
Management of knee osteoarthritis – a joint effort with patients ACG
Last updated 14 May 2026
ACE Clinical Guidelines (ACG) provide concise, evidence-based recommendations to inform specific areas of clinical practice and serve as a common starting point nationally for clinical decision-making.
Overview
This ACE Clinical Guideline (ACG) provides evidence-based recommendations on the assessment and non-surgical management of knee osteoarthritis (OA) in adults. Specifically, the ACG covers clinical assessment, mainstay management strategies, pharmacological treatment, involvement of allied health professionals, adjunctive treatments and considerations for specialist referral. The knee OA ACG annex includes validated assessment tools for knee OA, supplementary guidance on flare management and medication tables.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
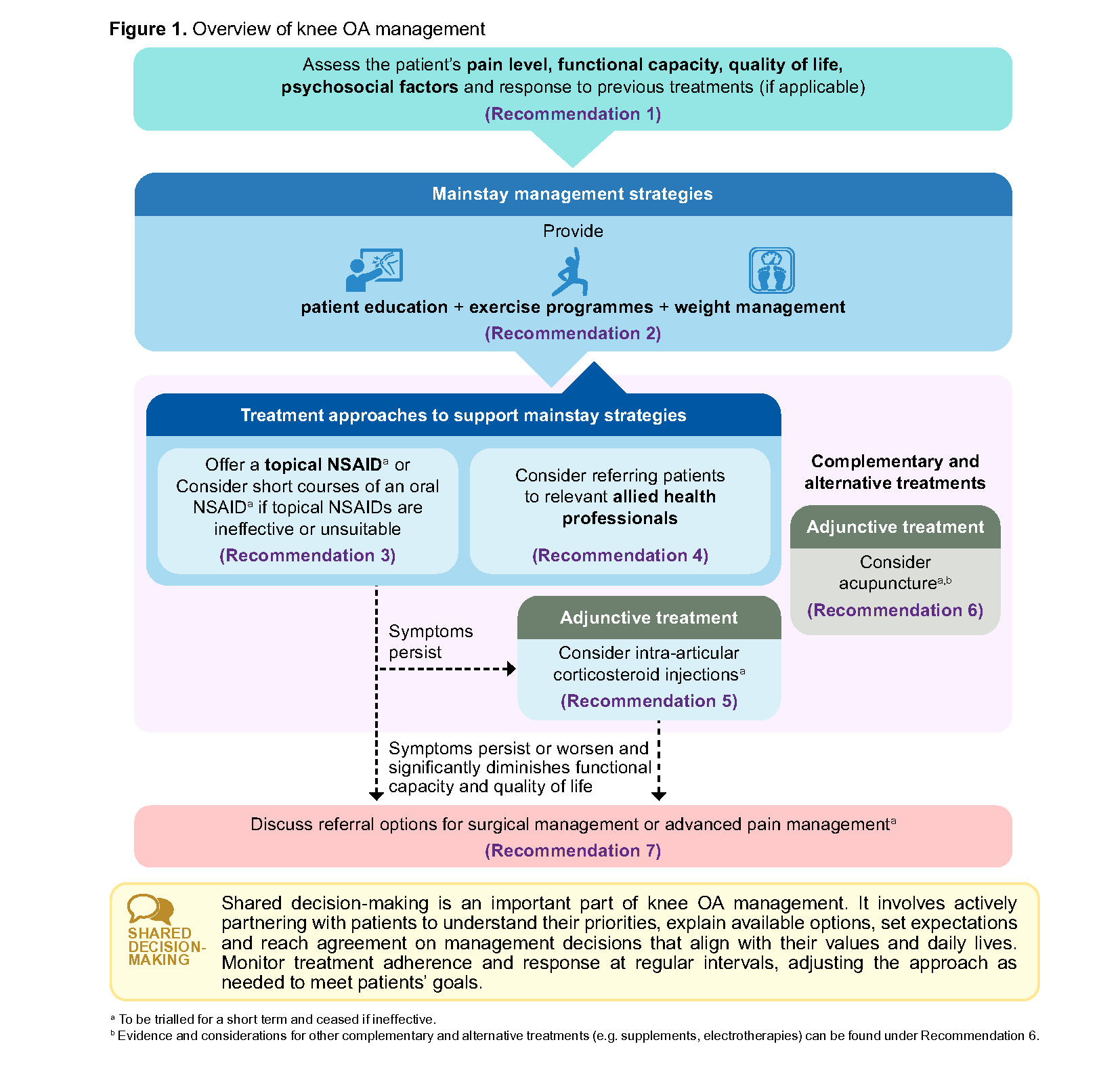
Assess the patient’s pain level, functional capacity, quality of life, psychosocial factors and response to previous treatments (if applicable) to create an individualised management plan.
Provide patient education, exercise programmes and weight management as mainstay strategies for all patients with knee OA, tailoring advice based on individual patient profile.
To complement or support adherence to mainstay strategies for knee OA:
a) Offer a topical NSAID
b) Consider prescribing short courses of an oral NSAID if topical NSAIDs are ineffective or unsuitable
Consider referring patients with knee OA to relevant allied health professionals for additional non-pharmacological strategies (e.g. supervised exercise, walking aids).
Consider intra-articular corticosteroid injections for short-term symptom relief alongside mainstay strategies for knee OA if symptoms persist despite NSAID treatment and/or allied health professional support.
Consider acupuncture as adjunctive therapy for patients with knee OA who have not responded adequately to conventional therapies (e.g. exercise, NSAIDs) or prefer alternative treatments.
For patients with knee OA whose persistent symptoms significantly impact function and quality of life, discuss referral options for surgical or advanced pain management.
Download the ACG and references in PDF
Management of knee osteoarthritis – a joint effort with patients (Apr 2026) [PDF]
Management of knee osteoarthritis – a joint effort with patients references (Apr 2026) [PDF]
Knee OA ACG Annex references (Apr 2026) [PDF]
EtR Framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values, acceptability and other considerations.
Knee OA EtR framework with summary of findings
Request for a hard copy
Click here
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guidance (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Knee osteoarthritis (OA) presents a significant global health burden and is one of the leading causes of disability worldwide.1 Singapore ranks third globally for knee OA prevalence and second for disease burden. In 2021, an estimated 5.8% of the population was affected, with an age-standardised years of life lost due to disability (YLD) of 189 per 100,000 people.2 This burden is projected to increase in the coming decades due to an ageing population and rising rates of sedentary lifestyle and obesity. The economic impact is also considerable, with the local total burden of knee OA estimated at $1.37 billion in 2021.3
Effective non-surgical management strategies are available to manage knee OA. However, many patients either do not receive these interventions (e.g. tailored patient education, exercise programmes, referrals to allied health professionals) before considering surgical management,4-6 or there is poor adherence.7 For example, a local study found that less than half of the patients with knee OA received information on non-steroidal anti-inflammatory drugs (NSAIDs) for knee pain; were assessed for walking difficulties; or were referred for weight management.4
This ACE Clinical Guideline (ACG) provides evidence-based recommendations for managing knee OA in primary care settings, focusing on conservative strategies and highlighting criteria for specialist consideration.
Once regarded as a degenerative ‘wear and tear’ condition, knee OA is now recognised as a complex, multifactorial disorder characterised by tissue breakdown and abnormal cellular changes of the entire joint.8 The condition arises from cumulative exposure to various risk factors and age-related structural changes, with progression accelerated by modifiable factors including obesity and sarcopenia.5
These changes are associated with clinical features such as joint pain, stiffness, functional impairment, crepitus and restricted range of motion. However, the severity of symptoms does not consistently correlate with the extent of structural abnormalities. In addition to peripheral nociceptive drivers arising from joint pathology, alterations in central sensitisation mechanisms may also contribute to pain perception and persistence in some individuals.5
Management of knee OA centres largely on non-pharmacological strategies. While primary care clinicians play a key role in managing knee OA, multi-disciplinary management involving physiotherapists, occupational therapists and other healthcare professionals enables comprehensive care to be delivered and reinforced consistently.
Figure 1 provides an overview of knee OA management to prevent disease progression and facilitate ongoing care in community settings. Many patients can achieve effective symptom control using non-surgical management strategies, although there is no standard treatment combination. Shared decision-making enables clinicians and patients to determine if selected treatments are effective and aligned with patient goals. Previously effective treatments may become less so over time and/or no longer align with patient goals, and vice-versa.9
Recommendation 1: Assess the patient’s pain level, functional capacity, quality of life, psychosocial factors and response to previous treatments (if applicable) to create an individualised management plan.
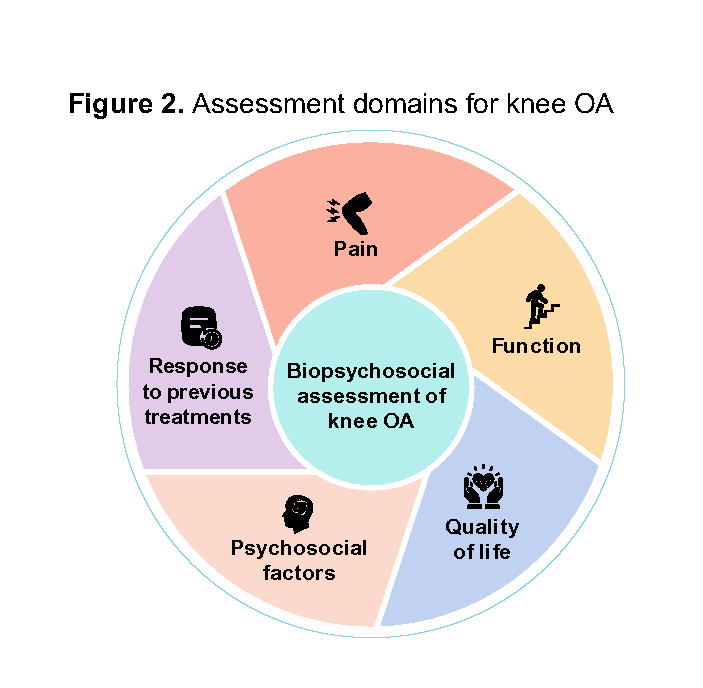
Patients with knee OA often present with debilitating symptoms, most commonly joint pain, alongside functional limitations.10 While pain and function are two primary assessment domains for knee OA, an effective biopsychosocial assessment should also include quality of life and psychosocial factors (Figure 2). This holistic approach recognises that knee OA affects social participation, mental health and overall life satisfaction, and ensures that treatment benefits can be measured using outcomes that matter most to patients.11
Psychosocial factors like kinesiophobia, pain catastrophising, depression and poor sleep can negatively influence how patients perceive their pain and functional limitations, and affect adherence to mainstay strategies (see Recommendations 2 and 4).12
A comprehensive biopsychosocial assessment enables clinicians to provide personalised care by:
Prioritising interventions based on the patient’s most significant problems and response to previous treatments
Setting realistic, patient-centred goals
Monitoring progress effectively by having clear baseline measurements
This comprehensive assessment can be complemented by the use of validated tools which assess the various domains shown in Figure 2 (see Annex A for examples of validated tools).
Notepad: Red flags and atypical symptoms The findings below may suggest a need for alternative or additional diagnoses and specialist evaluation (e.g. rheumatologist, orthopaedic surgeon):13
|
Notepad: Limited role for imaging Knee OA is primarily diagnosed clinically. Imaging plays a limited role in diagnosing and monitoring knee OA progression due to the poor correlation between radiographic findings and clinical symptoms. Therefore, reserve imaging for patients presenting with atypical symptoms, red flags or pre-surgical planning.14-16 |
Mainstay management strategies
Recommendation 2: Provide patient education, exercise programmes and weight management as mainstay strategies for all patients with knee OA, tailoring advice based on individual patient profile.
Patient education
Patient education is a core component of knee OA management and works synergistically with other treatment approaches such as exercise and weight management to provide greater benefits on pain and function compared to a single approach.17-19 Combined education and exercise programmes can be a cost-effective approach to improve pain and quality of life while reducing the need for surgery by 10–30%.20-23
Notepad: Educating patients about knee OA – communicating clearly and effectively Use clear, consistent and empathetic communication when explaining knee OA progression and management principles:
Click here to access local patient education leaflets on knee OA: Knee OA (HealthHub), Knee OA (SingHealth) |
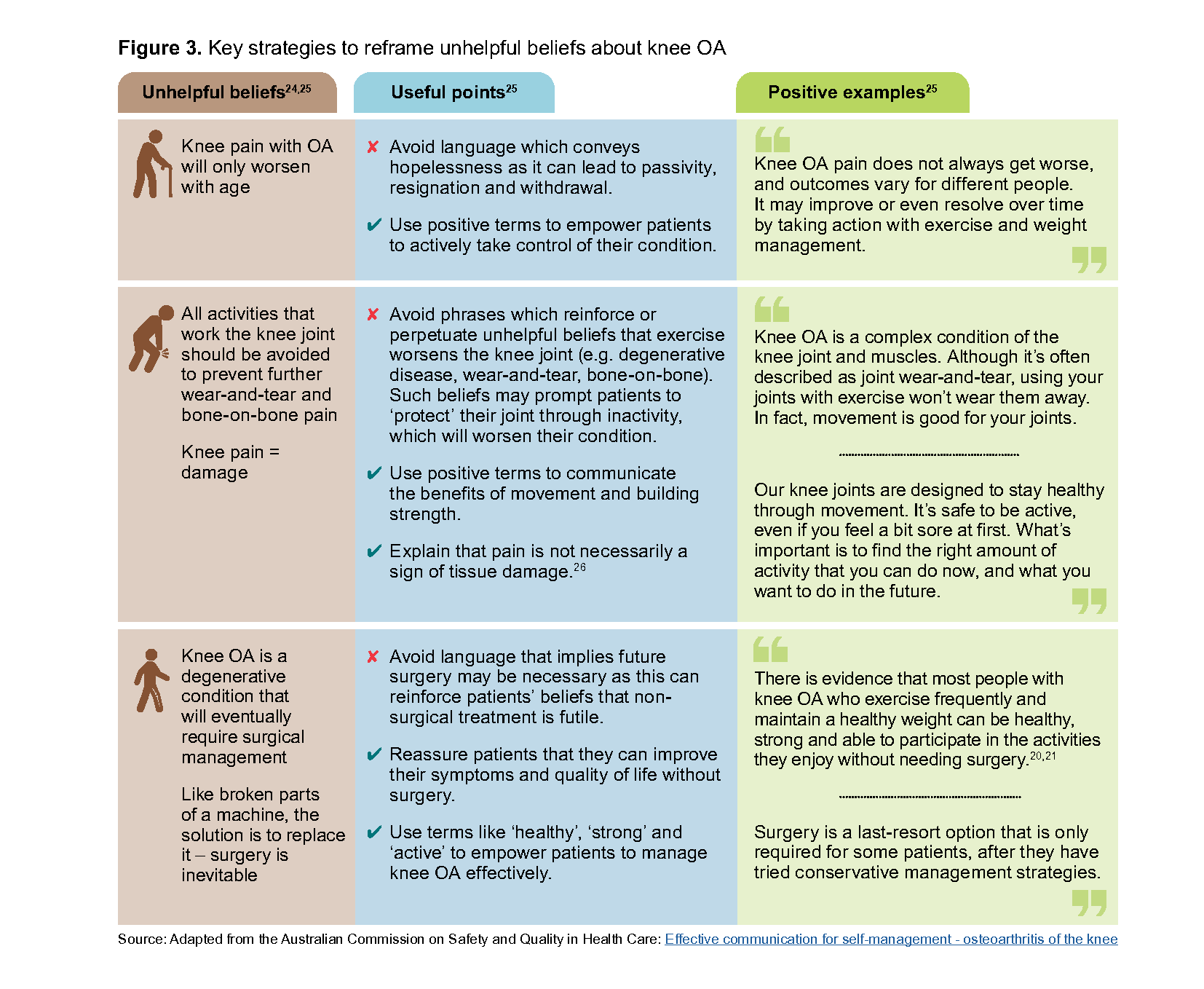
Besides information from clinicians, patients’ perception of knee OA may be shaped by other sources of information and their own lived experiences.24 Knee OA is often viewed as a condition defined by joint degradation and inevitable decline, which can discourage adoption of exercise and/or weight management programmes.24 Clinicians play an important role in reframing the narrative around knee OA – empowering patients to take active steps in managing their symptoms (Figure 3).
Exercise programmes
Exercise provides sustained benefits for pain reduction and functional improvement.17,27-29 While some guidelines recommend specific low-impact exercises like walking, muscle strengthening, Pilates, tai chi or hydrotherapy, there is currently insufficient evidence to recommend one form of exercise over another.16,28,30,31
Consider incorporating various exercise types into exercise programmes, including aerobic, strengthening, neuromuscular training, flexibility and balance training.32 While it is best to select exercises which directly address individual impairments or functional limitations,32 it may be more important overall to recommend an exercise programme which patients find acceptable and affordable to increase the chances of treatment adherence.
High-impact exercises like running may also be safe for most patients with knee OA. Recent evidence indicates that running does not worsen symptoms or disease progression, provided patients can tolerate temporary exercise-related discomfort and have a longer recovery period between each run.33,34 For patients with obesity or overweight, low-impact exercises can be considered to reduce excessive joint loading until weight improves.
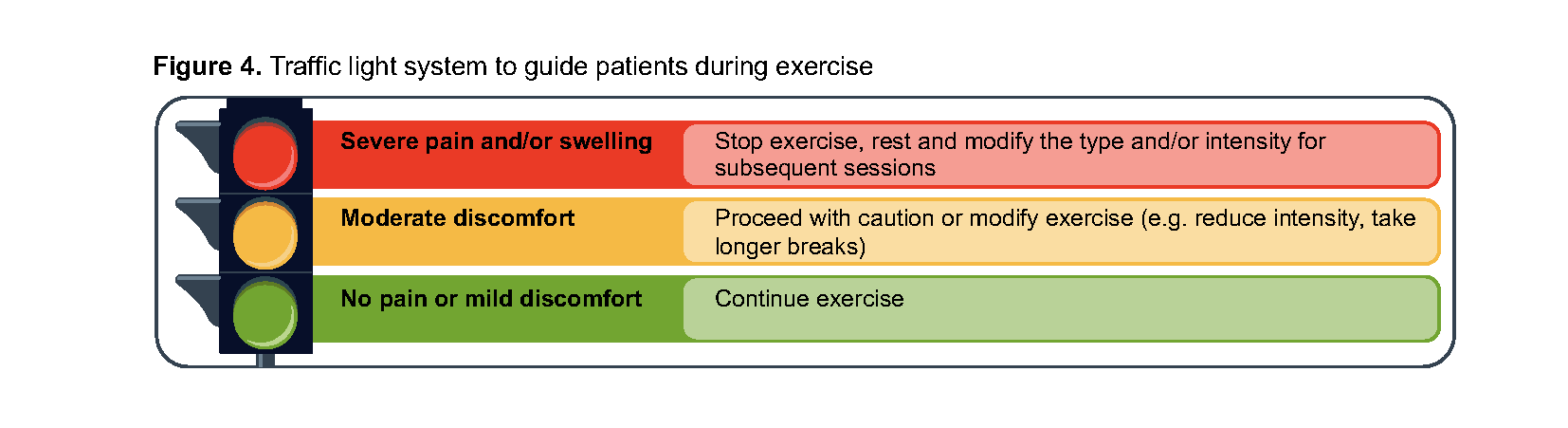
Exercise risks are mostly minor and involve transient increased pain and swelling at the affected knee joints.16,30 Reassure patients that despite the possible temporary pain, exercise is not harmful to the knee joints and will be beneficial in the long run to reduce pain (Figure 3), improve functional capacity and quality of life.15
When used appropriately, wearing knee braces during exercise or weight-bearing activities can be beneficial for short-term pain relief and functional improvement,35-37 without causing muscle atrophy.38,39 They only need to be worn for activities that precipitate symptoms, or during flares (see Annex B). Consider referral to allied health professionals to optimise knee brace selection and use, when appropriate.
Encouraging exercise
Click here to access local exercise resources for knee OA: Click here for examples of community exercise programmes: |
Weight management
Weight management encompasses weight loss, weight maintenance and prevention of weight gain.44 Obesity is a modifiable risk factor for knee OA development and progression, where systemic inflammation and increased mechanical joint loading contribute to pain and reduced function. Like exercise, weight loss can improve pain levels and disability, with greater pain relief observed when combining weight loss with patient education.45
For patients with knee OA who have obesity or overweight:
Weight loss may be achieved through a combination of psychological support, diet, exercise and/or medications.46
Every 1 kg of body weight lost results in a four-fold reduction in the load on the knee joints.
Gradual weight loss of 5–10% over 6–12 months is manageable and provides significant improvements in pain, function and quality of life, with greater weight loss providing progressively larger benefits.47-49
Click here to access local tips on weight management: Tips for successful weight management (HealthHub)
Notepad: A slow and steady approach Advise patients who have obesity or overweight to adopt strategies which promote gradual and sustainable weight loss, complemented by resistance training and adequate protein intake to preserve muscle mass. Discourage rapid or excessive weight loss, which is associated with risks like joint instability, muscle and bone loss, malnutrition and osteoporosis.50 Long-term weight loss maintenance also remains a challenge, with high rates of weight regain observed in patients with OA.50 Encourage them to persist in maintaining a healthy weight to minimise symptoms from returning. |
Treatment approaches to support mainstay strategies
Recommendation 3: To complement or support adherence to mainstay strategies for knee OA: a) Offer a topical NSAID; b) Consider prescribing short courses of an oral NSAID if topical NSAIDs are ineffective or unsuitable
The primary role of pharmacological treatment is to provide symptomatic relief so that patients can continue engaging in exercise and weight management programmes.
Offer topical NSAIDs first
Topical NSAIDs are strongly recommended for knee OA due to their favourable benefit and safety profile.14,15,27,28,51 Compared to paracetamol, topical NSAIDs show similar improvements for pain and better outcomes for functional improvement and safety, with only mild local skin reactions and lower risks of gastrointestinal (GI) adverse events.52 Topical NSAIDs are as efficacious for pain and functional improvement as oral NSAIDs, but carry less than half the risks for GI adverse effects due to lower systemic exposure.52 However, topical NSAIDs are not risk free, hence they should be used only when needed for the shortest possible duration and at the lowest effective dose.
Comparative efficacy and safety of oral NSAIDs
Both non-selective NSAIDs (nsNSAIDs) and cyclooxygenase-2 (COX-2) inhibitors provide comparable improvements in pain and function.16 Although evidence suggests that etoricoxib 60 mg/day and diclofenac 150 mg/day may be the most effective for improving pain and function in OA compared to other oral NSAIDs, paracetamol and opioids,53 the choice of oral NSAID should take into consideration risks and adverse effects, patient comorbidities, previous treatment response, patient preferences and cost (see Annex C).
Risks associated with oral NSAIDs
GI risks are present for all oral NSAIDs, with COX-2 inhibitors having lower risks than nsNSAIDs. Concurrent proton pump inhibitor (PPI) with nsNSAIDs can reduce GI risks (to a similar level as COX-2 inhibitors).54 Patients who may benefit from gastroprotective strategies (such as concurrent PPI therapy) include those:
With history of GI bleeding or peptic ulcers
Requiring high-dose NSAIDs
Aged >65 years
Concomitantly using medications with increased risk of GI effects (e.g. antiplatelet medications, anticoagulants, oral corticosteroids)
Oral NSAIDs’ cardiovascular (CV) risks are dose- and duration-dependent: CV risks rise within weeks of starting oral NSAIDs, except for naproxen which does not show this association.55,56 Of note, COX-2 inhibitors, high-dose diclofenac (150 mg/day) and high-dose ibuprofen (2,400 mg/day) may carry higher risks for vascular death, non-fatal MI or stroke, but not naproxen and low-dose ibuprofen.56
Notepad: Considerations for patients taking aspirin For patients taking aspirin for secondary prevention of conditions such as chronic coronary syndrome or stroke, avoid NSAIDs like ibuprofen and naproxen as they may weaken aspirin’s cardioprotective effects.57 Conversely, oral NSAIDs with high COX-2 selectivity like etoricoxib and diclofenac are unlikely to interfere with aspirin’s cardioprotective effects as they do not significantly inhibit COX-1;58 these may be more appropriate choices if an oral NSAID is required, depending on the patient’s comorbidities and other risks (see Annex C). |
Treatment duration and monitoring of oral NSAIDs
The analgesic effects of oral NSAIDs can begin within two hours of starting treatment and peak after two weeks, but diminish after eight weeks.59 Given that adverse effects may appear after four weeks of treatment,59 NSAIDs should be used only when needed for the shortest possible duration and at the lowest effective dose. Patients should be counselled against taking NSAIDs if they do not experience symptoms, and clinicians should review treatment effectiveness and consider alternative options if NSAIDs fail to provide adequate symptom relief within several weeks.
Limited role for paracetamol and opioids
While paracetamol is generally considered safe and serves as the first-line analgesic in the pain management ladder, its effectiveness in knee OA is limited. Paracetamol provides minimal improvements in pain and function compared to placebo in patients with knee OA.60 If paracetamol is used, it should be prescribed at the lowest effective dose for the shortest possible duration, due to the risk of hepatotoxicity particularly with prolonged high-dose use. Its use should typically be reserved for specific circumstances, such as when NSAIDs are unsuitable for patients.15,17
Opioids, including weaker ones like tramadol, are strongly discouraged for knee OA due to marginal benefits for pain and function when compared to placebo.14-17,28,53,61-63 The significant long-term safety risks – including dependency and increased mortality – make their risk-benefit profile particularly unfavourable for managing knee OA, especially in those with multiple chronic medical conditions.64
Notepad: Limited role for duloxetine in knee OA (off-label indication) Duloxetine is a serotonin and noradrenaline reuptake inhibitor (SNRI) which provides small improvements in pain, function and quality of life for some patients with knee OA with persisting symptoms despite NSAID treatment, particularly for those whose pain is modulated by central sensitisation, neuropathic pathways or psychosocial factors.65,66 However, duloxetine is currently not registered in Singapore for knee OA treatment (i.e. off-label use), and its adverse effects may lead to treatment discontinuation.65,66 If offered, duloxetine should be trialled as short-term adjunctive therapy and ceased if ineffective.16,17,28 |
Recommendation 4: Consider referring patients with knee OA to relevant allied health professionals for additional non-pharmacological strategies (e.g. supervised exercise, walking aids).
Physiotherapy and supervised exercise
Although exercise is an important mainstay strategy with significant benefits for knee OA (see Recommendation 2), exercise adherence may be suboptimal due to patient factors like negative beliefs, limited social support and environmental constraints.67 Physiotherapists can help address these barriers by reinforcing the importance of exercise programmes and further personalising exercise programmes by ensuring correct techniques and incrementally adjusting difficulty levels based on patient response.32 Supervised exercise by physiotherapists also produces greater improvements in pain and function compared to home-based programmes.68
Clinicians may refer patients to physiotherapists either alongside or after pharmacological treatment initiation (Figure 1) based on the patient’s symptoms, ability to adhere to exercise programmes and preferences. Early referral is particularly beneficial for patients experiencing functional limitations, muscle weakness, restricted range of motion or difficulties with self-directed exercise programmes.14-17,27,51,69 These patients often benefit more from supervised exercise and tailored instructions, which can improve treatment adherence and knowledge for effective self-management.
Click here for information about community physiotherapy programmes: Community rehabilitation (AIC)
Referral to other allied health professionals
Depending on patient needs and risk factors, clinicians can refer patients to other allied health professionals:
Patients with functional difficulties can benefit from referral to occupational therapists, for evidence-based assistive devices that offer stability and reduce weight burden to improve functional capacity and quality of life.
Patients who require additional support and nutritional guidance for weight management can benefit from referral to dietitians, especially if they have obesity, concurrent metabolic disease or those with multiple unsuccessful weight loss attempts.
Patients with psychosocial risk factors can benefit from referral to psychologists, for interventions such as cognitive behavioural therapy to provide additional improvements in pain, function, insomnia and depression.70,71 For guidelines on management of mental health conditions in primary care, refer to the ACGs on major depressive disorder and generalised anxiety disorder.
Adjunctive treatments
Recommendation 5: Consider intra-articular corticosteroid injections for short-term symptom relief alongside mainstay strategies for knee OA if symptoms persist despite NSAID treatment and/or allied health professional support.
Intra-articular corticosteroids (IA CSs) should be reserved for patients whose symptoms persist despite treatment with NSAIDs and allied health professional support, to enable them to continue adhering to exercise and/or weight management programmes. IA CSs also provide an option for patients for whom NSAIDs are unsuitable, or patients unsuitable for surgical management.
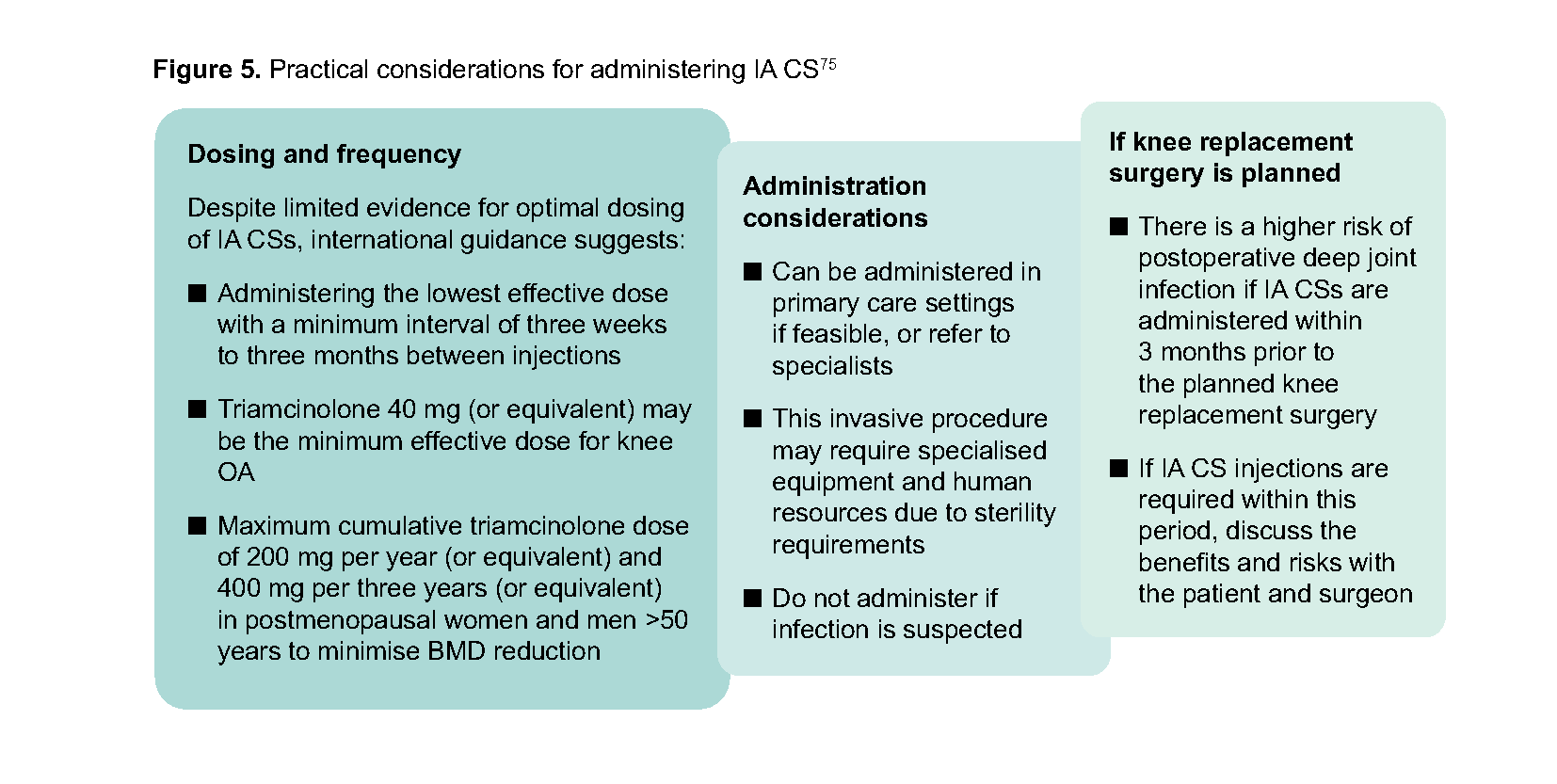
IA CSs such as triamcinolone may provide the most significant pain relief compared to other intra-articular therapies for knee OA, with benefits similar to NSAIDs for pain and function for up to 24 weeks.72-74 However, physiotherapy and exercise produce better long-term functional improvements. IA CSs are also associated with risks like elevated blood glucose levels, adrenal suppression and bone mineral density (BMD) reduction.75 Furthermore, mixed evidence suggests that multiple IA CS injections may be associated with knee cartilage loss on radiological imaging.61,76
Ensure that patients understand that IA CS injections serve as a temporary pain relief measure to complement the exercise and/or weight management programmes; it is not a standalone long-term treatment.
Notepad: Other intra-articular therapies Intra-articular hyaluronic acid (IA HA) IA HA, also known as viscosupplementation, represents the second most prescribed IA intervention for knee OA.73 IA HA is proposed to yield benefits through chondroprotection and anti-inflammatory effects.77 However, IA HA has not resulted in significant improvements in pain and function compared to placebo, IA CS or other intra-articular therapies, and may carry a higher risk of adverse events including acute knee swelling or pain.73 Platelet-rich plasma (PRP) PRP is a biological therapy for knee OA, with potential benefits including promoting cartilage repair and modulating knee inflammation.78 However, PRP resulted in no significant difference in pain and functional improvement compared to IA CS, with most adverse events being mild and transient.78 The lack of standardised PRP preparations and uncertainty over the evidence base further limits its use for knee OA.17,28 Stem cell injections Stem cell therapy represents another biological treatment approach based on the principle that stem cells can develop into mature cells to help regrow damaged joint cartilage and slow down disease progression. While stem cell injections may provide slight improvements in pain and function compared to placebo, uncertainty remains regarding their benefits over IA CS, efficacy in slowing disease progression, and overall safety profile.79 Use of intra-articular therapies listed above may incur additional costs without established clinical benefit for knee OA. If used, they should be trialled for a short, defined period and ceased if ineffective. |
Recommendation 6: Consider acupuncture as adjunctive therapy for patients with knee OA who have not responded adequately to conventional therapies (e.g. exercise, NSAIDs) or prefer alternative treatments.
Acupuncture, a Traditional Chinese Medicine (TCM) treatment involving the stimulation of specific acupoints by trained practitioners, may be considered as an adjunct to conventional knee OA treatment. Acupuncture reduces inflammation and provides modest improvements in pain and function with fewer adverse effects than NSAIDs, though the quality of evidence remains variable.80 Different acupuncture techniques show varying effectiveness. Electroacupuncture appears most effective for pain relief compared to other acupuncture techniques, and celecoxib.81,82 For improving function, warming acupuncture and electroacupuncture may be more effective than manual acupuncture.81,82 The modality, duration and frequency of sessions is left to the clinical discretion of the TCM practitioner.
Acupuncture is generally considered safe, with minor temporary adverse events including pain during needle insertion, post-insertion soreness, and local bruising.
Practical considerations for acupuncture
|
Notepad: Other complementary and alternative treatments Oral supplements Glucosamine and chondroitin are common supplements purported to relieve joint pain and slow cartilage loss. However, evidence regarding their efficacy remains uncertain due to varying formulations and inconsistent study results. There is conflicting evidence on whether they have benefits for pain and function compared to placebo,83,84 and adding them to exercise produced no significant benefit.85 Although considered safe with mild GI adverse effects, their use may add cost without established clinical benefit for knee OA. Herbal supplements like Boswellia serrata formulations may have benefits for knee pain and function with a good safety profile, though certainty in these findings is limited and more robust evidence is needed to ascertain its effectiveness.86,87 If prescribed, these supplements should be trialled for a short term and ceased if ineffective. Electrotherapies Electrotherapies including transcutaneous electrical nerve stimulation (TENS), interferential current, extracorporeal shock wave therapy and laser therapy may be less effective than conventional therapies like exercise for managing pain and function.36 Evidence remains unclear on the benefits of TENS for pain and function for patients with knee OA due to low quality of evidence and small sample sizes, though adverse effects like skin irritation are typically mild and infrequent.88-90 |
Specialist referral
Recommendation 7: For patients with knee OA whose persistent symptoms significantly impact function and quality of life, discuss referral options for surgical or advanced pain management.
Clinicians should discuss potential referral options when:
Patients continue to experience symptoms – including significant joint pain, swelling and deformity – despite conservative management; and
Function and quality of life are significantly impacted, such as disrupted sleep or impaired ability to perform activities of daily living; and
Duration of the above is lasting at least 3–6 months5,91
Surgical management
Surgical management (e.g. total knee replacement, unicompartmental knee replacement) can yield positive outcomes for pain, function and quality of life for patients with moderate-to-severe knee OA.92 However, these benefits should be balanced against risks associated with surgical intervention and cost considerations.3,4 Surgical management should only be considered after conservative interventions have been exhausted, with the most appropriate surgical approach determined by the surgeon based on patient factors and preferences.
When considering orthopaedic referral, discuss expectations and risks of surgical management,93 particularly whether surgery can realistically meet patients’ goals. Pain relief and restoration of range of motion following surgery is not guaranteed, with studies reporting that 10–34% of patients experience long-term pain, and 1–7% experience stiffness after total knee replacement.5,94 However, a local study found that fulfilling patient expectations provided significant improvements in pain, function and satisfaction after surgery.95 This finding highlights an opportunity for clinicians to enhance surgical and patient outcomes by actively managing patient expectations before surgery.
Patient education on surgical management Provide general information on knee surgery to help patients manage their expectations
Inform patients that possible risks of surgery include:
|
Advanced pain management
For patients who have exhausted conservative approaches but are ineligible for surgical management, prefer to avoid it, or are awaiting surgery, referral to pain medicine physicians for advanced non-surgical approaches offers an alternative. Patients reporting significant and persistent knee pain may benefit from specialised therapies like genicular nerve block or genicular nerve radiofrequency ablation, which are advanced options to improve pain and function.97,98
Expert group
Chairpersons
Dr Koh Kim Hwee, Family Medicine (SHP)
Dr Ng Yau Hong, Orthopaedics (Raffles Orthopaedic Centre)
Members
Ms Chen Zhen Zhen, Occupational Therapy (NUH/CAHOO)
Mr Gary Cheok, Physiotherapy (NHGP)
Dr Elaine Chua, Family Medicine (Bedok Medical Centre)
Dr Lau Kah Yong, Traditional Chinese Medicine (NTU)
Dr Ong Say Yang, Pain Medicine (NUHS)
Ms Soh Wee Teng, Pharmacy (Watsons)
Dr Bryan Tan, Orthopaedics (WHC)
Dr Kenneth Tan, Family Medicine (Kenneth Tan Medical Clinic)
Dr Tay Yoong Chuan, Pain Medicine (SGH)
Dr Veronica Teo, Pharmacy (NTFGH)
Ms Wang Chunyan, Nursing (NHGP)
Dr Ryan Wong, Family Medicine (OneDoctors Family Clinic [Holland Village])
Dr Frederick Yeo, Family Medicine (NHGP)
Ms Zhang Qinyi, Nursing (SHP)
Dr Zhang Zhi Peng, Family Medicine (NUP)
For more information on the Expert Group composition and other details, click here.

ACG survey and feedback
We invite all readers of the ACGs to complete this survey. The survey aims to understand the impact of the guideline on clinical confidence, decision-making, and practice. Results will contribute to informing future guidelines and implementation support for you. Your responses will remain confidential and will be analysed in aggregate to safeguard your privacy. The survey takes approximately 10–15 minutes to complete and will remain open for four weeks until 23 May 2026. We highly encourage you to complete the survey after reading the ACG.
Feedback
Click here to give us feedback on this ACG
ACG annex
Click below to see the list of references and other information.
Knee OA ACG Annex (Apr 2026) [PDF]
Expert Group details
Knee OA ACG EG composition and other details (Apr 2026) [PDF]
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Management of knee osteoarthritis – a joint effort with patients. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2026. Available from: go.gov.sg/acg-kneeoa
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.