
Management of chronic coronary syndrome ACG
Last updated 19 May 2026
Published on 26 March 2025
Overview
This ACE Clinical Guideline (ACG) provides evidence-based recommendations for managing patients with chronic coronary syndrome (CCS), with a focus on antiplatelet therapy and non-pharmacological interventions, including physical activity, smoking cessation, and dietary advice. Additionally, principles for assessing patients with CCS presenting with acute exacerbation of chest pain are outlined.
The ACG includes links to two patient education aids on coronary heart disease (CHD), and myths and facts about antiplatelet medicines for chronic CHD.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
1a.Use long-term low-dose aspirin monotherapy for secondary prevention of cardiovascular events.
1b.Consider long-term clopidogrel monotherapy as an alternative to aspirin.
2.Review patients following PCI to confirm that there is a specified treatment duration for their dual antiplatelet therapy and check with the referring cardiologist if treatment duration is unclear.
3a.For patients with new-onset AF with no recent stent (within the past 12 months), consider oral anticoagulant monotherapy based on modified CHA2DS2VASc score and patient factors such as comorbidities and bleeding risk.
3b.For patients with new-onset AF and a stent within the past 12 months, consult a cardiologist to reassess and optimise the current antithrombotic therapy.
4.Optimise management of comorbid or associated conditions in patients with CCS to reduce overall cardiovascular risk and complications.
5.Encourage sustained lifestyle interventions, including regular physical activity tailored to the patient’s capabilities and preferences.
6.Schedule regular follow-up visits for all patients with CCS to monitor symptoms, assess medication adherence, and adjust treatment plans as needed.
Refer to the Evidence-to-Recommendation (EtR) framework below for a summary of the factors underpinning the ACG’s recommendations.
Download the ACG, reference and EtR
Management of chronic coronary syndrome (Mar 2025) [PDF]
Management of chronic coronary syndrome references (Mar 2025) [PDF]
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the chronic coronary syndrome EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Management of chronic coronary syndrome EtR framework (Mar 2025) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Ischaemic heart disease (IHD) is the leading cause of death among non-communicable diseases worldwide.1 It is one of the leading causes of morbidity and mortality in Singapore,2, 3 with 2021 data reporting that it was responsible for approximately one-fifthof all deaths.3 The impact of IHD extends beyond the cardiovascular (CV) system, and it is commonly associated with various chronic comorbidities,4 including hypertension, dyslipidaemia, diabetes mellitus, and ischaemic stroke.
Chronic coronary syndrome (CCS) is a common form of IHD. While antithrombotic therapy is the cornerstone of CCS management, local primary care physicians highlighted uncertainty regarding its use for patients with CCS,5 including initiation, optimal dosing, and monitoring parameters. Hence, this ACE Clinical Guideline (ACG) provides evidence-based recommendations for managing CCS, focusing on the initiation and review of antithrombotic therapy in primary care settings. The ACG also covers pharmacological and non-pharmacological interventions used to manage chronic comorbidities associated with CCS, tailored to each patient’s individual needs.
Chronic coronary syndrome (CCS),a also known as chronic or stable ischaemic heart disease or stable coronary artery disease, refers to clinical presentations that arise due to structural or functional alterations related to chronic diseases of the coronary arteries or microcirculation.6 CCS encompasses six different clinical presentations as summarised in Figure 1.6, 7
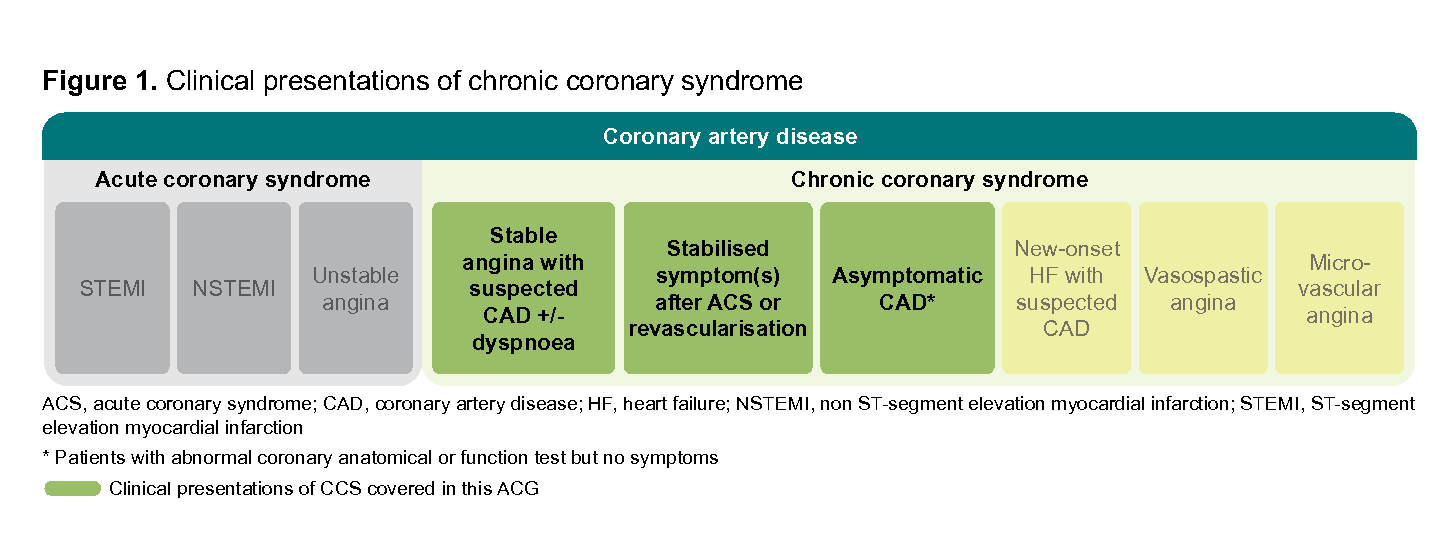
Figure 1. Clinical presentations of chronic coronary syndrome
The primary goals of CCS management are to alleviate symptoms, improve quality of life, and prevent adverse CV events. By doing so, it enhances both the patient’s immediate well-being and their long-term CV prognosis. This is achieved through a combination of pharmacological and non-pharmacological treatment, including lifestyle interventions.
This ACG focuses on the management of patients with established diagnosis of CCS due to coronary artery obstruction (i.e. patients with stable angina with suspected CAD with or without dyspnoea, stabilised symptoms after ACS or revascularisation procedure, and asymptomatic CAD detected through screening). Management of patients with new-onset heart failure and patients with vasospastic or microvascular angina is not discussed in this ACG (see ‘Angina/ischaemia with non-obstructive coronary arteries’).
Notepad: Angina/ischaemia with non-obstructive coronary arteries Management of patients with angina with no obstructive coronary artery (ANOCA) (e.g. vasospastic angina) or ischaemia with no obstructive coronary artery (INOCA) (e.g. microvascular angina) differ from management of patients with CCS due to coronary artery obstruction, and are not covered in this ACG. This distinction is due to the varying pathophysiological mechanisms involved. Notably, antiplatelet therapy is not considered a first-line treatment for patients with ANOCA or INOCA; also, choice of anti-anginal therapy may differ based on pathophysiology. |
Antiplatelet therapy for patients with CCS
Recommendation 1a: Use long-term low-dose aspirin monotherapy for secondary prevention of cardiovascular events
Recommendation 1b: Consider long-term clopidogrel monotherapy as an alternative to aspirin.
Oral antiplatelet therapy is the cornerstone of cardiovascular disease (CVD) secondary prevention.8
Low-dose aspirin
Low-dose aspirin (75–100 mg once daily) is the preferred antiplatelet for patients with CCS, regardless of history of myocardial infarction (MI), due to its efficacy and safety profile.9 The effect of low-dose aspirin for secondary prevention is well-established in the literature.10 Compared to placebo, aspirin significantly reduces serious vascular events, non-fatal MI, non-fatal stroke, and vascular mortality.7, 9-11 Compared to other antiplatelets (e.g. ticagrelor or dipyridamole), aspirin showed similar or non-inferior effects.9, 10
The low dosage is associated with minimal bleeding risk and it is recommended for patients with CCS, including those who have undergone PCI (after a short duration of dual antiplatelet therapy) or coronary artery bypass graft (CABG).6 For patients at high risk of gastrointestinal bleeding, gastric protection with proton pump inhibitors may be required.
a The term CCS is used throughout the ACG in alignment with international literature and recognising the dynamic nature of the condition (i.e. atherosclerotic plaque accumulation and functional alterations of coronary circulation).
Notepad: Patient education aids Click below to access the following patient education aids.
|
Clopidogrel and other P2Y12 inhibitors
Compared to aspirin monotherapy, clopidogrel monotherapy has been found to be associated with a reduction in the risk of CV events such as major adverse cardiac and cerebrovascular events, MI, stroke and major bleeding.12 However, the overall evidence is assessed to be of low quality for most outcomes. Long-term clopidogrel monotherapy is an alternative to aspirin monotherapy — for example for patients with CCS who are intolerant to aspirin or when an alternative is preferred.
When using clopidogrel, consider that:
Depending on types of elective or diagnostic procedures, there may be a need to replace clopidogrel with aspirin for a few days (e.g. 5–7 days) beforehand. This is due to the slightly greater inhibition of platelet function with clopidogrel compared to aspirin, potentially conferring a higher risk of peri-operative bleeding. However, it is important to note that temporary cessation of all antiplatelet therapy in CCS, even for a few days, is associated with an increased risk of thrombotic events. As such, many surgeons or endoscopists may recommend switching from clopidogrel monotherapy to aspirin monotherapy for 5–7 days before the surgery or endoscopy, depending on the risk of procedure-related bleeding. The patient is usually switched back to clopidogrel 12–24 hours after the elective procedure if there is no significant bleeding; check with the proceduralist to confirm bleeding status before switching back. For patients with aspirin intolerance or allergy, consider aspirin desensitisation in consultation with a specialist (e.g. an allergist or immunologist) before temporarily switching to aspirin. Alternatively, if the thrombotic risk is low, consider stopping clopidogrel without aspirin cover (in consultation with a cardiologist).
Premature withdrawal of clopidogrel in patients with recent drug-eluting stent implantation (within past 1–3 months) may be associated with stent thrombosis and potentially fatal consequences;13, 14 seek advice from the cardiologist if non-urgent surgery or diagnostic procedure is required for these patients.
The evidence for other P2Y12 (purinergic receptor P2Y, G-protein coupled, 12 protein) inhibitor (i.e. ticagrelor and prasugrel) monotherapy in patients with CCS is limited. The optimal timing and duration of ticagrelor monotherapy remains unclear due to a lack of long-term data. Similarly, there is insufficient evidence regarding the efficacy and safety of prasugrel monotherapy in patients with CCS.
Notepad: Clopidogrel genetic testing The use of clopidogrel in East Asian populations, particularly in Chinese patients, may be complicated by the high prevalence of CYP2C19 intermediate metabolisers (IMs) and poor metabolisers (PMs). These genetic variations can lead to poor pharmacodynamic and pharmacokinetic effects,15 potentially resulting in suboptimal therapeutic outcomes. While genetic testing for CYP2C19 variants is supported by evidence for patients with ACS, post-stroke, or transient ischaemic attack, its utility for patients with CCS and post-PCI is less established. This limits the overall value of routine genetic testing for CYP2C19 variants before clopidogrel initiation. The decision to test should be individualised, considering the patient’s existing ischaemic and bleeding risk, response to antiplatelet therapy, as well as the cost and availability of the test. |
Recommendation 2: Review patients following PCI to confirm that there is a specified treatment duration for their dual antiplatelet therapy and check with the referring cardiologist if treatment duration is unclear.
Dual antiplatelet therapy (DAPT), combining aspirin with clopidogrel or ticagrelor, is indicated for patients after PCI due to its superior efficacy in preventing thrombosis compared to aspirin monotherapy, despite an increased bleeding risk.16,17
Besides clinical effectiveness, the optimal duration of DAPT is influenced by factors such as procedure-related considerations and the number of stents or stent sites. Therefore, DAPT duration for patients with CCS following PCI is typically determined by the cardiologist performing the procedure or involved in the patient’s care, and communicated to the primary care physician. Overall, recent evidence suggests that in patients after PCI, shortterm DAPT (1–3 months) followed by P2Y12 inhibitor monotherapy could significantly reduce major bleeding risk by 40% compared to 12-month DAPT, without increasing the risk of major adverse CV events, MI, or death.18
Certain clinical scenarios may require shorter DAPT duration than initially specified, necessitating effective communications for collaborative care between primary care and the cardiologist (see ‘Need for further collaborative care’). This approach ensures tailored treatment, minimises risks, and promotes the appropriate clinical care of patients on DAPT.
Notepad: Need for further collaborative care Ongoing collaborative care with the referring cardiologist is recommended for patients on DAPT who develop clinical conditions which may warrant a shorter duration of therapy. This includes patients who have high bleeding risk or those requiring imminent non-cardiac surgery. In such cases, consult the cardiologist to ensure that the DAPT regimen is appropriately tailored to the patient’s current clinical needs, balancing the need to prevent thrombosis against the need to minimise bleeding. |
Oral anticoagulant therapy for patients with CCS and new-onset AF
Recommendation 3a: For patients with new-onset AF with no recent stent (within the past 12 months), consider oral anticoagulant monotherapy based on modified CHA2 DS2 VASc score and patient factors such as comorbidities and bleeding risk.
Oral anticoagulant (OAC) therapy is primarily used to prevent thromboembolic events and reduce stroke risk in patients with atrial fibrillation (AF).7, 11 For patients with CCS who have new-onset AF and no recent stents (within the past 12 months), long-term OAC therapy is recommended, with direct oral anticoagulants (DOACs) generally preferred over warfarin due to improved efficacy and safety.7, 11, 19
Use the modified CHA2 DS2 VASc score (see Box 1) to guide the decision to initiate OAC therapy in patients with CCS who do not have a mechanical heart valve or moderate-to-severe mitral stenosis. OAC therapy is generally recommended for patients with a modified CHA2DS2VASc score ≥2, as the benefits typically outweigh the bleeding risks. However, always consider the individual patient’s circumstances, including both bleeding and thrombotic risks. For detailed guidance on OAC therapy, including dosing recommendations, refer to the ACG Oral anticoagulation for atrial fibrillation.
Box 1. Modified CHA2 DS2 VASc score | |
+1 | Congestive heart failure (clinical heart failure, moderate-to-severe left ventricular dysfunction, or hypertrophic cardiomyopathy) |
+1 | Hypertension |
+1 | Diabetes mellitus |
+2 | Prior stroke or transient ischaemic attack |
+1 | Vascular disease (prior myocardial infarction, peripheral artery disease or aortic plaque |
+1 | Age 65–74 |
+2 | Age ≥ 75 |
Sex category - not counted | |
Caution: In patients with CCS and AF with no recent stents within the past 12 months, OAC therapy alone is sufficient; the addition of antiplatelet therapy to OAC is not recommended. Review the necessity of continuing the patient on antiplatelet therapy together with the OAC as this increases bleeding risk. If there is no indication for antiplatelet therapy aside from CCS, it should be stopped when the OAC is started. |
Recommendation 3b: For patients with new-onset AF and a stent within the past 12 months, consult a cardiologist to reassess and optimise the current antithrombotic therapy.
If a patient with CCS and a stent within the past 12 months develops AF, there is a need to reassess their thromboembolic risk as AF further increases the risk of thromboembolic stroke, potentially necessitating adjustments to the patient’s post-PCI antithrombotic therapy.
The type and duration of antithrombotic therapy will vary depending on the individual patient’s risk of ischaemia and thrombosis versus the risk of bleeding. In general, this may include concurrent OAC and antiplatelet medication. The precise medication regimen and duration (single, dual or triple antithrombotic therapy) will also depend on the timing of the new-onset AF relative to the stent. Consultation with a cardiologist for collaborative care is recommended to individualise and optimise medication therapy.
Management of comorbid or associated conditions
Recommendation 4: Optimise management of comorbid or associated conditions in patients with CCS to reduce overall cardiovascular risk and complications.
While antithrombotic therapy is the cornerstone of CCS treatment, managing other associated or comorbid conditions such as dyslipidaemia, hypertension, diabetes mellitus (DM), chronic kidney disease (CKD), and chronic heart failure (CHF), is crucial to reduce overall CV risk and complications.20, 21 Figure 2 below summarises the management principles for major comorbid conditions more commonly associated with CCS in Singapore.
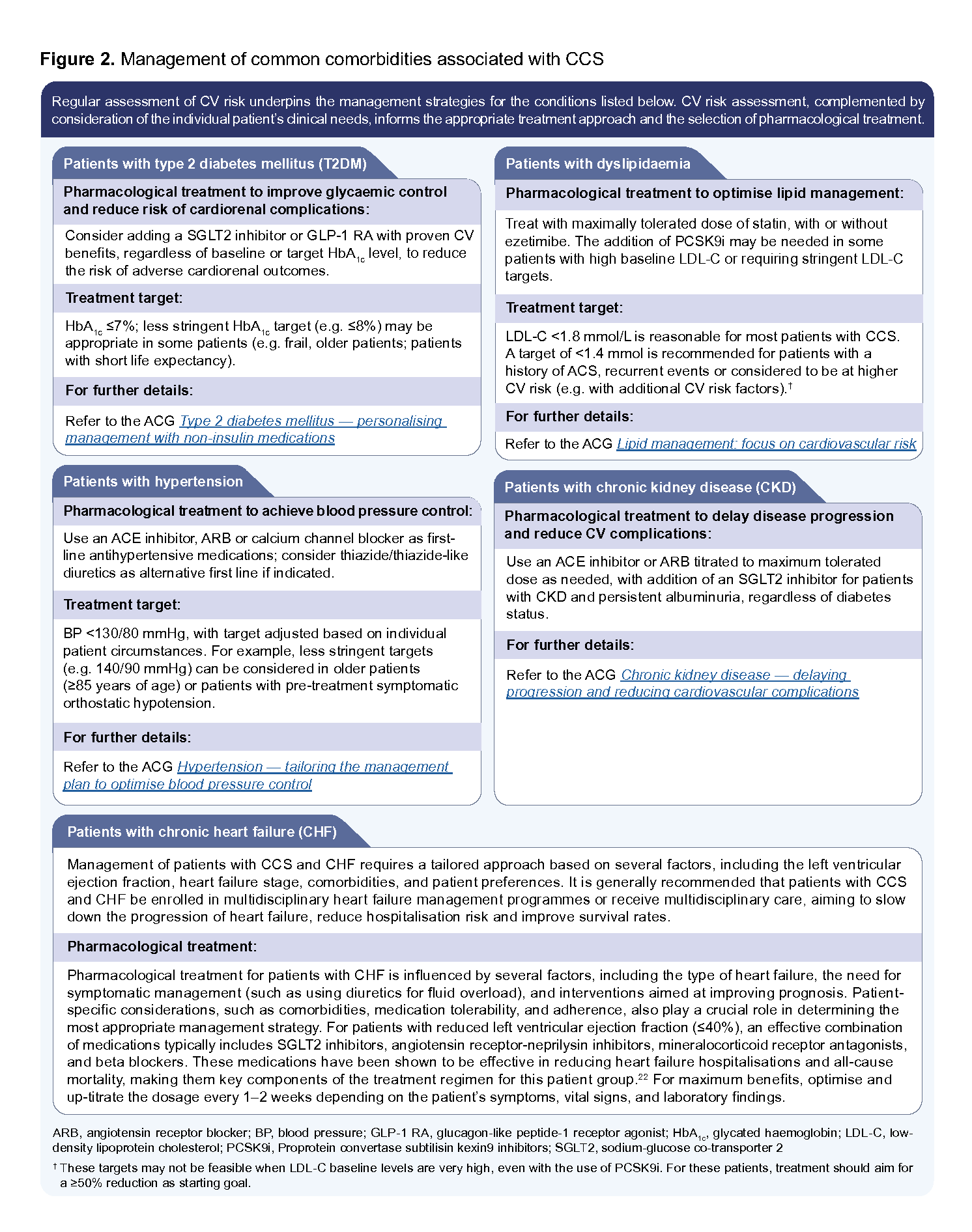
Figure 2. Management of common comorbidities associated with CCS
Click here for larger version of the image
Assessment of acute exacerbation of chest pain in patients with CCS
Patients with established CCS can present with signs and symptoms of acute chest pain (angina). In these circumstances, establishing the origin of the chest pain can be challenging,23 requiring detailed clinical history and assessment of concomitant risk factors. The primary aim of the assessment is to determine whether the chest pain is of cardiac origin, which may indicate an emergency. ‘Typical’ chest pain is more likely to be of cardiac origin and presents with all three of the following features:
Constricting or compressive discomfort in the front of the chest, radiating to the neck, shoulders, jaw, or arms
Precipitated by physical exertion
Relieved by rest or short-acting glyceryl trinitrate within approximately 5 minutes When only (any) two of the above are present, chest pain is defined as ‘atypical’ and is less likely to be of cardiac origin. Figure 3 provides more examples and guidance for differentiating chest symptoms (including dyspnoea) of cardiac versus non-cardiac origin.
When only (any) two of the above are present, chest pain is defined as ‘atypical’ and is less likely to be of cardiac origin. Figure 3 provides more examples and guidance for differentiating chest symptoms (including dyspnoea) of cardiac versus non-cardiac origin.
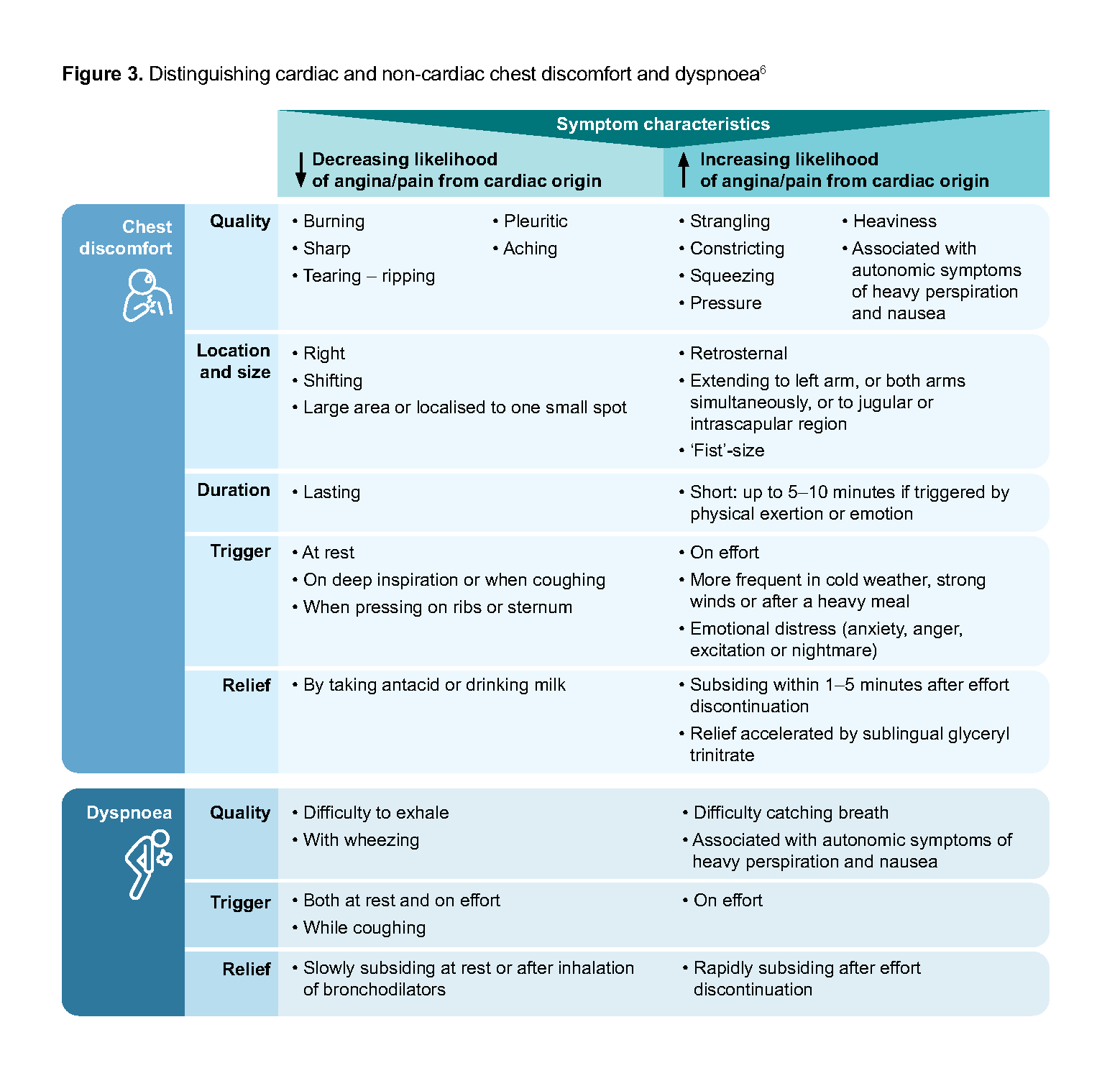
Figure 3. Distinguishing cardiac and non-cardiac chest discomfort and dyspnoea
When chest pain is suspected to be of cardiac origin, a resting 12-lead ECG test can offer baseline assessment at presentation. All patients with CCS with chest pain of suspected cardiac origin should then be offered further investigation or be referred to a tertiary centre or emergency department for more comprehensive assessment. For patients with CCS and atypical chest pain, other possible causes of chest pain including non-cardiac origins should be considered, and managed accordingly, even though the possibility of angina cannot be completely excluded.
Table 1 provides an overview of pharmacological management options for patients with angina. Sublingual or translingual glyceryl trinitate is recommended for immediate, short-term relief of angina or equivalent symptoms. This is typically the first-line treatment for acute anginal episodes.6 Medications used for long-term management and prevention of angina symptoms include beta blockers, calcium channel blockers, long-acting nitrates, ranolazine, ivabradine, and trimetazidine. The choice of medication should be tailored to the individual patient’s hemodynamic profiles (e.g. blood pressure, heart rate), comorbidities (e.g. presence of CHF, or reactive airway disease), concomitant medications with potential interactions, preferences, and treatment response.
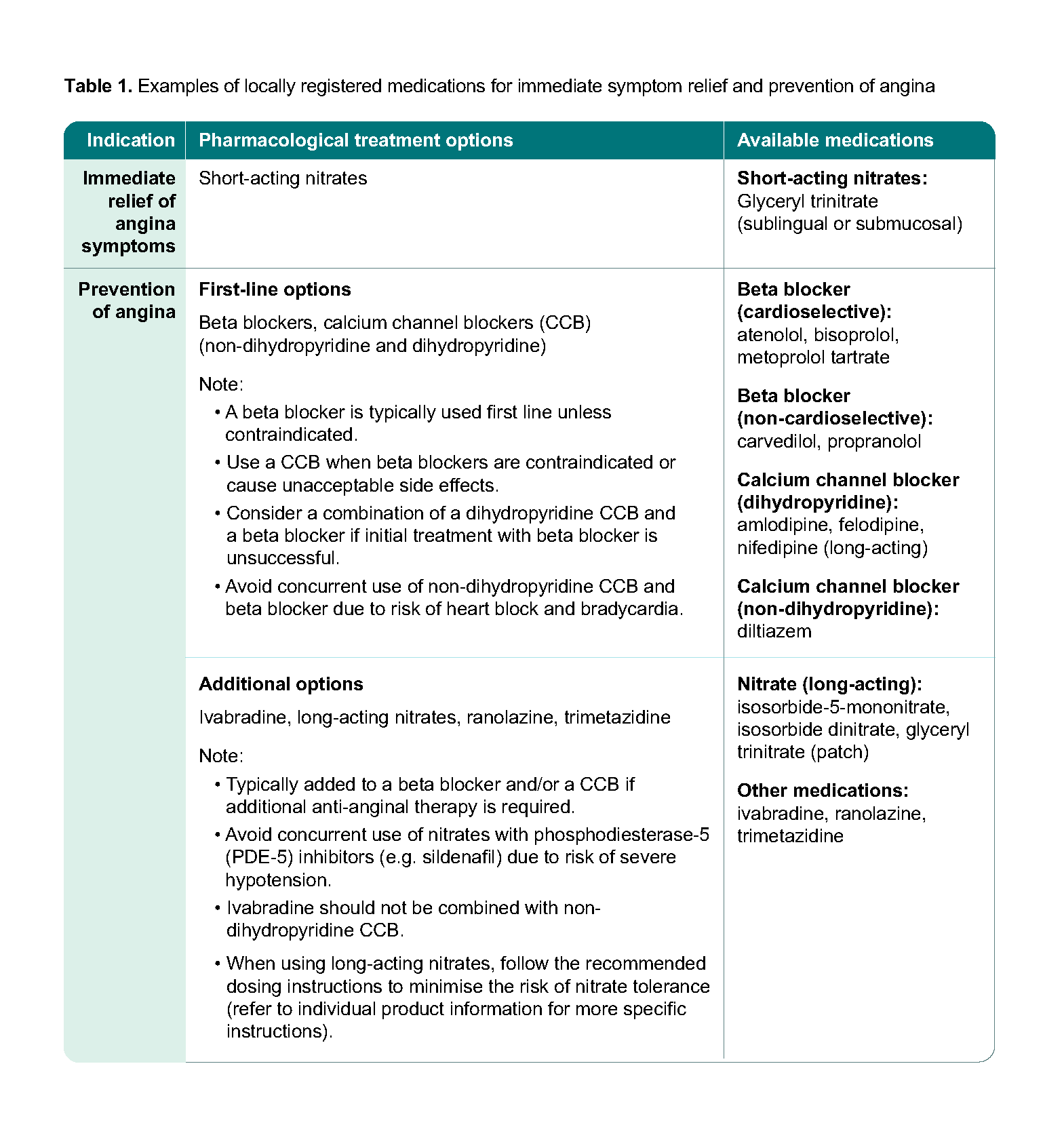
In addition to medications for immediate symptom relief, management of angina in patients with CCS aims to prevent CV events and includes treatment of related comorbidities (e.g. ACE inhibitor or ARB for patients with comorbidities such as hypertension, diabetes mellitus, left ventricular systolic dysfunction, or CKD). See Recommendation 4.
Lifestyle
Recommendation 5: Encourage sustained lifestyle interventions, including regular physical activity tailored to the patient’s capabilities and preferences.
Lifestyle interventions can significantly improve the overall health status of patients with CCS, and their benefits are well established in international guidelines and the literature.6, 11, 24 These interventions warrant a multidisciplinary approach, and include increased physical activity, dietary changes, and smoking cessation. The goals are to enhance patients’ knowledge, self-care abilities, and health-related quality of life.25
Physical activity: Regular physical activity is recommended for patients with CCS as it reduces atherosclerotic risk factors and mortality.26 Appropriate physical activity is considered safe for most patients with CCS (Table 2), except for patients with specific conditions (see ‘Exercise contraindications’).27 Advise patients who do not regularly exercise to consider starting with lower-intensity lifestyle activities exercise and gradually increase frequency, intensity and duration over time.28 |
Table 2. Example of exercise routine
Aerobic exercise | Resistance training |
Recommended at least 3 days per week, preferably 6-7 days per week, with ≥150 minutes of moderate intensity or ≥75 minutes of higher intensity activity weekly or an equivalent combination of both, spread throughout the week. • Activities can include walking, jogging, cycling, and swimming. | • Recommended ≥2 days per week, using 8–10 different exercises involving each major muscle groups such as biceps, triceps, and hamstrings. |
Notepad: Exercise contraindications Exercise is contraindicated in patients with the following clinical conditions, and further assessments or advice from the specialist/cardiologist may be needed:
|
Encourage patients who have attended cardiac rehabilitation programme(s) (e.g. patients after PCI) to continue the recommended physical activities after the programme has ended29 because exercise-based cardiac rehabilitation programmes have been shown to decrease morbidity and mortality.30
Smoking cessation
Tobacco smoke exposure, particularly from cigarette smoking, is a leading cause of CV events in patients with CCS.31-33 Prospective cohort studies of patients with CCS demonstrate that smoking cessation is associated with a 32% reduction in MI,34 and 36% risk reduction in mortality.34 Advise patients with CCS who smoke tobacco to quit at every visit.35 For further details on management of smoking cessation, refer to the ACG on smoking cessation.
Diet
Dietary intake plays a significant role in reducing the risk of CVD in patients with CCS. Lower CVD risk is associated with healthy dietary patterns, including a Mediterranean diet and Dietary Approaches to Stop Hypertension (DASH) diet.36, 37 Adherence to the ‘ethnic breads, legumes and nuts’ and ‘whole grains, fruit and dairy’ patterns was associated with a lower predicted CVD risk in an Asian population.38 Encourage patients with CCS to adopt a diet rich in wholegrain foods, fruits, legumes, and fish. For patients with CCS who consume alcohol, advise them to limit alcohol intake to reduce CV and all-cause death.11, 39
Table 3 below summarises guidance on other lifestyle interventions recommended for patients with CCS.
Table 3. Lifestyle advice for patients with CCS
Body mass index and weight management |
|
Psychosocial aspects |
|
Sexual activity |
|
Patient education |
|
Follow-up and monitoring
Recommendation 6: Schedule regular follow-up visits for all patients with CCS to monitor symptoms, assess medication adherence, and adjust treatment plans as needed.
Patients with CCS who are on antithrombotic therapy should be reviewed regularly for optimal management, even if their condition is stable and asymptomatic. There is limited evidence to guide the frequency of review for patients with CCS. In general, this will depend on:
Severity of the condition
Comorbidities and optimisation of risk factors
Changes in symptoms and functional capacity
Availability of resources
Depending on the considerations mentioned above, the type and nature of assessments and testing at follow-up visits vary, and clinical judgement is required to determine the need for testing or repeated testing. For instance, frequent reviews (e.g. 1-3 monthly) accompanied by appropriate assessments and tests may be considered for some patients with CCS to compare any changes with baseline or previous parameters, such as recently diagnosed patients, patients following PCI, or patients who have received coronary revascularisation.11, 19
During follow-up visits:
Assess overall CV risk factors especially in patients with comorbid conditions (e.g. dyslipidaemia, T2DM).
Review any reported symptoms on exertion and at rest, and their impact on daily activities.
Assess adherence to non-pharmacological advice (e.g. physical activities) and medications.
Remind patients to keep up to date with vaccination against influenza, pneumococcal disease, other widespread infections (e.g. COVID-19).
If required, refer to a tertiary center or specialist for further tests or collaborative care.
Expert group
A/Prof Mark Chan Yan Yee, Cardiology (NUH)
Clin Asst Prof Gilbert Tan Choon Seng, Family Medicine (SHP)
Members
Dr Grace Chang Shu-Wen, Pharmacy (KTPH)
Dr Jennifer Diandra, Family Medicine (NUP)
Prof Derek Hausenloy, Cardiology, (NHCS); CADENCE (NCTP)
Adj A/Prof Foo Chee Guan David, Cardiology (NHGHI)
Dr Vincent Han Xiao, Family Medicine (Bridgepoint Health [Maxwell])
Ms Koh Meng Poh, Nursing (TTSH) Dr William Kristanto, Cardiology (Mount Elizabeth Hospital)
Dr Candice Lee, Family Medicine (NHGP)
A/Prof Francis Lee Chun Yue, Emergency Medicine (KTPH)
Dr Derek Li Shi’An, Family Medicine (Raffles Medical Group)
Clin Asst Prof Moy Wai Lun, General Medicine (Sengkang General Hospital)
Adj Prof Shirley Ooi Beng Suat, Emergency Medicine (NUH)
Dr Kenneth Tan Kian Wee, Family Medicine (Kenneth Tan Medical Clinic)
Ms Tan Su Ching, Pharmacy (NUH)
Clin A/Prof Tay Jam Chin, General Medicine (TTSH)
Dr Teo Lee Wah, Nursing (NHCS)
Feedback
Click here to give us feedback on this ACG.
Related ACGs
Chronic kidney disease — delaying progression and reducing cardiovascular complications
Hypertension – tailoring the management plan to optimise blood pressure control
Type 2 diabetes mellitus — personalising management with non-insulin medications
Other related resources
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation: Agency for Care Effectiveness (ACE). Management of chronic coronary syndrome. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2025. Available from: go.gov.sg/acg-ccs
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.