of preventive care that aims to reduce the risk of atherosclerotic CV events, such as myocardial infarction and ischaemic stroke.
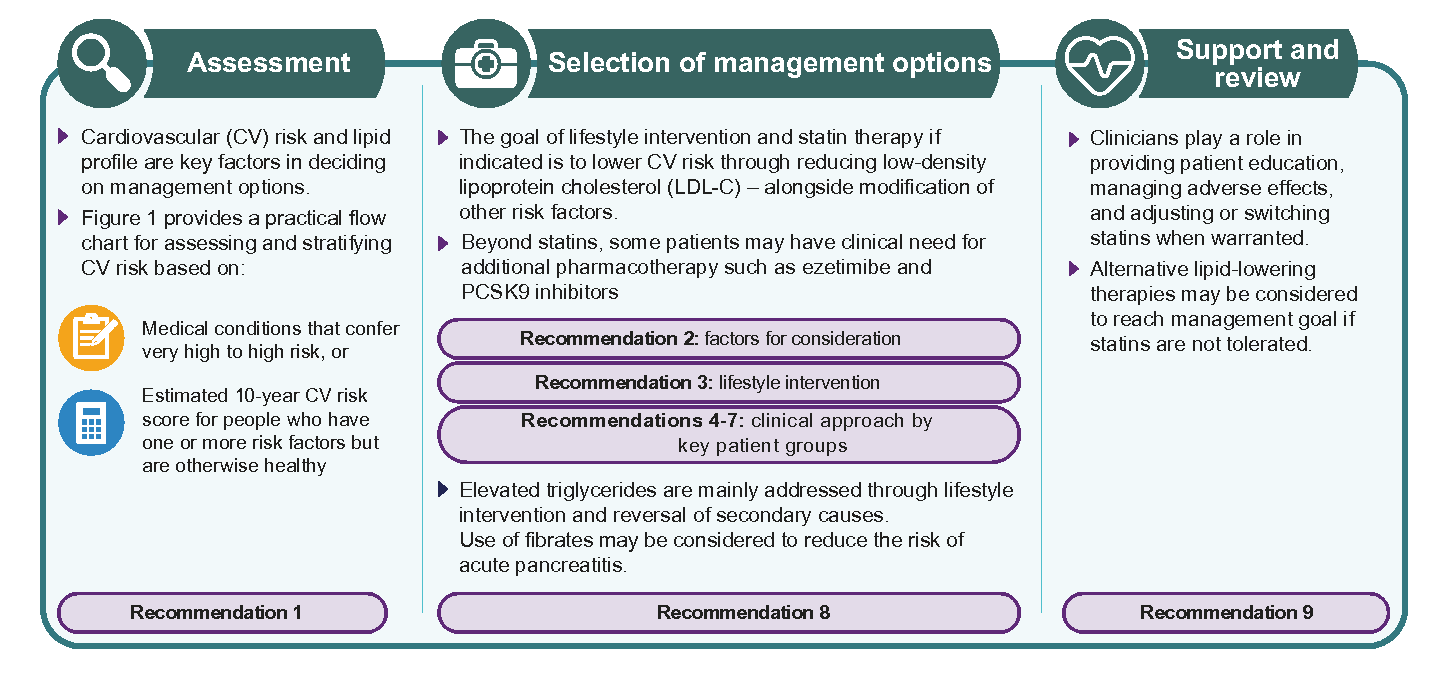
Assessment
Recommendation 1: Assess overall CV risk to inform initial and ongoing management of hyperlipidaemia
CV risk provides the starting point for clinical judgment and shared decision-making to manage hyperlipidaemia, since the benefit from lipid lowering is proportionate to the baseline cardiovascular risk. Specifically, CV risk assessment informs:
1. The need for statin initiation
2. The intensity of pharmacotherapy, including use of non-statin lipid-lowering medications
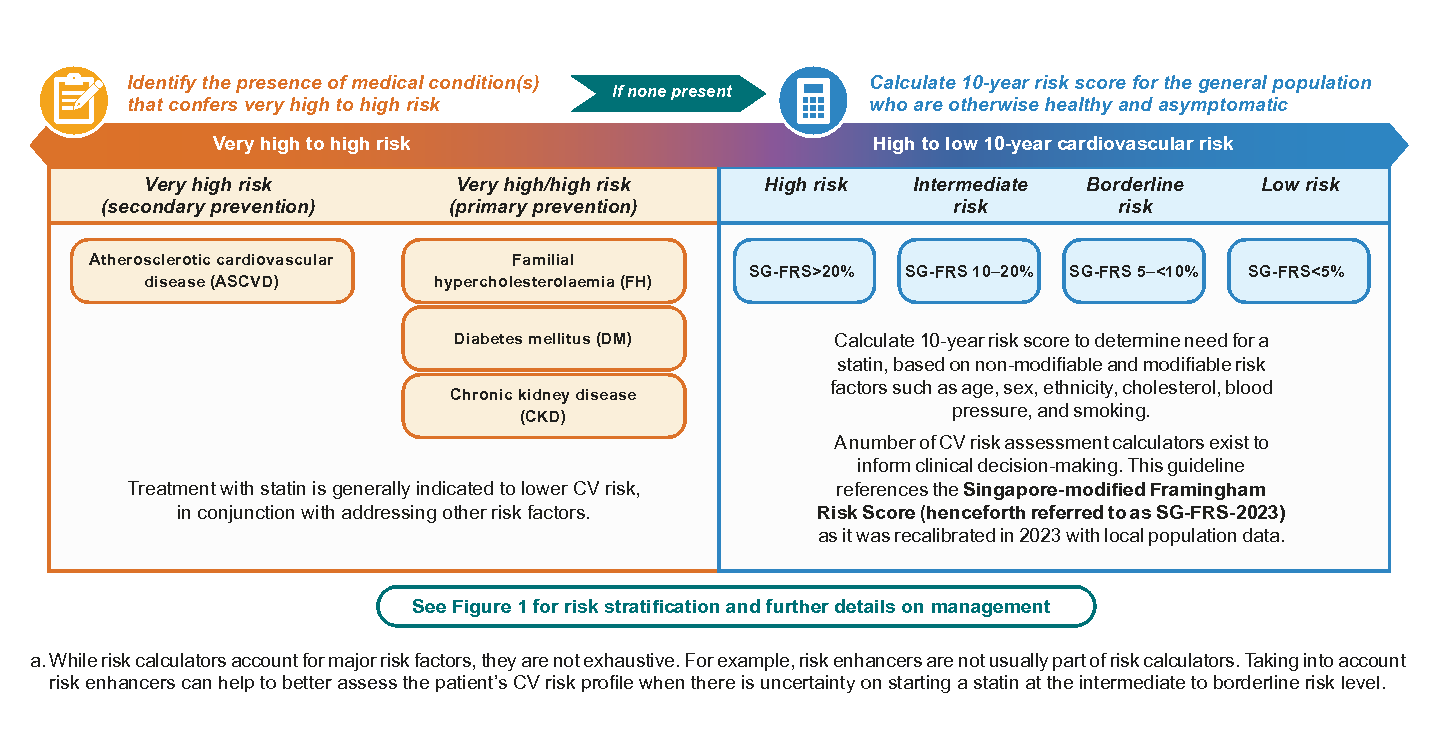
For the purpose of lipid management, assess for the presence of medical conditions that confer risk, and other CV risk factors. In the absence of established conditions that confer a very high to high level of risk, calculate 10-year risk scorea (see Figure 1 for risk stratification).
Click here for the updated SG-FRS score.
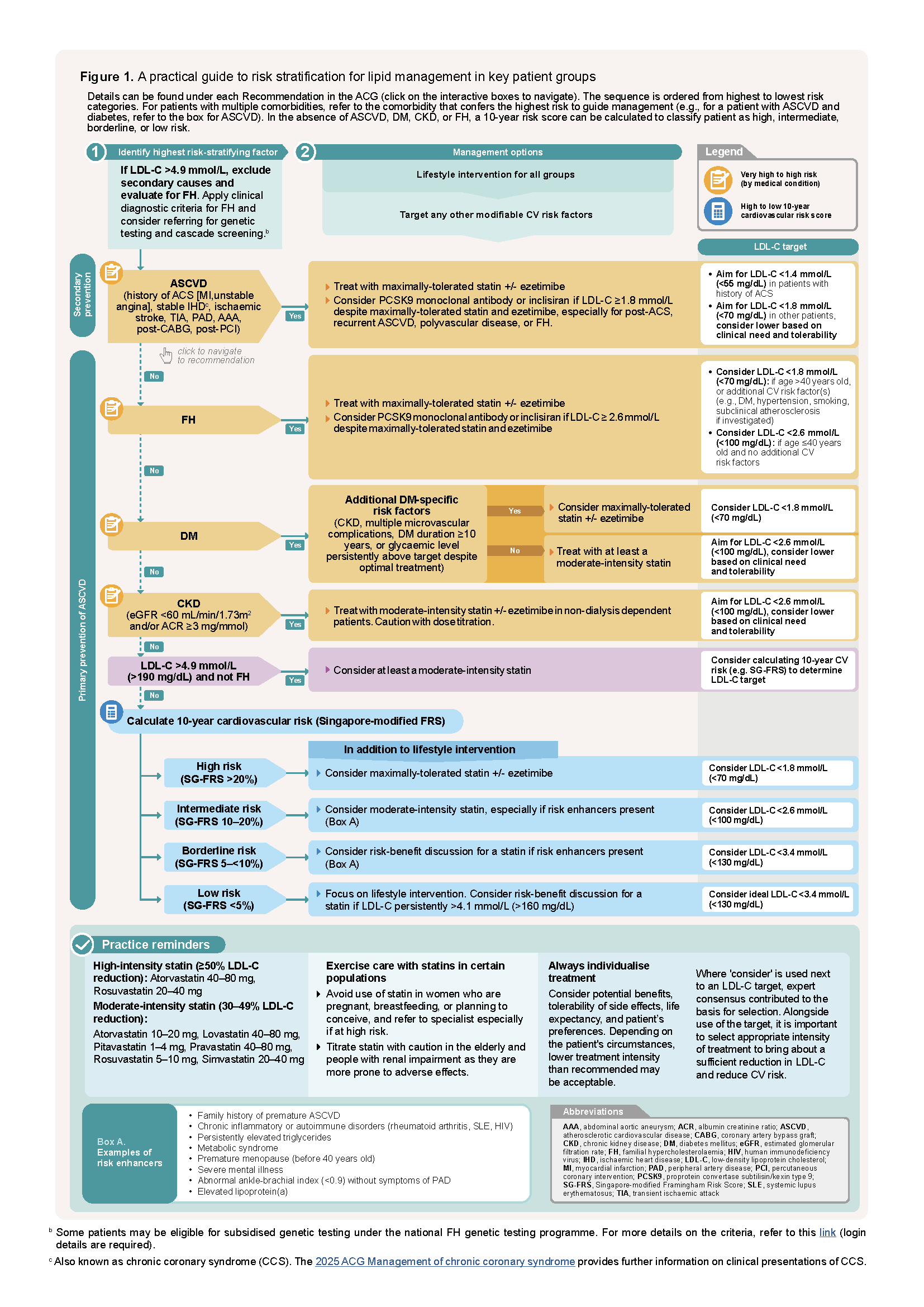
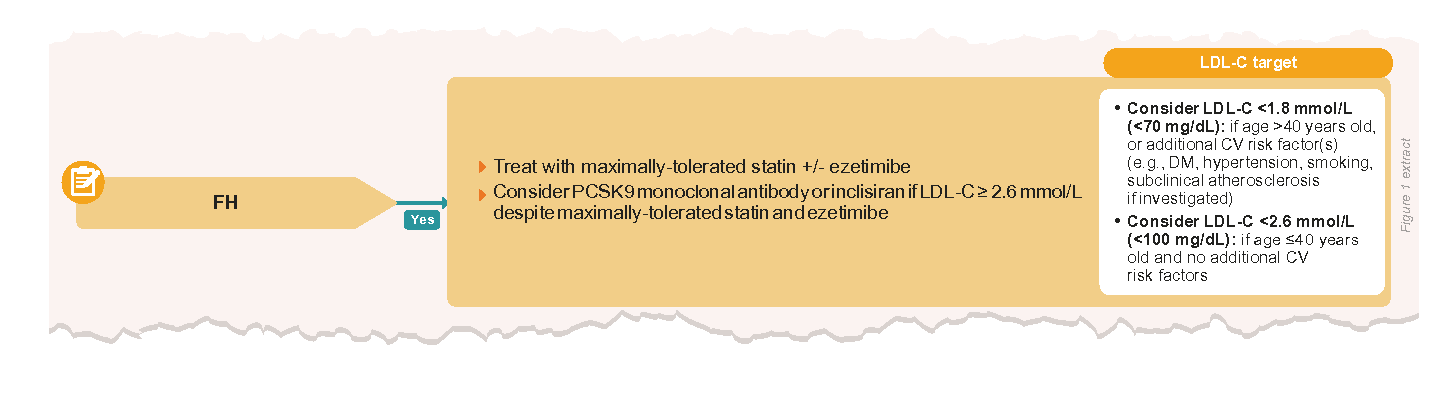
Figure 1. A practical guide to risk stratification for lipid management in key patient groups
Click here for the enlarged view of the above image
Selection of management options
Recommendation 2: Individualise management goals, including use of LDL-C targets, in the context of patient-specific risk factors
Reduction of CV risk requires multiple management strategies, as lipid management alone reduces but does not eliminate risk (residual risk can remain in patients who have achieved lipid control).
Management should be tailored to individual goals and characteristics, including comorbidities. For example, lipid management for a patient with both ASCVD and diabetes would be tailored to the risk conferred by ASCVD (CV risk is assigned according to the highest category fulfilled), while attending to other factors such as glycaemic control.
Lipid management options should include the following considerations:
Overall CV risk: absolute benefits from lowering LDL-C are greater as risk increases.
Lifestyle factors: a trial of lifestyle intervention (to address diet, physical activity, smoking) can be offered as primary prevention for those who are not at high risk of CV events. For those who are at higher risk, lifestyle intervention should be emphasised in parallel with pharmacological treatment.
Patient preferences and values
Putting the patient at the centre of management allows for shared decision-making, which is essential to achieve agreed goals and encourage adherence to medication and medical advice.
Lifestyle interventions should be tailored based on readiness to change and individual context (such as occupation and social support).
Age, functional status, and life expectancy:
In patients with poor functional status or short life expectancy, pill burden and the relative importance of other management goals can influence the choice of management options (e.g., the need to start pharmacotherapy).
While older age (>75 years) is not a contraindication for statin use, factors to be considered include potential benefits, risk of side effects (noting that renal or hepatic impairment and potential for drug interactions may be more likely), patient preference, and functional status.
Notepad: Use of lipid-lowering therapy in pregnancy In pregnant women, choice of lipidlowering therapy is limited by potential safety concerns, and balance of benefits and risks should be individualised. Generally, statins should be avoided in most pregnant patients. |
LDL-C remains an established marker for lipid management
Setting management goals in the form of absolute LDL-C targets may be useful in monitoring progress, and guides clinicians on management when pre-treatment LDL-C is not available. However, there are evidence limitations to the treat-to-target strategy, as this approach is indirectly derived from clinical trials and observational studies. To help contextualise use of LDL-C targets:
Select appropriate intensity of pharmacotherapy, as a sufficient reduction in LDL-C is necessary to reduce CV events.
Consider individual circumstances in which LDL-C target attainment is outweighed by other clinical priorities or is of uncertain benefit due to factors such as precautions with statin use, frailty, or polypharmacy.
If a patient cannot attain their LDL-C target, check for barriers such as poor adherence, adverse effects, misperceptions about statins, or issues with medication administration before increasing statin dose or adding another medication class.
Individuals vary in their response to lipid-lowering therapy; if pre-treatment LDL-C is available, percent reduction from baseline can be monitored alongside absolute LDL-C targets.
Lifestyle
Recommendation 3: Encourage and support healthy diet, physical activity, weight management, or smoking cessation, tailored to the patient’s circumstances
Lifestyle intervention, as a component of both primary and secondary prevention, should be tailored according to the individual’s context, overall CV risk, and lipid profile. In addition to addressing cardiometabolic risk factors, 3-7 patients may value benefits to quality of life and daily functioning.7-9 Among patients with clinical need for significant reduction in LDL-C, lifestyle intervention is complementary to pharmacotherapy.
Supporting behavioural change via engaging patients in their lifestyle intervention plan can optimise chances of sustained changes. Simple counselling frameworks may be applied to assess lifestyle factors and support patients, such as the 5A’s – ask, advise, assess, assist and arrange.10 Follow-up and support may be provided over several visits, including by allied-health professionals.
For individuals who have undertaken a trial of lifestyle intervention, 10-year CV risk can be reassessed after 3–6 months, alongside the lipid profile, to determine effectiveness.
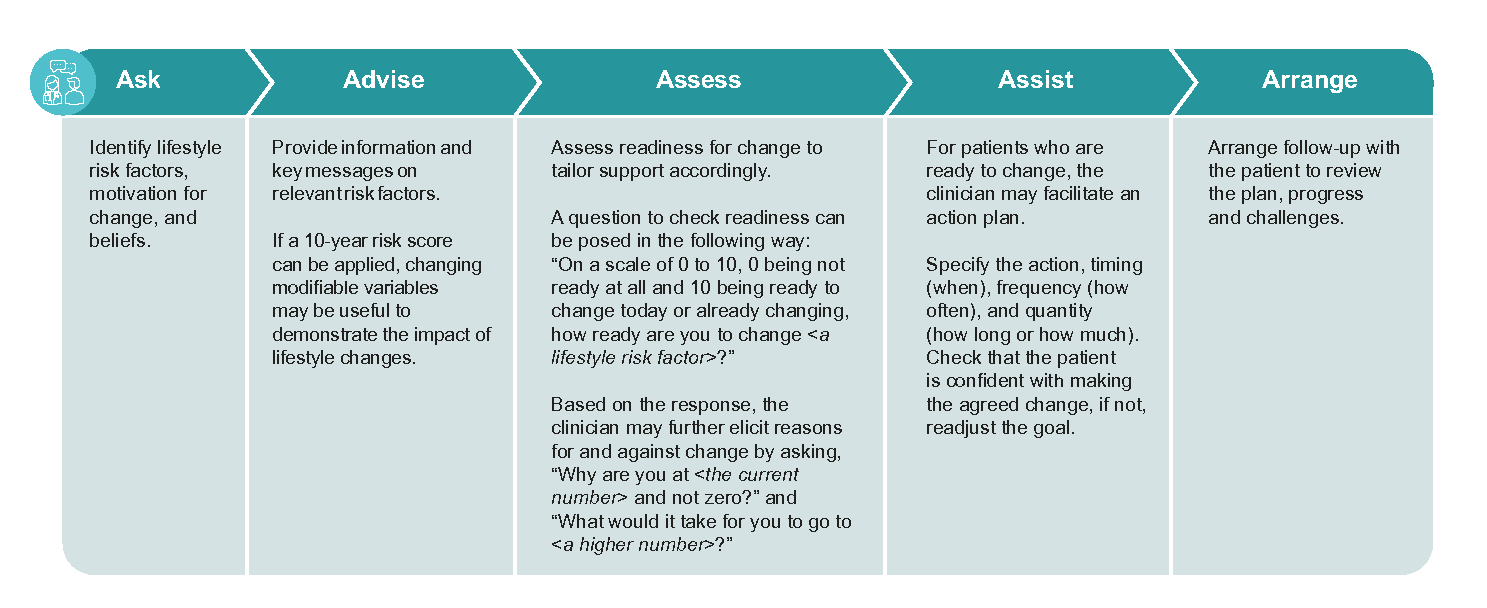
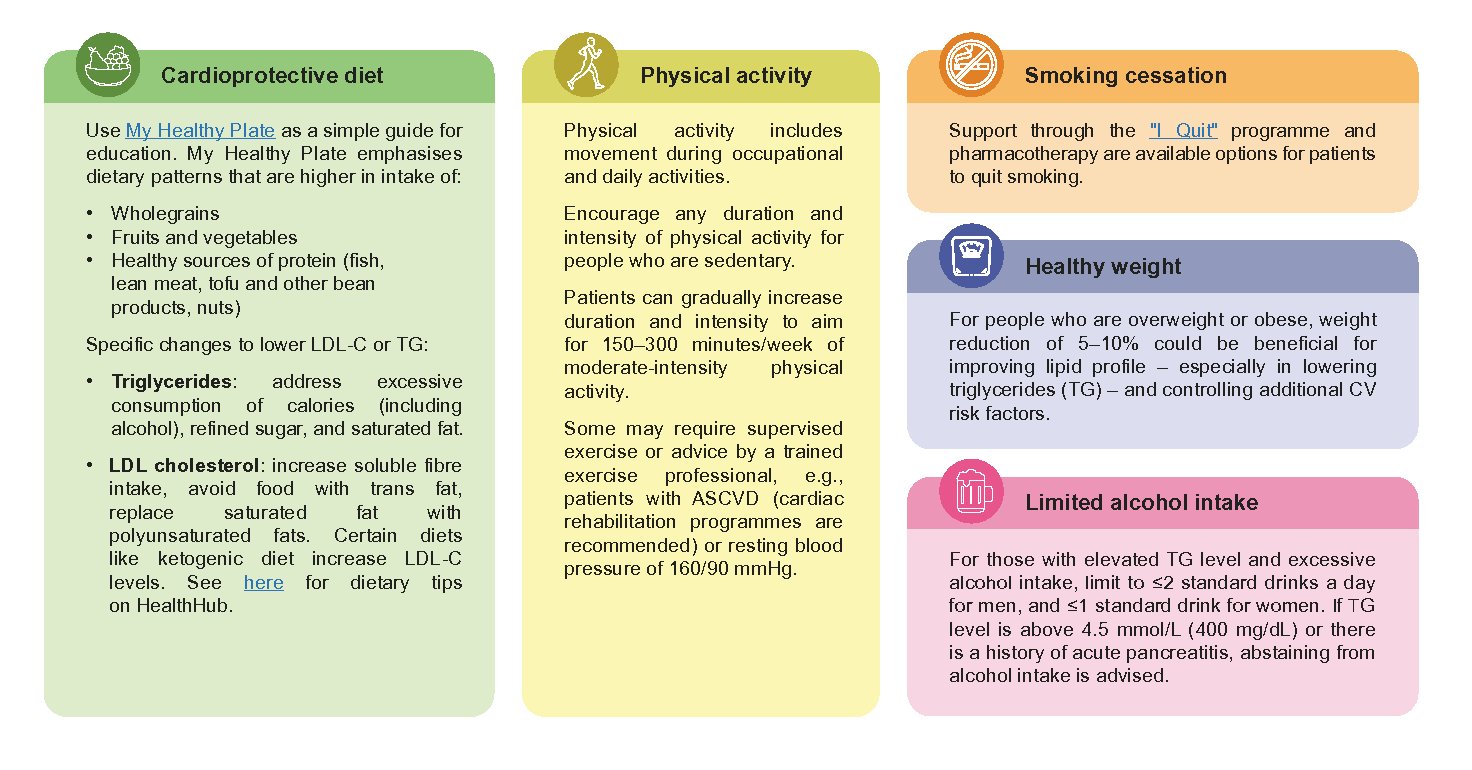
Figure 2. Key components of lifestyle intervention to support lipid management
LDL-C lowering pharmacotherapy
This subsection discusses lipid-lowering pharmacotherapy options for patients with various degrees of CV risk (patient groups are aligned with those in the Figure 1 flow chart).
Statins
In addition to lifestyle intervention, statins are the mainstay of pharmacological lipid management, lowering the risk of major CV events by 20–25% per 1 mmol/L (40 mg/dL) reduction in LDL-C.11,12 With the same relative risk reduction, absolute benefits are greater as risk increases. Apart from LDL-C lowering effect, statins modestly reduce triglyceride levels, lower inflammatory markers like C-reactive protein, and have plaque-stabilising effects.13,14
Statins range from low- to high-intensity, leading to different degrees of LDL-C reduction (Table 1).
Where “maximally-tolerated statin” is recommended, note that:15-17
Most patients in this category benefit from intensive lipid lowering, that is at least 50% reduction or to reach lower LDL-C targets, due to their high to very high level of CV risk.
Some patients may not tolerate a high-intensity statin dose. For these patients, a maximally-tolerated statin may be of lower dose or a less potent statin instead. The addition of a non-statin medication such as ezetimibe may be helpful in such patients.
Notepad: Before starting a statin, check for: • Pregnancy, preconception planning, or breastfeeding (if applicable) • Hepatic impairment, as use is contraindicated in decompensated cirrhosis and acute liver failure • Renal function to inform dose adjustment • Predisposition to adverse effects • Concurrent treatment that may interact with statins See Recommendation 9 for more details. |
Table 1. Statin intensity by ACC/AHA system of classification
Statin | Low-intensity dose | Moderate-intensity dose | High-intensity dose |
|---|---|---|---|
(LDL-C reduction <30%) | (LDL-C reduction 30–49%) | (LDL-C reduction ≥50%) | |
Atorvastatin | - | 10-20 mg | 40-80 mg |
Lovastatin | 20 mg | 40-80 mg | - |
Pitavastatin | - | 1-4 mg | - |
Pravatatin | 10-20 mg | 40-80 mg | - |
Rosuvastatin | - | 5-10 mg | 20-40 mg |
Simvastatin | 10 mg | 20-40 mg | * |
ACC, American College of Cardiology; AHA, American Heart Association
*Simvastatin 80 mg is not recommended due to high risk of myopathy; use should be restricted to those who have been taking 80 mg long-term without evidence of myopathy
Non-statin lipid-lowering medications
Use of a non-statin lipid-lowering medication may be indicated, if a patient is on maximally-tolerated statin and has not reached their management goal (despite good adherence) or is unable to tolerate statins. Factors for consideration include CV risk profile, potential adverse effects, affordability, and patient preference.
• Ezetimibe is an oral, cholesterol absorption inhibitor that lowers LDL-C by 15–20%,19-21 with associated CV risk reduction when combined with statin therapy.22
• Proprotein convertase subtilisin/kexin type-9 (PCSK9) inhibitors include monoclonal antibodies (evolocumab, alirocumab) and inclisiran. This class of medication reduce LDL-C by an additional 45–60% when added to statin therapy and may be considered for select patients with ASCVD or FH who require more intensive lipid lowering.23 In monotherapy trials with statin-intolerant patients, mean LDL-C reduction ranged from 45 to 52%. 24, 25
• Bile acid sequestrants (BAS) lower LDL-C by an additional 10–20%,26 but lack proven cardiovascular benefit and thus are less preferred as add-on medication. BAS require multiple doses daily and are prone to drug-drug interactions.
Notepad: General principles of lipid-lowering pharmacotherapy for CV risk reduction
|
Recommendation 4: Select intensive lipid-lowering therapy, using maximally-tolerated statin and adding ezetimibe as needed, for patients with: Atherosclerotic cardiovascular disease (ASCVD); Familial hypercholesterolaemia (FH). Consider adding a PCSK9 monoclonal antibody or inclisiran for further risk reduction based on LDL-C level and clinical need.
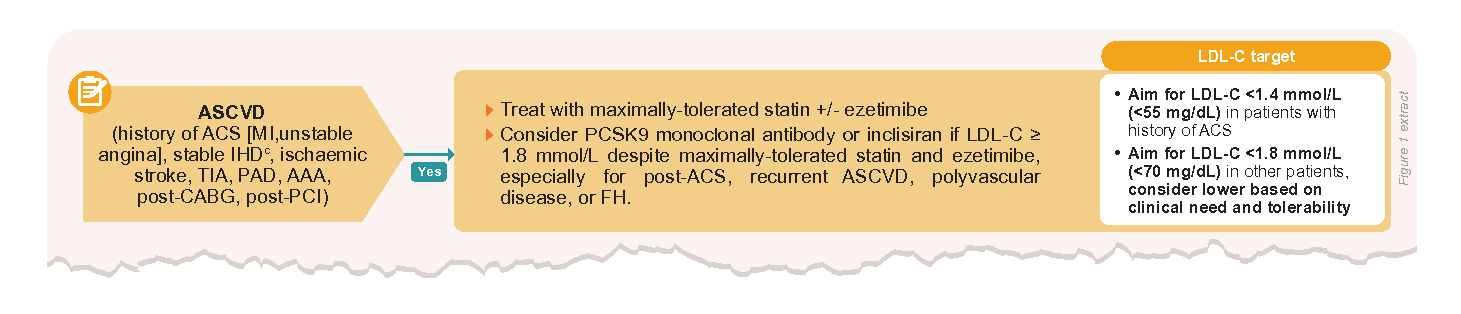
Intensive medical management in ASCVD aims to reduce risk of recurrent events such as acute coronary syndromes (ACS) and strokes. Due to significant CV risk at baseline and RCT evidence of further reduction in major CV events, intensive lipid lowering involves the addition of ezetimibe if the LDL-C target cannot be achieved.
Some individuals may achieve very low LDL-C (such as below 1.0 mmol/L or 40 mg/dL) with statin and ezetimibe. If tolerated well, the dosage can be maintained and does not need to be reduced, especially in patients with ACS. In the pivotal IMPROVE-IT trial, achieving LDL-C below 1.0 mmol/L was not associated with increased risk of myopathy, haemorrhagic stroke, hepatobiliary issues, neurocognitive problems, or cancer, compared to higher LDL-C values.27
Less safety evidence with very low LDL-C levels exist for other types of ASCVD. For example, slight increase in risk of intracranial haemorrhage with statins has been reported for patients with ischaemic stroke; other causes such as uncontrolled hypertension, anticoagulant treatment, or underlying frailty, may also contribute to this risk. However, the benefit in preventing ischaemic stroke outweighs the risk of intracranial haemorrhage for most individuals.28,29
Abnormally high LDL-C levels greater than 4.9 mmol/L (190 mg/dL) suggest a possible diagnosis of FH. History-taking can be directed to assess for FH through clinical diagnostic criteria, such as the Dutch Lipid Clinic Network (DLCN) or Simon BroomeTrust criteria. Besides a clinical suspicion of a hereditary cause, assess for secondary causes that may contribute to LDL-C elevation, such as hypothyroidism, nephrotic syndrome, or primary biliary cholangitis.
FH requires lifelong treatment with at least statin therapy to reduce the onset and progression of atherosclerosis. If untreated or not detected early, FH is associated with premature cardiovascular morbidity and mortality.
Clinical approach for ASCVD and/or FH
If not currently on lipid-lowering therapy, high-intensity statin or maximally-tolerated statin is recommended to achieve a substantial reduction in LDL-C. Monitor and titrate statin therapy towards the patient’s LDL-C target.
For individuals already on a statin, titrate to a high-intensity statin or maximally-tolerated statin, and add ezetimibe for an additional 15–20% reduction if LDL-C target cannot be achieved (see Table 3 below for additional considerations).
Table 3. Additional considerations when prescribing ezetimibe
Route of administration | Oral |
|---|---|
Dosing frequency | Once-daily |
Adverse effects and safety considerations | Elevation in liver transaminases – mostly self-limiting – may occur, and liver function testing should be performed when adding to a statin. The manufacturer does not advise use in moderate to severe hepatic impairment (Child-Pugh class B and C). Due to risk of cholelithiasis, fibrates other than fenofibrate should not be used in combination with ezetimibe. |
Cost and affordability | Ezetimibe 10 mg tablet exists in both branded and generic formulation (generic tablet available on government subsidy list). |
PCSK9 monoclonal antibodies (mAb) – alirocumab and evolocumab – reduce major CV events when added to statin-based regimens (the CV outcome trial for inclisiran is ongoing).
ASCVD: For patients with ASCVD whose LDL-C remains elevated at or above 1.8 mmol/L (70 mg/dL) despite adherence to maximally-tolerated statin and ezetimibe, consider the need and suitability for either a PCSK9 mAb or inclisiran – especially for patients with ACS, recurrent ASCVD, FH, or polyvascular disease (see Figure 4 below for additional considerations).
FH(Without ASCVD): Similarly, these medications are useful for primary prevention in FH (without ASCVD), if LDL-C levels remain persistently at or above 2.6 mmol/L (100 mg/dL). Only evolocumab is registered for use in both heterozygous and homozygous FH (a rare and severe type of FH). Shared care or specialist management at lipid clinics is recommended for patients who are unable to achieve a substantial reduction from baseline LDL-C or attain lipid control with maximally-tolerated oral pharmacotherapy.
ASCVD | For patients with ASCVD whose LDL-C remains elevated at or above 1.8 mmol/L (70 mg/dL) despite adherence to maximally-tolerated statin and ezetimibe, consider the need and suitability for either a PCSK9 mAb or inclisiran – especially for patients with ACS, recurrent ASCVD, FH, or polyvascular disease (see Figure 4 below for additional considerations). |
|---|---|
FH(Without ASCVD) | Similarly, these medications are useful for primary prevention in FH (without ASCVD), if LDL-C levels remain persistently at or above 2.6 mmol/L (100 mg/dL). Only evolocumab is registered for use in both heterozygous and homozygous FH (a rare and severe type of FH). Shared care or specialist management at lipid clinics is recommended for patients who are unable to achieve a substantial reduction from baseline LDL-C or attain lipid control with maximally-tolerated oral pharmacotherapy. |
Table 4. Additional Consideration when prescribing PCSK9 monoclonol antibodies or inclisiran
Route of administration | Subcutaneous: Alirocumab and evolocumab – counsel patients on injection technique and appropriate storage for self-administration. Inclisiran – should be administered by a healthcare professional. |
|---|---|
Dosing frequency | Alirocumab and evolocumab: according to the dose prescribed Inclisiran: at 3 months after the first injection, then once every 6 months. |
Adverse effects and safety considerations | Injection-site reactions (itch, bruising, pain), upper respiratory tract infections, back pain, and arthralgia, have been documented. As a novel class of medications, there is uncertainty regarding long-term safety. |
Cost and affordability | Alirocumab, evolocumab, and inclisiran are newer and higher in cost compared to statins and ezetimibe. More information on use of evolocumab under subsidy listing can be found here: ACE Technology Guidance |

If FH has been excluded, manage LDL-C according to their CV risk strata, as determined either by presence of relevant clinical conditions (ASCVD, DM, CKD) or based on 10-year risk calculation. Severe hypercholesterolaemia (LDL-C greater than 4.9 mmol/L or 190 mg/dL) confers a higher lifetime risk of major CV events – even without a known FH mutation detected by current genetic testing – and at least a moderate-intensity statin can be considered.
b Further information can be found in Supplement 1, Overview of lipid-lowering medications registered in Singapore
Recommendation 5: Select a statin for patients with diabetes mellitus (DM), chronic kidney disease (CKD), or high 10-year CV risk (>20%). Consider adding ezetimibe for further risk reduction if needed.
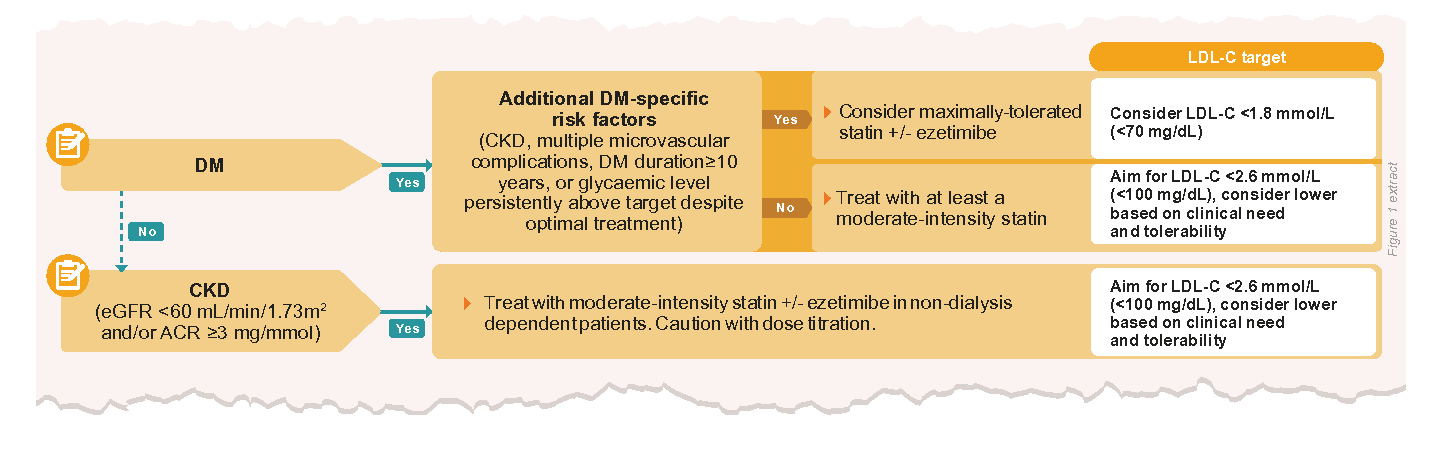
Most people with DM or non-dialysis-dependent CKD (without prior ASCVD or FH) have an elevated risk of CV complications over their lifetime. Also, the lipid profile in patients with DM or CKD often consists of mixed dyslipidaemia, where both TG and LDL-C are elevated.
Clinical approach for DM and/or CKD
As part of a multifactorial CV risk reduction strategy, use at least a moderate-intensity statin for patients with DM. Due to significant residual risk, consider increasing statin dose or adding ezetimibe as needed if DM-specific risk factors are present (CKD, multiple microvascular complications, long disease duration, or persistently above-target glycaemic levels).
• For advanced CKD, caution with dose titration of statin is advised to minimise the risk of myopathy, especially when eGFR <30 mL/min/1.73m2 (see Supplement 1 for dose adjustments and contraindications).
There is uncertainty of the benefit of high-intensity statins for patients with non-dialysis dependent CKD in primary prevention or treating intensively to target. A moderate-intensity statin, with or without ezetimibe, is recommended for this group. Benefits of initiating statins have not been demonstrated in dialysis-dependent patients.
Address modifiable risk factors, including glycaemic control and BP control:
For guidance on management of T2DM, refer to Type 2 diabetes mellitus – personalising management with non-insulin medications and Initiating basal insulin in type 2 diabetes mellitus
For guidance on management of CKD, refer to Chronic kidney disease – delaying progression and reducing cardiovascular complications
In the absence of high-risk medical conditions such as DM or CKD, overall cardiovascular risk should be assessed and stratified according to 10-year risk score to inform decision-making on statin initiation and intensity of lipid lowering.

Clinical approach for high 10-year risk (>20%)
The benefit of pharmacotherapy in reducing CV risk outweighs potential adverse effects for patients with a 10-year risk above 20%. It is therefore reasonable to offer a statin (high-intensity or maximally-tolerated dose), regardless of baseline LDL-C, and add ezetimibe as needed to reach management goals. In addition to statin-based therapy, address modifiable factors that contribute to the 10-year CV risk such as hypertension and smoking.
Factors such as patient preferences and values, life expectancy, frailty, and polypharmacy apply when deciding on starting a statin and selecting a target. While older age alone may confer significant CV risk, direct evidence of intensive lipid lowering is currently lacking for patients older than 75 years without ASCVD.30
It should be noted that the SG-FRS predicts the endpoint myocardial infarction and coronary death, and does not include ischaemic stroke as an outcome. Thus, established risk factors for stroke31 — namely hypertension, atrial fibrillation, physical inactivity, diet, smoking, and abdominal obesity — should be addressed, in view of their contribution to the overall CV risk.
Recommendation 6: Consider prescribing a statin for patients with 10-year CV risk between 10–20%, especially in the presence of risk enhancers.

Clinical approach for intermediate 10-year risk (10–20%)
Generally, a 10-year CV risk score of 10% and above indicates that CV benefits likely outweigh adverse effects from use of a moderate-intensity statin for most patients.c When assessing the balance between CV risk reduction and potential adverse effects conferred by statin therapy on an individual basis, note that risk enhancers could contribute to a higher CV risk than calculated. Discuss lipid management options with the patient, as informed by individual circumstances and preference, with the view to agree on a management goal and strategy (see Table 5 below for suggested areas of discussion).
Table 5. Key discussion points with the patient to decide management options
Areas of discussion | Examples of patient-centred approach |
Overall CV risk | •Communicate overall CV risk in a way that the patient can understand. For example, use absolute risk of events rather than percentages (e.g. 15% risk can be explained as “out of 100 people who have the same age, sex and risk factors, 15 will develop heart disease in the next 10 years.”) • Explain that risk enhancers indicate a higher risk than predicted • Reassure the patient that CV risk can be reduced with appropriate management of modifiable factors |
Lifestyle factors |
|
Benefits and potential harms of statins | • Explain that statins lower the level of cholesterol and reduce the risk of heart disease in the long term, together with lifestyle changes •Emphasise that the higher the CV risk, the more likely they are to benefit from the statin • Explain that statins may have adverse effects, but that they do not occur in everyone; reassure the patient that if these do happen, they can try other statins which may be more suitable • Provide information about monitoring that is required, such as liver function tests |
Patient values and preferences | • Discuss patient concerns and preferences |
Notepad: Risk enhancers Patients with risk enhancers may be at higher risk than their estimated 10-year CV risk score suggests. Some examples are: • Family history of premature ASCVD32,33 • Chronic inflammatory or autoimmune disorders (rheumatoid arthritis, SLE, HIV)34 • Persistently elevated triglycerides (e.g. >1.7 mmol/L or 150 mg/dL)35,36 • Metabolic syndrome37,38 • Premature menopause (before 40 years old)39,40 • Severe mental illness41,42 In some cases, additional markers may be available: • Abnormal ankle-brachial index (<0.9) without symptoms of PAD43 • Elevated lipoprotein(a)32 |
c For example, at a 10-year CV risk score of 10–20%, about 3–8 out of 100 people will avoid a major CV event by taking a moderate-intensity statin over ten years. In comparison, 1 out of 100 people may experience myalgia or new-onset diabetes over five years (slightly increased for those with risk factors for diabetes.
Notepad: Selective use of coronary artery calcium (CAC) scoring If uncertainty on the benefit-harm balance of statin initiation remains after both 10-year CV risk score and risk enhancers have been considered, some guidelines suggest potential use of CAC scoring to reclassify risk for decision-making. Risk scores are available which integrate the calcium score to recalculate 10-year risk (e.g., Multi-Ethnic Study of Atherosclerosis Risk [MESA] calculator). In many patients at intermediate risk, CAC scoring is not needed as the decision to start statin is clear. It is not intended for derisking patients with known risk, such as those with smoking history. More information on CAC scoring can be found in the Academy of Medicine Singapore (AMS) Clinical Practice Guideline on Management of Lipids 2023. |
Recommendation 7: Provide education and a lifestyle management plan for patients with 10-year CV risk below 10%; consider assessing risk enhancers for patients with borderline risk to discuss the clinical need for a statin.
Addressing modifiable risk factors and optimising lifestyle are the main management options for individuals with a 10-year CV risk below 10%, as the balance of CV benefits and adverse effects for a statin are less certain. If the patient has severe hypercholesterolaemia (LDL-C >4.9 mmol/L or 190 mg/dL, not FH), consider at least a moderate-intensity statin on account of the elevated risk factor alone.

Clinical approach for borderline risk (5–<10%)
The borderline risk group is a new category that recognises the potential benefit of providing earlier clinical attention to patients who will accumulate risk over a longer time period, if lifestyle and risk factor modification are not started.
Among patients in the borderline CV risk group, the benefit-risk balance of taking a statin is less certain.f Hence, risk enhancers may be helpful to decide which patients are closer to intermediate risk and may benefit from early discussion on clinical need for a statin or closer monitoring (see Table 5 above).

Clinical approach for low risk (<5%)
In general, statin therapy is not needed if 10-year CV risk is low (<5%). If LDL-C level is persistently high (above 4.1 mmol/L [160 mg/dL]) despite intensive lifestyle changes, consider a risk-benefit discussion for pharmacotherapy.
Optimal lipid control early and over time is associated with a lower risk of CVD or mortality in later life.44 Thus, clinicians may wish to offer an ideal LDL-C level of <3.4 mmol/L (<130 mg/dL) as part of shared decision-making with the patient. Many lowrisk patients with LDL-C between 3.4–4.1 mmol/L can still benefit from lifestyle intervention. Younger age groups especially have a longer time trajectory to be exposed to LDL-C and other risk factors, the burden of which is not reflected in their low 10-year risk scores.
While all patients should be reassessed and provided tailored advice on optimising lifestyle, some patients may benefit from a personalised lifestyle management plan that specifies the quantity, timing, and type of action to drive behavioural change (see Recommendation 3).
f. For example, at a 10-year CV risk score of 5–9%, about 1-3 out of 100 people will avoid a major CV event over ten years by taking a moderate-intensity statin. In comparison, 1 out of 100 people may experience myalgia or new-onset diabetes over five years (slightly increased for those with risk factors for diabetes).
Managing hypertriglyceridaemia
Recommendation 8: For patients with elevated triglycerides (TG): a). Assess and manage lifestyle-related and secondary causes; b). At higher levels exceeding 4.5 mmol/L (400 mg/dL), consider fibrates to lower the risk of pancreatitis.
Elevated triglyceride level (TG >1.7 mmol/L or 150 mg/dL) contribute to overall cardiovascular risk, while even higher levels lead to accumulation of large chylomicrons that may trigger pancreatitis.45 Correcting underlying causes and lifestyle factors is the cornerstone of management. Reversible secondary causes including the following should be identified and managed:45
• Diet high in saturated fat, simple sugars, and caloric intake
• Obesity or overweight
• Poorly controlled diabetes
• Alcohol intake
• Medications that raise TG (e.g. thiazide diuretics, beta-blockers), some of which may be replaced with lipid-neutral alternatives
• Hypothyroidism
Managing cardiovascular risk
Many patients with hypertriglyceridaemia also have concurrent CV risk factors that can be optimised. If not yet assessed or not already on a statin, they should be risk-stratified according to the figure 1.
Lifestyle intervention, and pharmacotherapy if indicated, are the cornerstone of managing CV risk in patients with elevated TG where secondary causes have been ruled out or addressed. Statins reduce TG levels by 10–20%,46,47 with higher reduction if baseline TG is higher.
Notepad : Fibrates in statin-treated patients Lowering TG through fibrates has not demonstrated significant additive benefits for CV risk reduction among patients optimised on statins. |
Managing pancreatitis risk
The risk of acute pancreatitis increases progressively with triglyceride level. In a cohort study, individuals with TG between 4.5–10 mmol/L have on average double the risk compared to those at 1.7 mmol/L or below.35 Previous history of acute pancreatitis is a strong risk factor for recurrence, even when TG is modestly elevated.
Internationally, differences exist in the recommended threshold of TG level for treatment to reduce pancreatitis risk.45 Most commonly, TG level either exceeding 4.5 mmol/L (400 mg/dL) or 5.6 mmol/L (500 mg/dL) is used to guide clinical attention to the need for more intensive dietary management, alcohol abstinence, and triglyceride-lowering pharmacotherapy. After excluding or addressing secondary causes, fibrates may be considered when significant TG lowering, up to 30–70%,48–50 is desired.
When the patient is on a statin, fenofibrate is preferred over gemfibrozil, as it has a lower risk of drug-drug interaction resulting in severe myopathy. Concomitant fibrate and statin therapy require liver function monitoring due to risk of hepatotoxicity. Multiple formulations of fenofibrate exist; refer to product-specific prescribing information for dosing.
Severe elevation of TG at 10 mmol/L (885 mg/dL) and above generally warrant specialist assessment and management.
Support and review
Notepad: Follow-up and review of patients with hyperlipidaemia include: ✓ Lipid control (LDL-C, TG) ✓ Lifestyle changes and maintenance ✓ Medication tolerability or adverse effects ✓ Treatment adherence ✓ Management of modifiable risk factors (e.g. blood pressure, glycaemic level, etc.) ✓ Changes in CV risk factors or clinical comorbidities |
Recommendation 9: Encourage statin adherence by providing patient education, managing adverse effects, and optimising treatment to improve tolerability as needed
The benefits of statins accrue over the long term, with a relative risk reduction of 16% in major coronary events during the first year that increases to above 20% in each subsequent year.12 However, poor adherence and premature discontinuation due to adverse effects are common, contributing to poorer CV outcomes.51 Clinicians play an important role in the structured assessment and management of adverse effects, as well as ongoing patient education, to achieve desired health outcomes.
Before starting a statin
• Proactively identify risk factors that may predispose patients to myopathy (e.g. older age, thyroid disorders, excessive alcohol consumption, family history of myopathy to statins, renal or hepatic impairment). While severe myopathy or rhabdomyolysis is rare, carefully monitor individuals with multiple risk factors.
• Check that patients do not have muscle-related issues or unexplained elevated liver transaminases at baseline that need to be investigated.
• Review other medications: ensure dose adjustment according to manufacturer’s advice to avoid drug-drug interactions or choose statins that are less susceptible to interactions.
Refer to Supplement 1, Table 3 for guidance on clinically significant interactions.
Patient education
Patients may have negative beliefs about statins, which contribute to reluctance in initiating or continuing statin therapy.52 It is therefore important to correct the understanding about benefits and risks of statin therapy, where applicable. For example:
• Frame information on adverse effects in the context of greater CV benefits
• Inform that adverse effects are infrequently caused by the statin itself and that if a new symptom arises, it can be managed
• Address individual concerns raised by the patient; unproven adverse effects purportedly linked to statin use by the mass media include cognitive impairment or dementia, eye cataracts, renal impairment, and cancer
Managing adverse effects
Muscle symptoms
Muscle aches or weakness are commonly reported by patients taking statins. However these symptoms are infrequently related to the statin and can arise through negative expectations of treatment; when compared with placebo, less than 10% of reported events are attributed to statin therapy itself.53,54 Recent smallscale studies among patients previously labelled as unable to tolerate statins due to muscle symptoms show that half to two-thirds are able to restart treatment, after observing similar symptoms between placebo and active treatment periods.54,55
Since statin intolerance is uncommon, clinicians play an important role to assess symptoms systematically and prevent unnecessary discontinuation, in discussion with the patient and after providing education. The degree of creatinine kinase (CK) elevation and symptom intensity informs whether the statin should be continued or stopped temporarily, and whether restarting with a lower dose or different statin can be considered (Figure 6).56-62 Adopt a patient-centered approach throughout and maintain rapport to meet the clinical need for CV risk reduction.
Rhabdomyolysis is rare and a more serious concern. Discontinue the statin if serious adverse effects are suspected and consider referral to hospital for management.
Note: Typical statin-associated muscle symptoms • Symmetric in distribution • Located in large muscle groups • Short in time to onset after starting therapy (within 4–12 weeks) • Resolve when statin is stopped, and recur when it is restarted. |
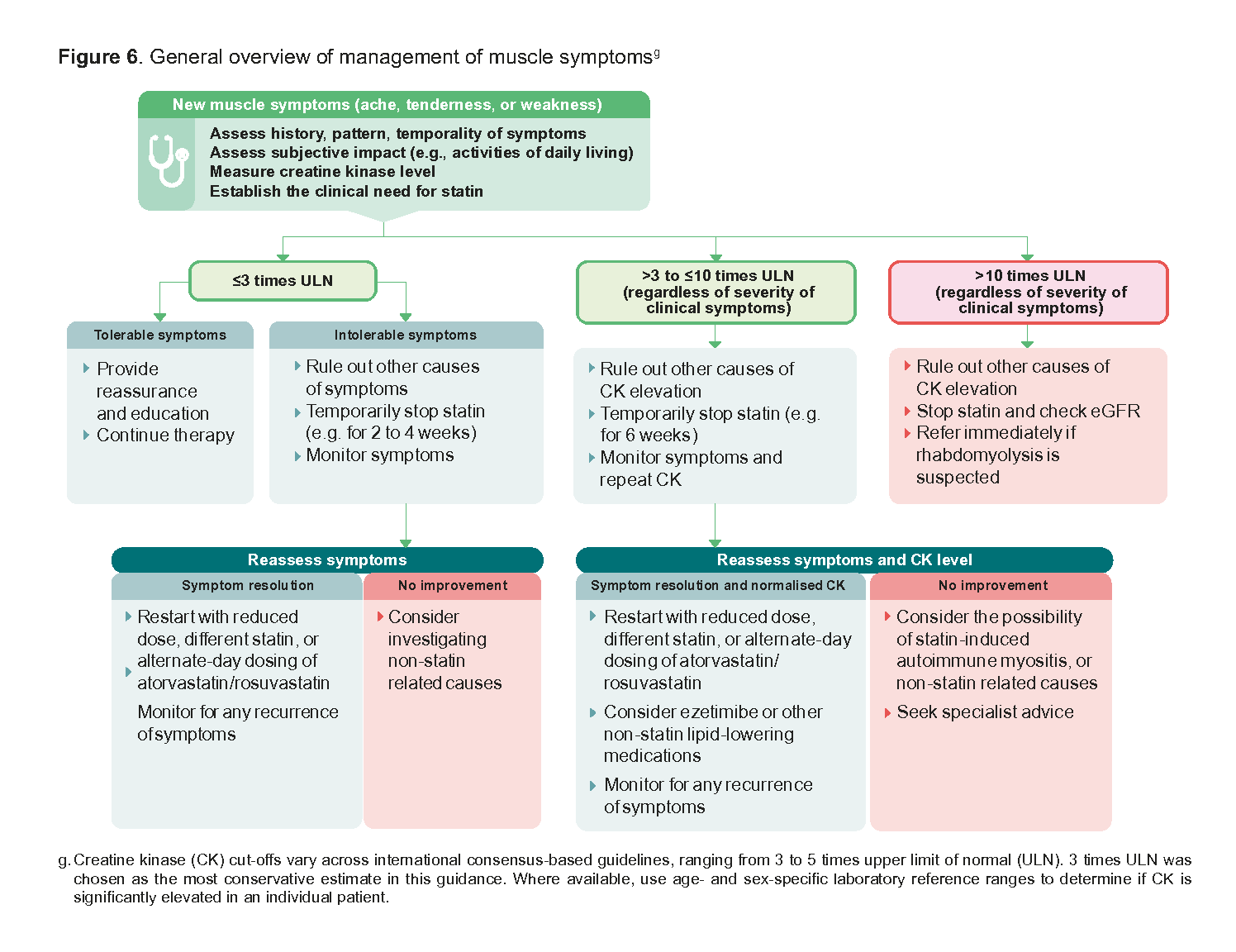
Figure 6. General overview of management of muscle symptoms
Liver transaminase elevations
Transient transaminase elevations occur in 1–3% of patients on statin therapy, but rarely rise to above 3 times upper limit of normal (ULN).63 If transaminases are elevated to above 3 times ULN without symptoms, reduce statin dose temporarily or withhold until levels normalise. Other causes of elevation should be considered. Restart statin with a reduced dose, different statin intensity, or use non-daily dosing of atorvastatin or rosuvastatin.
Clinical liver injury is rare and idiosyncratic. If there is concomitant increase in bilirubin (suggestive of cholestatic liver abnormality) or clinical symptoms of hepatotoxicity, stop statin and evaluate underlying causes.
New-onset diabetes
The risk of new-onset diabetes from statin use is generally higher for patients with predisposing risk factors, in whom management should include intensive lifestyle intervention.64 High-intensity statins are associated with slightly greater risk of new-onset diabetes compared to moderate-intensity doses, however in terms of absolute risk, this is outweighed by the benefit of averted major CV events.65 It is not recommended to withdraw statins in patients with new-onset DM as CV benefits outweigh the risk in most people.
Notepad: Definition of statin intolerance Based on consensus definitions, statin intolerance is a clinical syndrome that involves significant symptoms or abnormal elevation of laboratory markers in response to at least two different statins, which resolve when statin is stopped and recur when restarted.56, 57, 59, 61, 66 Such symptoms or abnormal elevation of laboratory markers are not attributed to drug-drug interactions or secondary causes, and lead to treatment goals not being met or act as a barrier to adherence. Complete statin intolerance is uncommon. There may be a need to use alternative non-statin lipid-lowering medications after systematic assessment and trials of statin. In a minority of individuals unable to tolerate the lowest dose of statins, including non-daily dosing of atorvastatin or rosuvastatin, consider the alternative use of ezetimibe as monotherapy. |
Supplementary Materials
Lipid-lowering medications in Singapore
Expert Group
Chairpersons
Clin Prof Chua Siang Jin Terrance, Cardiology (NHCS)
Dr Ian Phoon Kwong Yun, Primary Care (SHP)
Members
Dr Beh Chun Yen, Primary Care (NUP)
Ms Jen Pei-Hsuan, Pharmacy (NHGP Pharmacy)
Dr Khoo Yin Hao Eric, Endocrinology (Diabetes and Endocrine Clinic Pte Ltd, Gleneagles)
Dr Ian Koh Jan Ming, Primary Care (NHGP)
Dr Suraj Kumar, Primary Care (Drs Bain & Partners)
Dr Leong Choon Kit, Primary Care (Mission Medical Clinic)
Dr Lee Sze Haur, Neurology (NNI @ TTSH Campus)
Dr Lim Chun Leng Michael, Cardiology (Royal Healthcare)
Adj Prof Poh Kian Keong, Cardiology (NUHCS)
Dr Sim Kok Ping, Primary Care (Frontier Healthcare)
Adj Assoc Prof Ashish Anil Sule, Internal Medicine (TTSH)
A/Prof Sum Chee Fang, Endocrinology (KTPH)
A/P Doreen Tan Su-Yin, Pharmacy (NUS)
Dr Justin Tang I-Shing, Cardiology (KTPH)
Healthier SG cardiovascular risk calculator
Click here to access an online calculator to compute SG-FRS-2023 scores for the general population, originally developed as part of Healthier SG Care Protocols resource. The calculator additionally generates target levels for LDL cholesterol (and blood pressure) for patients at various levels of cardiovascular risk.
Additional resource for cardiovascular risk assessment using SG-FRS-2023 [PDF]
Message to healthcare professionals
With our nation’s move to Healthier SG, the optimal management of hyperlipidaemia has assumed critical importance. Numerous clinical trials have continued to examine the value of more intensive treatments and newer medications across a range of settings and add to the wealth of medical evidence supporting the role of effective lipid management in reducing cardiovascular risk. For the busy clinician, staying current with this latest evidence can be challenging, especially as international guidelines are not uniform in their recommendations. Hence it is timely that local guidelines on lipid management be updated.
As the national-level guideline, the MOH ACE Clinical Guideline on lipid management considers this broad variety of new evidence within the context of local practice to ensure it is relevant for all healthcare professionals caring for patients with hyperlipidaemia, especially those in primary or generalist care. Simultaneously, the Academy of Medicine, Singapore has developed their Clinical Practice Guideline, to cover the detailed needs of specialist management.
While all guidelines recommend using risk stratification for global ten-year cardiovascular risk to guide lipid management, there is a need to tailor these risk scores to our local population. Notably, guidelines should support, not negate, flexibility for healthcare professionals to customise treatment according to each patient's unique needs and profile.
We are grateful to Saw Swee Hock School of Public Health, National University of Singapore, and Ministry of Health Singapore, for the recalibration of the SG-FRS-2023 risk score. We are very grateful for the efforts of all who have contributed to crafting this guideline.
Clin Prof Terrance Chua Siang Jin | Dr Ian Phoon Kwong Yun
ACG Expert Group co-chairpersons
Version History
Lipid management: focus on cardiovascular risk
Version no. | Notes | Date of release |
|---|---|---|
1.0 | Publication of guideline | 15 Dec 2023 |
1.1 | Amendments made to the 2023 guideline:
| 26 June 2025 |
Feedback
Click here to give us feedback on this ACG.
Related ACGs
Chronic kidney disease — delaying progression and reducing cardiovascular complications
Type 2 diabetes mellitus — personalising management with non-insulin medications
Hypertension — tailoring the management plan to optimise blood pressure control
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Lipid management: focus on cardiovascular risk. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-lipid-management
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.