
Hypertension – tailoring the management plan to optimise blood pressure control ACG
Last updated 21 May 2026
Published on 15 Dec 2023
Overview
This ACE Clinical Guideline (ACG) highlights the importance of clinical assessment and management of elevated blood pressure to reduce risk of cardiovascular disease. The ACG offers evidence-based recommendations on assessing cardiovascular risk and optimising blood pressure control through pharmacotherapy, with considerations for appropriate selection of first-line antihypertensives in context of associated conditions. Principles of lifestyle intervention, strategies to encourage adherence, considerations for intensification of medications, home blood pressure monitoring, and regular follow-up are also discussed. An additional resource on the updated Singapore-modified Framingham Risk Score supplements the ACG.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Include cardiovascular risk assessment to inform management options for patients with elevated BP.
Use an ACE inhibitor, ARB, or CCB as first-line antihypertensive medications; consider thiazide/thiazide-like diuretics as alternative first-line if indicated.
Avoid initiating beta blockers (BBs) as first-line monotherapy for BP control unless BB use is expected to have favourable effect on patient comorbidities.
Consider initiating low dose dual therapy from two different antihypertensive medication classes based on required BP reduction and cardiovascular risk.
Intensify antihypertensive medications to optimise BP control if response to initial treatment is not achieved as expected (e.g. within three months).
Follow up all patients with hypertension at least every six months, with more frequent review as needed.
Download the ACG and reference
Hypertension – tailoring the management plan to optimise BP control (Dec 2023) [PDF]
Hypertension – tailoring the management plan to optimise BP control references (Dec 2023) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Hypertension is a highly prevalent risk factor for the development of cardiovascular disease (CVD), affecting an estimated 1.28 billion people worldwide.1 In Singapore, the 2022 National Population Health Survey reported that over one in three residents (37%) aged 18 to 74 years had hypertension, and that more than half of this group (53%) were previously undiagnosed.2 Without appropriate management, hypertension can lead to complications such as stroke, ischaemic heart disease, heart failure, and kidney damage, which are all associated with premature morbidity and mortality.
A comprehensive assessment that incorporates cardiovascular risk is essential for informing prognosis and treatment options for patients presenting with hypertension. This assessment is also a useful communication tool to help patients understand the importance of managing their elevated blood pressure (BP).3
Accurate diagnosis of hypertension is important, as management is often lifelong and can involve multiple medications. Definitions used in this clinical guideline are based on clinic BP readings as follows:
Grade 1 hypertension and above: BP ≥140/90 mmHg
High-normal BP: BP ≥130–139/85–89 mmHg
Recommendations in this clinical guideline apply to any patient with clinic BP ≥130/85 mmHg (elevated BP), which includes both those diagnosed with hypertension (Grade 1 and above) and those identified with high-normal BP.
Notepad: Clinic and non-clinic BP readings Clinic BP readings may differ from those taken in non-clinic settings. This should be considered when diagnosing or managing hypertension, including when setting BP targets. For example, a clinic BP of 140/90 mmHg would correspond to a home BP of 135/85 mmHg. For more information on these differences, see ‘ A general reference for corresponding values of clinic and non-clinic BP readings’ below. |
|---|
Assessment
Recommendation 1: Include cardiovascular risk assessment to inform management options for patients with elevated BP.
Assess cardiovascular risk together with clinic BP readings to inform care decisions and to engage the patient in a discussion about the importance of managing elevated BP.
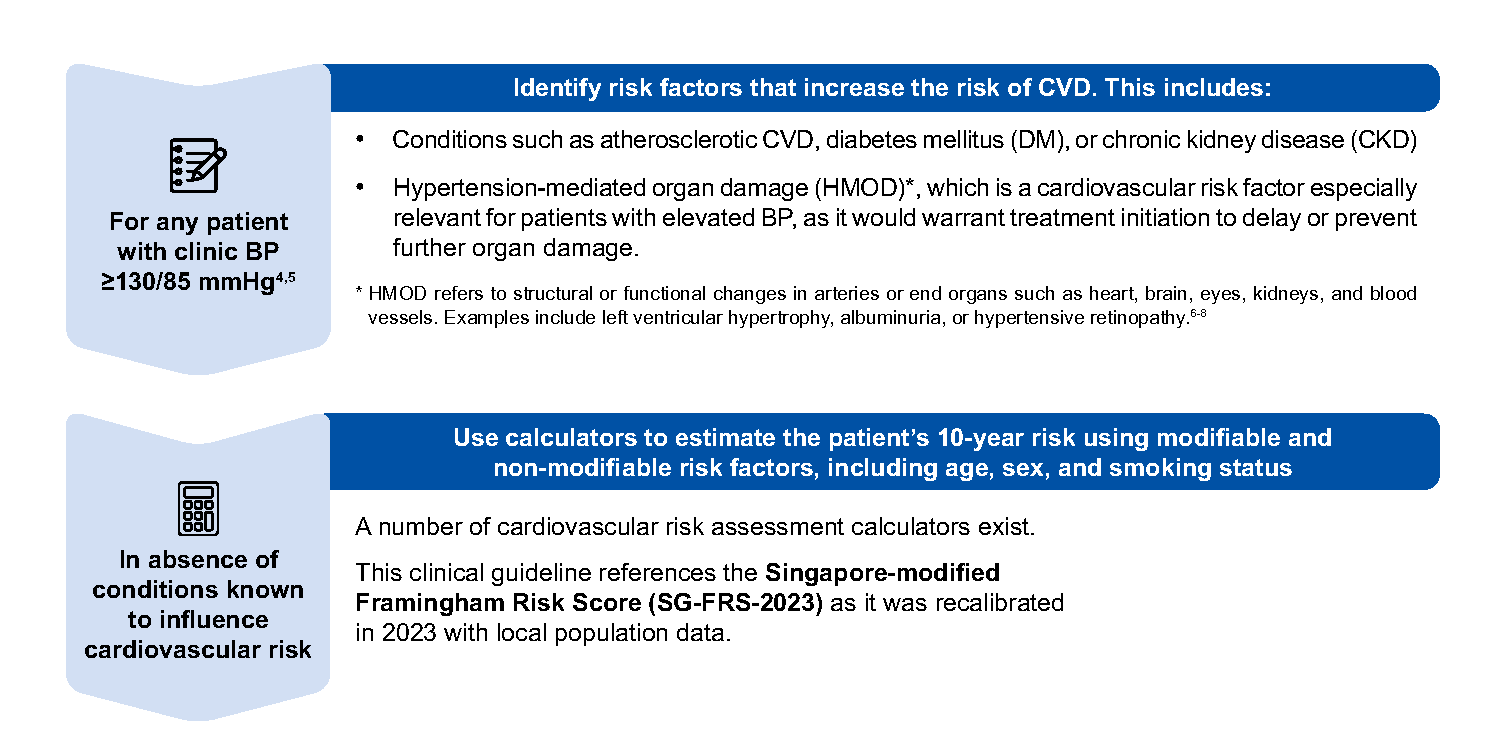
The SG-FRS-2023 is available here
Additional factors that should be considered to further inform overall assessment and guide individualised management include:
Other comorbidities not identified through cardiovascular assessment, such as asthma/COPD or gout
Patient-related factors and overall health status, including pregnancy, frailty, life expectancy, socioeconomic factors, as well as individual needs, values or preferences regarding management options
The use of clinic BP and cardiovascular risk assessment to inform pharmacotherapy options is discussed further below.
Notepad: Care for patients with comorbidities Management of hypertension is only one component of cardiovascular preventive care. Refer to the following ACGs for further details on relevant comorbidities: |
Notepad: Consider secondary causes of hypertension Secondary hypertension refers to hypertension due to an underlying, identifiable cause.9 Suspicion of secondary hypertension should be higher in certain circumstances, such as early-onset, severe, or resistant hypertension. A suggestive family history or clinical clues can point to a specific secondary cause of hypertension, which includes:
Management of secondary hypertension depends on the underlying cause and can require a combination of lifestyle intervention, cause-specific medications, and surgery. Referral for further investigations and shared management is often required. |
†Safe or moderate drinking is defined as no more than two standard drinks a day for men, and no more than one standard drink a day for women; a standard alcoholic drink contains 10 g of alcohol and roughly equates to one can (330 ml) of regular beer with 5% alcohol content, half a glass (100 ml) of wine with 15% alcohol content and one shot (30 ml) of spirits with 40% alcohol content.10
‡Local evidence on patients with hypertension reported a prevalence of around 5%.11
Management
The main goals of hypertension management are to achieve significant reduction in BP to attain optimal BP control, delay or prevent progression of hypertension and its associated complications, and mitigate CVD risks. BP levels can be effectively lowered through a tailored management plan, which includes personalised BP targets, sustainable lifestyle intervention, and pharmacotherapy where appropriate.
BP targets for patients with hypertension
Any reduction in BP decreases the risk of cardiovascular morbidity and mortality.12-15 The benefits of BP reduction are shown in Figure 1 below.
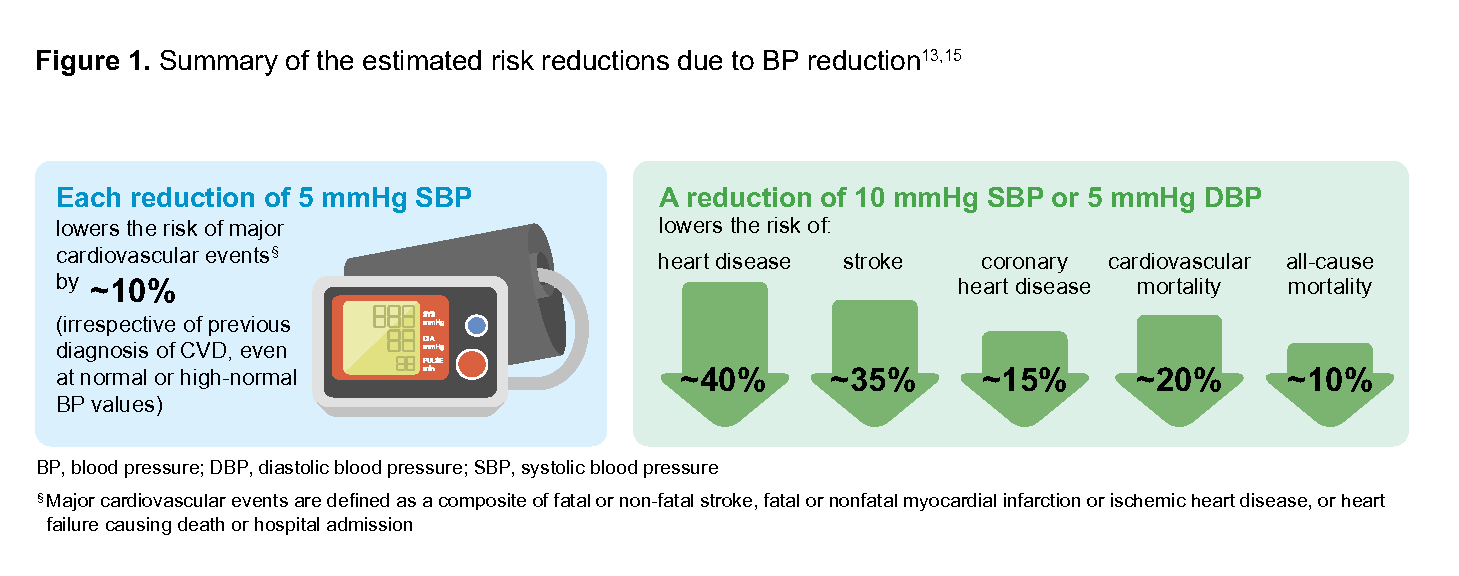
Figure 1.Summary of the estimated risk reductions due to BP reduction
Individualise BP targets according to patient cardiovascular risk and overall health status; more stringent BP targets can be considered as tolerated by the patient. Do not lower BP below 120/70 mmHg as evidence of benefit beyond this threshold is inconsistent, and the potential for increased risk of side effects can lead to treatment discontinuation.
Table 1. Guide to setting BP targets
Patient stratification based on comprehensive assessment | BP targets (clinic reading) |
|---|---|
High to very high cardiovascular risk
| <130/80 mmHg |
Low to intermediate cardiovascular risk
| <140/90 mmHg Consider going lower as tolerated (e.g., <130/80 mmHg) |
Older age (e.g., >80 years old), frail, orthostatic hypotension, or limited life expectancy | Consider less stringent BP targets (e.g., <150/90 mmHg) |
BP, blood pressure; CVD, cardiovascular disease; CKD, chronic kidney disease; DM, diabetes mellitus; HMOD, hypertension-mediated organ damage; SG-FRS-2023, Singapore-modified Framingham Risk Score 2023
Benefits of lifestyle intervention
For patients with elevated BP, lifestyle intervention includes healthy diet (e.g., reducing sodium intake and alcohol consumption), increased physical activity, weight reduction if overweight or obese, and smoking cessation.a Benefits of lifestyle intervention extend across age groups and cardiovascular risk levels, and are therefore encouraged for all patients.
A personalised approach taking into consideration factors such as comorbidities, patient’s preferences, quality of life, frailty, functionality, and cognitive status will help in setting sustainable lifestyle plans. 19,20
For examples of patient resources and programs, see High blood pressure: healthy eating guide, MOVEIT Programme. For patients with concomitant CKD, see ACG on CKD management, as advice relating to salt and protein intake can vary.
When to initiate pharmacotherapy
Pharmacotherapy complements lifestyle intervention where appropriate. The decision to initiate treatment with antihypertensive medications is guided by the patient’s BP, cardiovascular risk, and presence of conditions such as CVD, CKD, DM, or HMOD. Figure 2 below provides a general guide for when pharmacotherapy should be initiated.
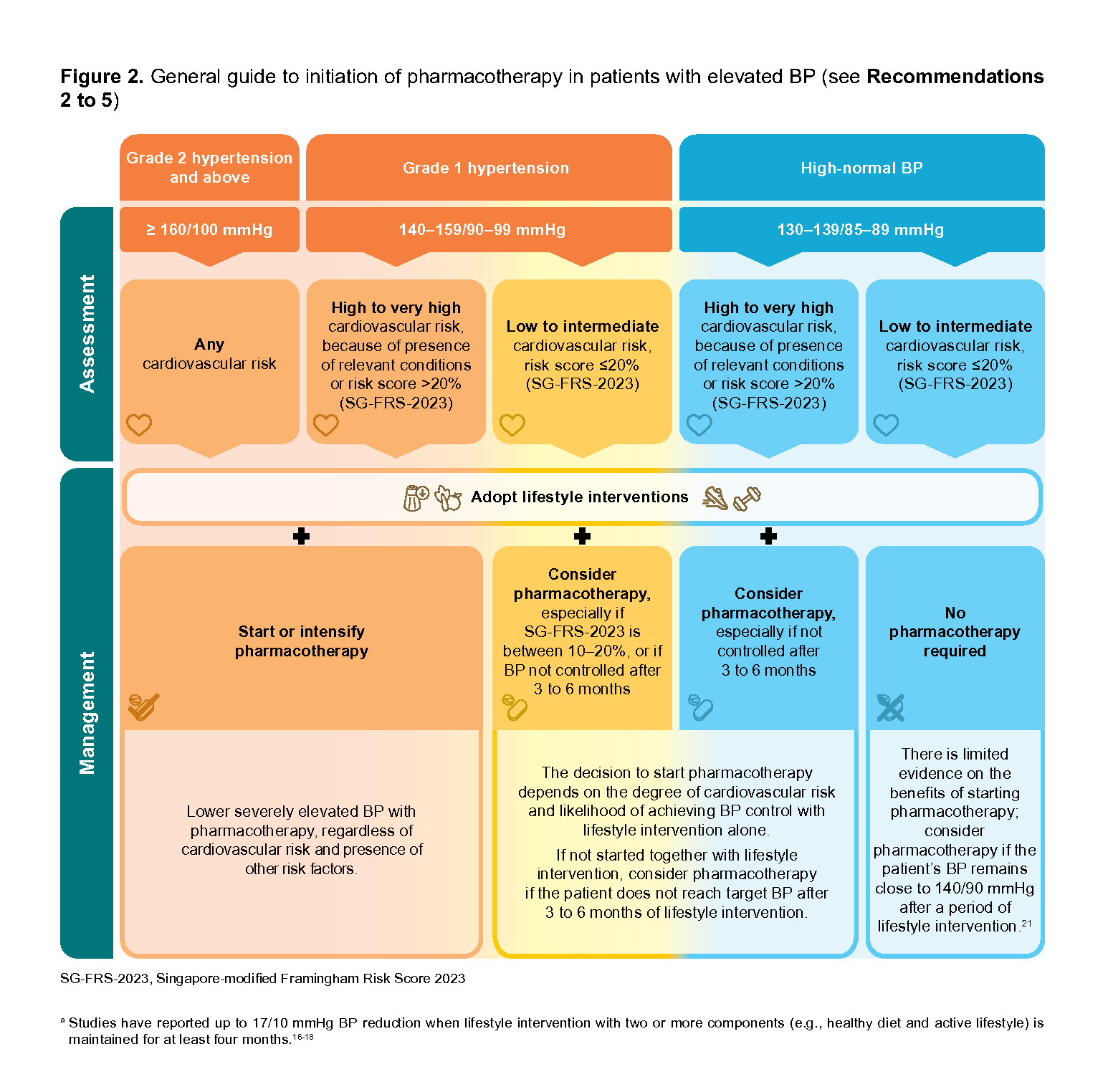
Figure 2.General guide to initiation of pharmacotherapy in patients with elevated BP (seeRecommendations2 to 5)
Choosing pharmacotherapy
Recommendation 2: Use an ACE inhibitor, ARB, or CCB as first-line antihypertensive medications; consider thiazide/thiazide-like diuretics as alternative first-line if indicated.
Where antihypertens medication is warranted, most patients would benefit from starting with a low-dose, regardless of whether it is monotherapy or dual therapy.
As monotherapy, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and thiazide/thiazide-like diuretics have comparable BP-lowering efficacy and are equally effective in preventing risk of fatal and non-fatal cardiovascular events.22-26
Thiazide/thiazide-like diuretics are considered as an alternative first-line as their side-effect profile is less favourable compared to the other first-line antihypertensives. Known side-effects include increased risk of insulin resistance and potential electrolyte derangement, especially for elderly patients.
Overall, the choice of antihypertensive(s) depends on a patient’s comorbidities, common side effects, monitoring parameters, and other practical considerations such as frequency of administration (see Table 2)
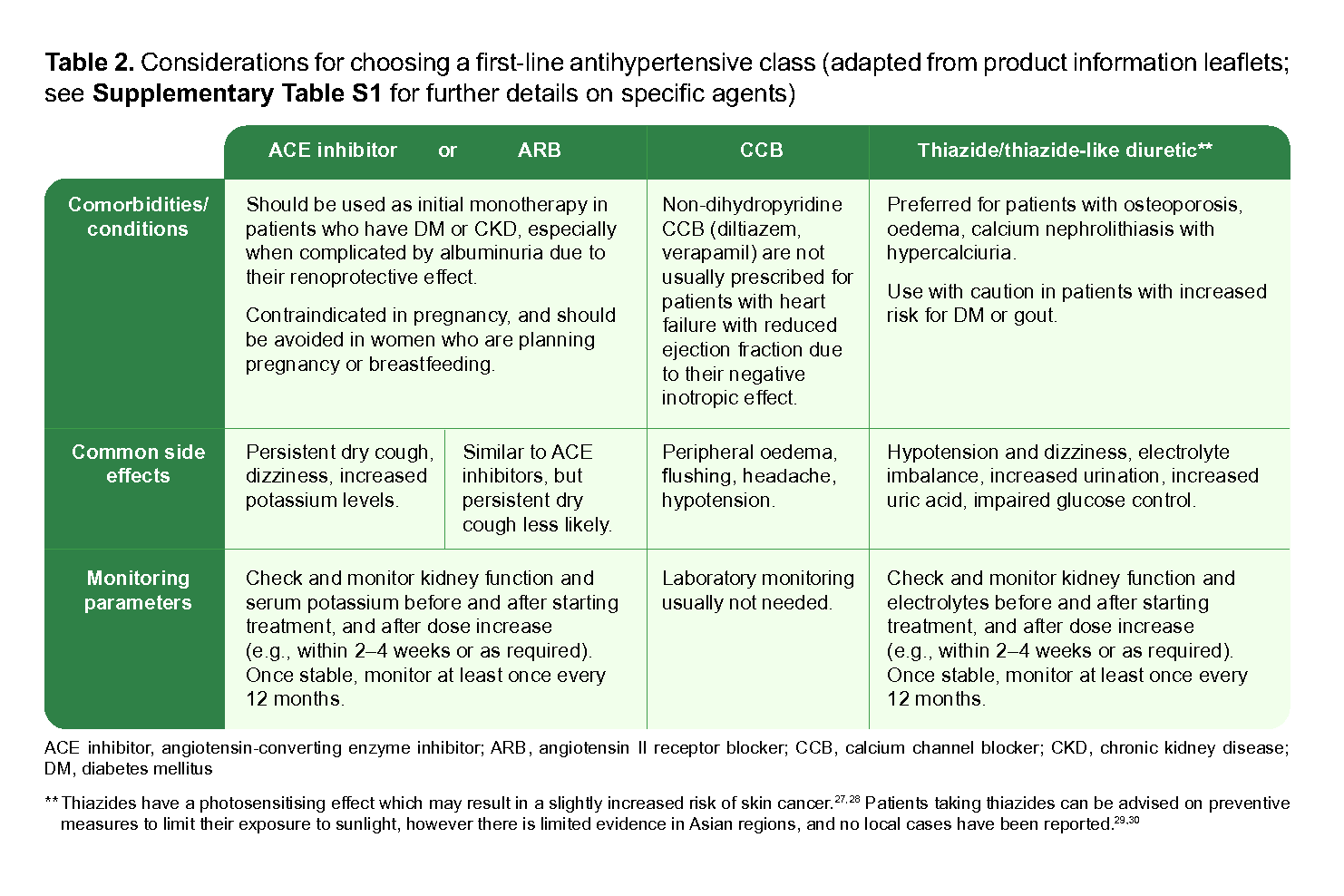
Table 2.Considerations for choosing a first-line antihypertensive class (adapted from product information leaflets;seeSupplementary Table S1 for further details on specific agents)
Recommendation 3: Avoid initiating beta blockers (BBs) as first-line monotherapy for BP control unless BB use is expected to have favourable effect on patient comorbidities.
While antihypertensive medication classes have similar BP-lowering effects, ACE inhibitors, ARBs, CCBs, and thiazides/thiazide-like diuretics are associated with better outcomes against stroke and all-cause mortality compared to BBs, especially in patients aged 60 years or older.26, 31-34
Because of this less favourable benefit/risk ratio, BBs are not preferred as first-line monotherapy for BP-lowering. However, they may be beneficial for patients who also require heart rate reduction, or have cardiac comorbidities such as stable ischaemic heart disease, chronic heart failure, or atrial fibrillation.26, 31, 32, 35
BB subclasses differ in their pharmacodynamic and pharmacokinetic properties due to differences in bioavailability and receptor selectivity (see Table 3)
Table 3. Prescribing considerations for cardioselective and non-selective beta blockers
Cardioselective (e.g., atenolol, bisoprolol, metoprolol and nebivolol) | Non-selective (e.g., propranolol and carvedilol) |
|
|
The choice of BB should be based on the patient’s clinical profile, side effect profile, and dosing frequency (see Supplementary Table S1).
Recommendation 4: Consider initiating low-dose dual therapy from two different antihypertensive medication classes based on required BP reduction and cardiovascular risk.
Compared to monotherapy, dual therapyc (treatment with two medicines from different antihypertensive classes) is associated with greater magnitude of BP-lowering and better safety profile.36-38 Therefore, starting with dual therapy may be appropriate if a greater reduction in BP is required to reach targets, such as for patients with SBP/DBP ≥20/10 mmHg above target, those with Grade 2 hypertension or higher (clinic BP ≥160/100 mmHg), or those with comorbidities such as DM or CKD who may require more intensive treatment.39-41
For elderly or frail patients, the benefits of dual therapy should be weighed against potential harms, such as increased risk of adverse effects, the impact of impaired organ function, or limited tolerability for medications. |
While the choice of medication class is largely informed by comorbidities (see Table 2) and other patient factors, evidence suggests the most effective combination for reducing cardiovascular, cerebrovascular, and adverse renal outcomes is:
ACE inhibitor/ARB + dihydropyridine CCB (such as amlodipine)42, or
ACE inhibitor/ARB + diuretic (preferably a thiazide-like diuretic)43,44
Certain combinations may need caution or avoidance due to associated risks (see Table 4 below).
Table 4. Common antihypertensive combinations to consider avoiding due to their associated risks
Combination of medication classes to consider avoiding | Risks when used in combination |
|---|---|
ACE inhibitor + ARB | Increased risk of hyperkalaemia, acute kidney injury and lower BP due to similar mechanisms of action |
BB + non-dihydropyridine CCB (e.g., verapamil) | Increased risk of bradycardia and/or atrioventricular block |
BB + diuretic | Increased risk of developing T2DM |
ACE inhibitor, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BB, beta blocker; BP, blood pressure; CCB, calcium channel blocker; T2DM, type 2 diabetes mellitus
Single-pill combinations may be used due to their practical benefits such as reaching BP targets, improved treatment adherence and persistence rates, and lower pill burden.45, 46 However, single-pill combinations may not be suitable for all patients, such as those who require individualised dose adjustment, or are at risk of adverse effects from medication interactions.
b‘ Low-dose’ is defined as ‘initial dose’ (see Supplementary Table S1).
cDual therapy at average to high doses is associated with adjusted mean SBP reductions of 20–25 mmHg and DBP reductions of 10–15 mmHg, while monotherapy at average doses achieved adjusted mean SBP reductions of 10–15 mmHg and DBP reduction of 8–10 mmHg.39
Recommendation 5: Intensify antihypertensive medications to optimise BP control if response to initial treatment is not achieved as expected (e.g., within three months).
Patients on pharmacotherapy who do not reach their BP target may require treatment intensification. After ruling out modifiable reasons for suboptimal response (see section ‘Considerations before intensification’ below), treatment could be intensified by increasing dosage of current medication, adding a different antihypertensive class, or switching to a different medication class.
Adding a different antihypertensive medication at low-dose is encouraged where possible, as this provides additive BP-lowering effects while minimising the risk of side effects (it is possible to achieve half of the maximal BP-lowering effect within a week of intensification and full effect within four weeks).47-49 Evidence on the optimal timeframe for intensification is limited, with one study suggesting that this could be set around three months after treatment initiation (if expected treatment response is suboptimal) to avoid increased risk of cardiovascular events or mortality.50
Considerations before intensification
Prior to advancing treatment intensity, review and discuss factors influencing medication adherence with the patient, including their ability to tolerate existing medications, side effects from increasing the dose, cost, and patient preferences. Other clinical and practical considerations include:
Evaluating salt intake
Investigating secondary hypertension (including medication-induced causes)
Managing volume overload (e.g., salt and water retention due to acute kidney injury)
Treating comorbidities
Notepad: Strategies to encourage and support adherence Including the patient in discussions about their management options is a key part of shared decision-making, enabling open conversations about individualised treatment goals and improving adherence to the overall plan. Discuss and agree with the patient on the approach to treating their hypertension, including lifestyle interventions, benefits and risks of starting pharmacotherapy in light of their overall cardiovascular risk, and medication choices. Encourage adherence by educating patients on how their antihypertensive medications work, and the expected time frame for improvements in BP reduction. Reinforce this information at each visit. For example, if a decision is made to initially prescribe two low-dose antihypertensives together, emphasise why it is important that both are taken consistently, i.e. to maximise BP control while reducing the risk of adverse effects (compared with high-dose monotherapy). Other strategies to support adherence include:
Patients can also take their antihypertensive medications at a time of day that is convenient for them, which optimises adherence and minimises undesirable effects.51 Night-time dosing may limit the perception of adverse effects. |
Considerations for specialist referral
Specialists can be consulted for advice, referral or collaborative care at any point, particularly for:
Patients with indications for emergency or urgent treatment, e.g., malignant hypertension, hypertensive cardiac failure or other impending complications
Patients with difficult-to-manage hypertension, e.g., unusually labile BP
Patients with hypertension with no or incomplete response to multiple medication regimes (three or more i.e. resistant hypertension)
Patients with suspected secondary hypertension, e.g., hypertension with hypokalaemia
Hypertension in certain patient populations, e.g., pregnant women, young children, patients aged less than 30 years
Patients with acute or recent cardiovascular complications from hypertension
Notepad: Resistant hypertension Resistant hypertension is defined as uncontrolled BP despite a patient taking ≥3 optimally-tolerated antihypertensives (including a diuretic). When suspecting resistant hypertension, check if:
Consider referral to a specialist or seek specialist advice after ruling out adherence issues. |
Monitoring and follow-up
Recommendation 6: Follow up all patients with hypertension at least every six months, with more frequent review as needed.
The frequency of follow-up visits should be tailored according to the patient’s clinical circumstances and progress in BP reduction. More frequent review (e.g., within three months) can be considered:
For patients at increased risk of hypertension-related complications, such as those with BP ≥160/100 mmHg, CKD, DM, HMOD, or high cardiovascular risk
If medication was recently initiated or optimised (dose adjustment, switching or adding-on of different antihypertensive class)49,50
If response to treatment is not as expected
Home BP monitoring should be encouraged where possible (see ‘Clinical utility and approach to home BP monitoring’ below). Monitor patients closely and adjust the management plan accordingly if complications or treatment-related adverse events arise. Continue reviewing cardiovascular risk factors and parameters where appropriate, including BP, lipids profile, weight, body mass index, cardiac and kidney assessment (such as estimated glomerular filtration rate and urinary albumin:creatinine ratio), kidney function, electrolytes (e.g., serum potassium), alcohol and smoking status.
Notepad: Clinical utility and approach to home BP monitoring When available, home BP monitoring is useful for:
|
Click here for resources on educating patients or caregivers on appropriate home BPmonitoring techniques
Notepad: A general reference for corresponding values of clinic and non-clinic BP readings BP readings taken in non-clinic settings tend to be lower than readings taken in clinic. The difference between clinic and non-clinic BP readings is not fixed, and decreases as clinic BP decreases. Table 5 should be interpreted with caution as the information reflects the average clinic and non-clinic BP values across untreated and treated individuals from non-Asian and Asian ethnicities. |
Table 5.Corresponding values of clinic versus non-clinic BP readings (mmHg).††
Clinic 24-hour | HBPM or Daytime ABPM | Night-time ABPM | ABPM |
|---|---|---|---|
120/80 | 120/80 | 100/65 | 115/75 |
130/80 | 130/80 | 110/95 | 125/75 |
140/90 | 135/85 | 120/70 | 130/80 |
160/100 | 145/90 | 140/85 | 145/90 |
ABPM, ambulatory blood pressure monitoring; HBPM, home blood pressure monitoring
††Adapted from Whelton et al. 201753
dWhite-coat hypertension: If clinic BP is consistently elevated despite the absence of obvious risk factors.
eMasked hypertension: If clinic BP is consistently normal but there are clinical features consistent with hypertension, e.g., signs of HMOD.
Click here for Table S1 and S2
Expert Group
Chairpersons
Clin Assoc Prof Tay Jam Chin, General Medicine (TTSH)
Dr Lee Biing Ming Simon, Family Medicine (NHGP)
Members
Dr Moy Wai Lun, General/Internal Medicine (SKH)
Dr Mondry Adrian, General/Internal Medicine (Kaizen Medical)
Clin Assoc Prof Lim Soo Teik, Cardiology (NHCS)
Dr Chai Ping, Cardiology (NUHCS)
Dr Low Lip Ping, Cardiology (Low Cardiology Clinic)
Dr Troy Puar Hai Kiat, Endocrinology (CGH)
Assoc Prof Chua Peng Wei Melvin, Geriatric Medicine (SKH)
Adj Assoc Prof Chua Horng Ruey, Nephrology (NUH)
Dr Sankaraprasad Anand Sankar, Family Medicine (NUP)
Dr Andrew Ang Teck Wee, Family Medicine (SHP)
Dr Leong Choon Kit, Family Medicine (Mission Medical Clinic, Class PCN)
Dr Ngoh Hui Lee Sharon, Family Medicine (AMK FM Clinic, Parkway-Shenton PCN)
Dr S Suraj Kumar, Family Medicine (Drs Bain & Partners)
Ms Wong Yee May, Cardiology Pharmacy (TTSH)
Mr Marvin Sim, Pharmacy (NUHSP)
Healthier SG cardiovascular risk calculator
Click here to access an online calculator to compute SG-FRS-2023 scores for the general population, originally developed as part of Healthier SG Care Protocols resource. The calculator additionally generates target levels for LDL cholesterol (and blood pressure) for patients at various levels of cardiovascular risk.
Additional resource for cardiovascular risk assessment using SG-FRS-2023 [PDF]
Feedback
Click here to give us feedback on this ACG
Related ACGs
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Hypertension – tailoring the management plan to optimise blood pressure control. ACE Clinical Guideline(ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-htn-management
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.