
Major depressive disorder – achieving and sustaining remission ACG
Last updated 19 May 2026
ACE Clinical Guidelines (ACG) provide concise, evidence-based recommendations to inform specific areas of clinical practice and serve as a common starting point nationally for clinical decision-making.
Overview
This ACE Clinical Guideline (ACG) highlights the non-pharmacological and pharmacological management of major depressive disorder (MDD) to achieve remission and reduce the risk of relapse. Specifically, the ACG offers evidence-based recommendations on holistic assessment of MDD severity and patient factors to guide management, treatment of an MDD episode, and maintenance treatment to reduce relapse risk. The ACG focuses on adults (patients 18 years old and above), though brief guideline on other patient groups (including perinatal women as well as children and adolescents) is included.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Evaluate MDD severity based on
Symptom profile,
Functional impairment, and
Risk of harm (to self or others).
Personalise the treatment approach based on MDD severity and other patient factors.
For patients with mild to moderate MDD, offer psychological treatment over antidepressants where feasible and acceptable.
For patients with moderately severe or severe MDD:
Offer a combination of a second-generation antidepressant with psychotherapy, or psychotherapy alone.
Consider a second-generation antidepressant when psychotherapy is not feasible or acceptable.
If response to initial treatment is suboptimal, assess possible reasons before adjusting management strategy.
Continue treatment after remission to reduce relapse risk; if antidepressants are prescribed, continue at optimal dose for at least 6 months after remission.
Refer to the Evidence-to-Recommendation (EtR) framework below for a summary of the factors underpinning the ACG’s recommendations.
Download the ACG and references in PDF
Major depressive disorder - achieving and sustaining remission
Major depressive disorder – achieving and sustaining remission references (Mar 2025) [PDF]
EtR Framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the major depressive disorder EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values.
Major depressive disorder – achieving and sustaining remission EtR framework (Mar 2025) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guidance (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Major depressive disorder (MDD) is highly debilitating. Patients experience a reduction in quality of life1 and ability to function,2 impacting interpersonal relationships, education, and employment.3-5 This may result in an overall substantial economic impact (due to demands on healthcare utilisation and reduced productivity).5, 6 The numerous detrimental effects of this mental health condition, including the increased likelihood of suicidal behaviour,7 underscore the need for effective treatments.
The 2023 National Mental Health and Well-being Strategy aims to enhance primary care capacity and capability for managing mental health conditions, which will facilitate anchoring care in community settings under a tiered care model.8 In support of the National Strategy, this ACE Clinical Guidance (ACG) aims to inform clinical management of MDD in primary and generalist care, among patients with a diagnosis of MDD. See Figure 1 for an overview of MDD management. Adults (patients 18 years old and above) are the focus of this ACG, though brief guidance on other populations is also included. Depression and anxiety are commonly comorbid9 – management of generalised anxiety disorder (GAD) is covered in another ACG
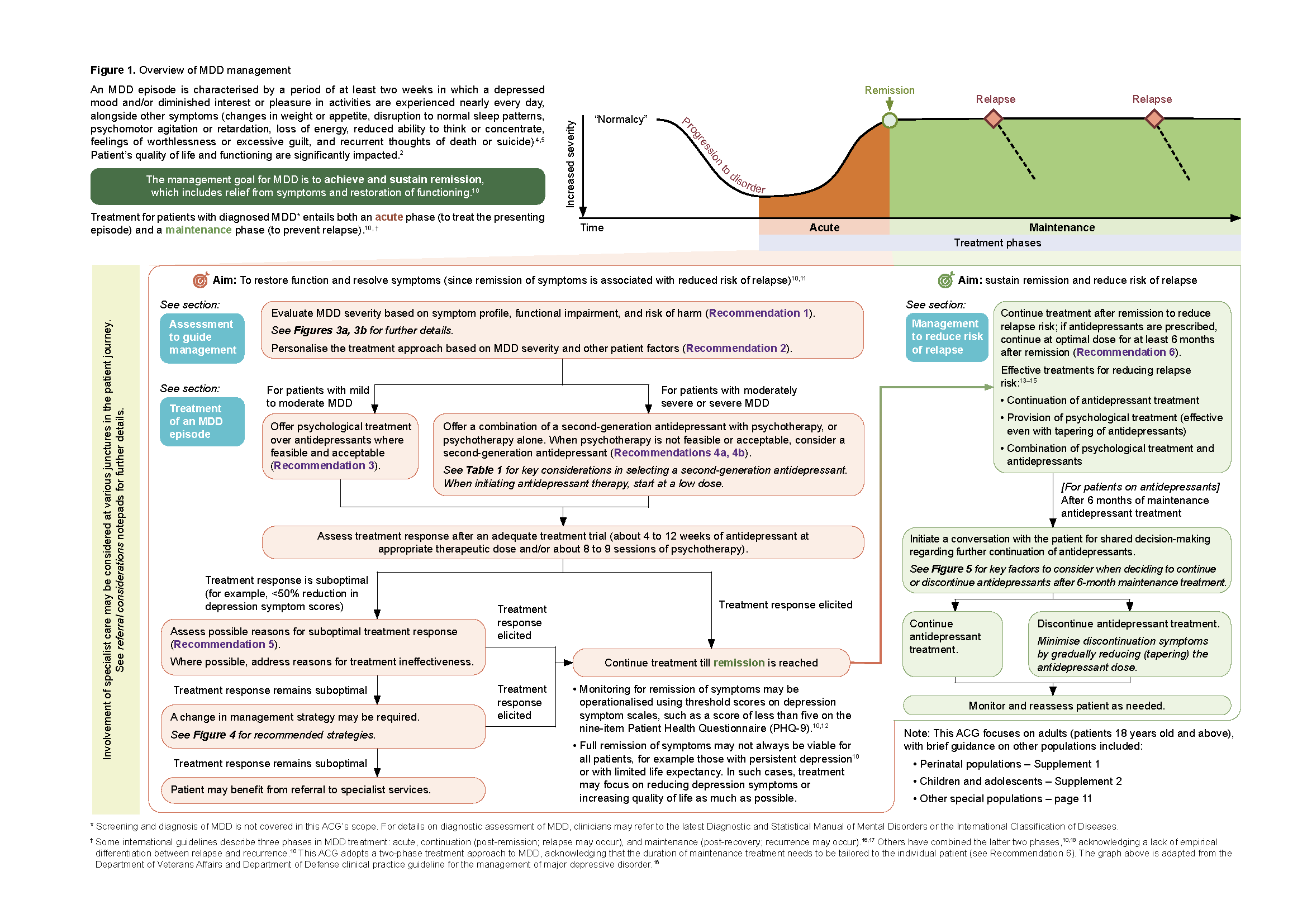
Figure 1. Overview of MDD management
Click here for larger version of the image
Assessment to guide management
Recommendation 1: Evaluate MDD severity based on; Symptom profile, Functional impairment, and Risk of harm (to self or others).
For patients who have been diagnosed with MDD, the first step is to determine the severity to inform management. 16,18
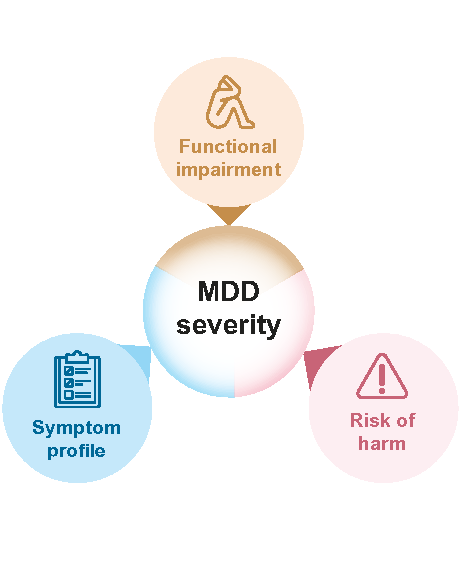
Assessing both a patient’s symptoms and extent of functional impairment provides a well-rounded view of the overall severity.4,5,10 As patients with MDD have a greatly increased vulnerability for suicide,7 incorporating risk of harm assessment is crucial (Figure 2). Figure 3a provides further details on each of these dimensions, and Figure 3b illustrates their interplay.
Locally, the PHQ-9 is commonly used to characterise the intensity of depression symptoms, which is a core dimension of the patient’s overall symptom profile.
Recommendation 2: Personalise the treatment approach based on MDD severity and other patient factors.
The assessed severity of the current MDD episode informs the intensity of treatment provided (see Recommendations 3 and 4). Other patient factors can also influence the overall treatment approach. These include:
Patient factors | Impact on treatment approach |
|---|---|
Patient preference | Patients may prefer either pharmacological or non-pharmacological treatment. Factor this in when selecting treatment, via shared decision-making. |
Physical illnesses and concurrent medication | Pharmacotherapy choice and dosing is influenced by patient’s comorbidities and current medication regime. For example, lower antidepressant doses may be required for patients with renal or hepatic impairment. When selecting an antidepressant, consider potential drug interactions with concurrent medications which may increase the side effect burden. Refer to package inserts or drug information references for further details. |
Social and environmental factors | Sources of stressors can be targeted as a complement to clinical treatment. For example, referral can be made to community resources or social services for patients experiencing domestic unrest or financial pressure. |
History of past episodes and treatment | Treatments that worked previously can be restarted.19 |
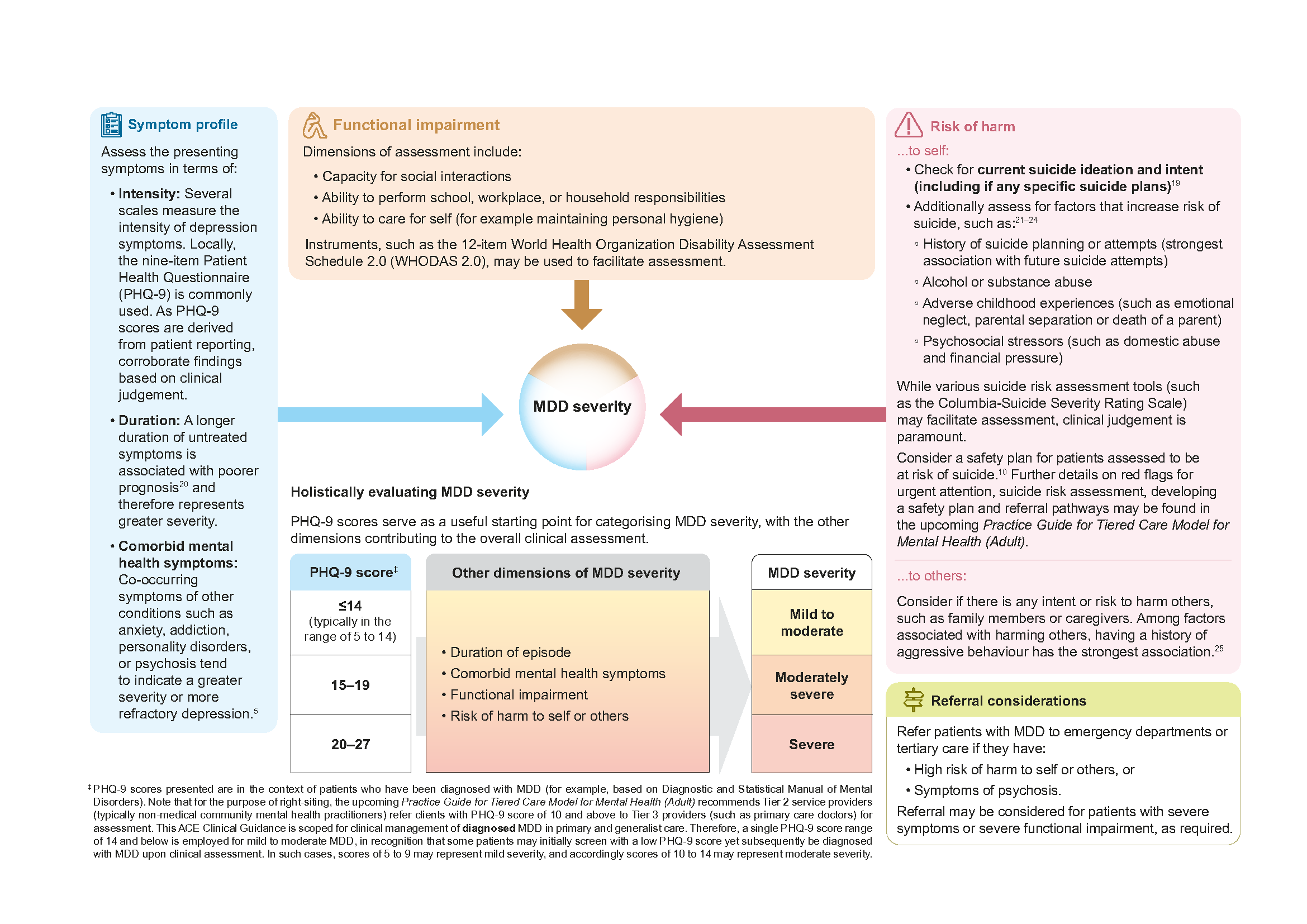
Figure 3a. Evaluation of MDD severity (to inform management) is based on symptom profile, functional impairment, and risk of harm (to self or others)
Click here for larger version of the image
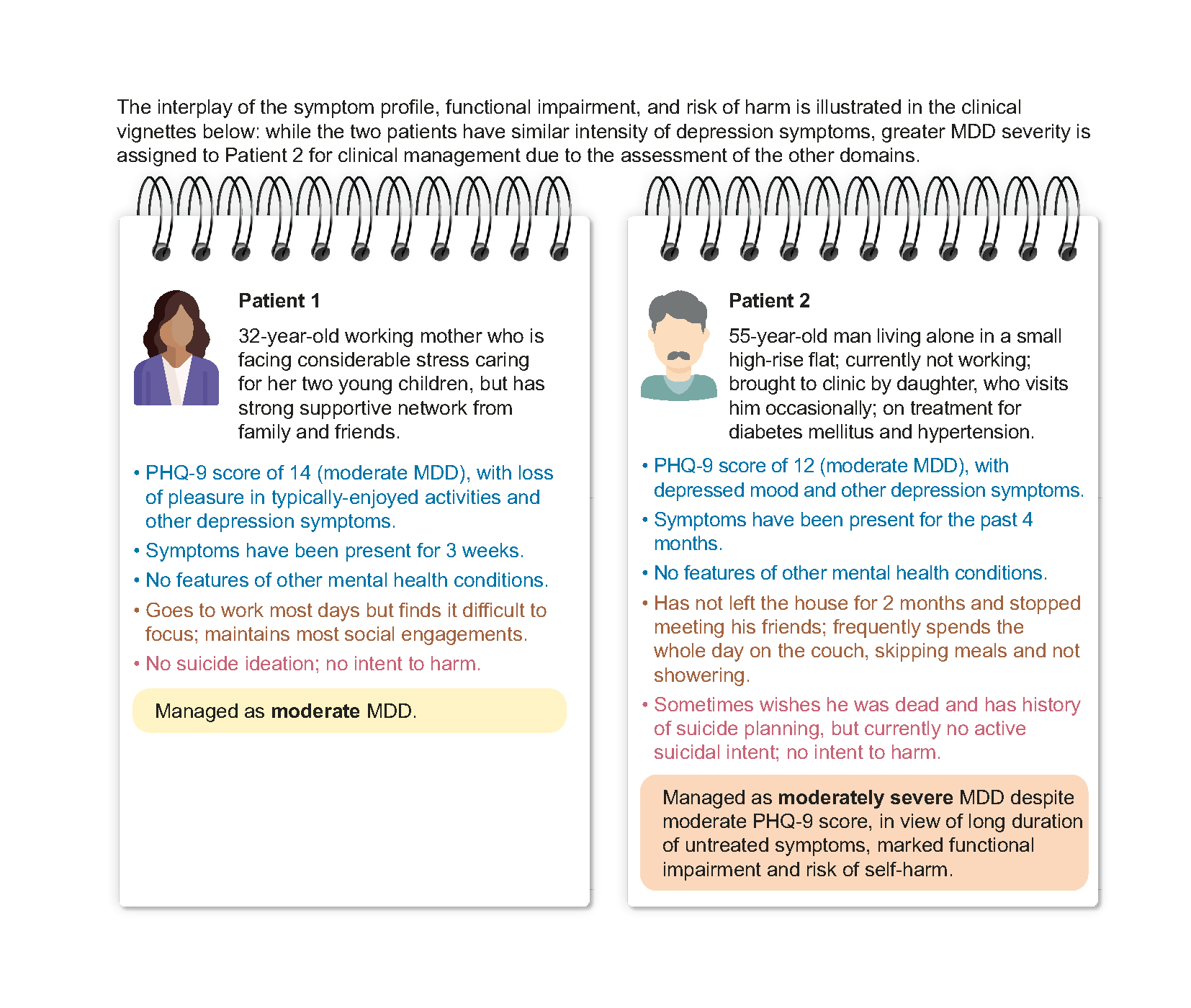
Figure 3b. Clinical vignettes illustrating holistic assessment of MDD severity (based on symptom profile, functional impairment, and risk of harm)
Treatment of an MDD episode
Evidence of efficacy and benefit-risk profile of treatments
The mainstay treatment options for MDD in primary care are antidepressants, psychological treatment (supportive counselling or psychotherapy), a and a combination of both. Network meta-analyses of randomised controlled trials (RCTs) have found that combining antidepressants with psychotherapy results in increased response26 and remission27 rates for depression, compared to antidepressants or psychotherapy alone. Overall, a combined treatment approach is most effective for patients with MDD, although the evidence base is more established for moderately severe and severe depression than for mild to moderate depression.27
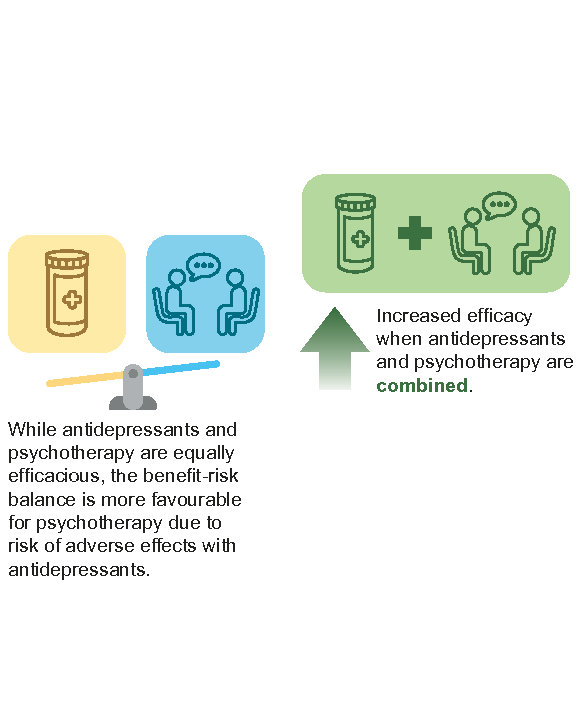
Antidepressant treatment and psychotherapy are equally effective in achieving remission.27-29 There is emerging evidence that psychotherapy may be more effective in the long term, although further research is required.26,27 Given that antidepressants and psychotherapy are equally efficacious, and considering the risk of adverse effects with antidepressant use,18,28 the overall benefit-risk balance is more favourable for psychotherapy.
Recommendation 3: For patients with mild to moderate MDD, offer psychological treatment over antidepressants where feasible and acceptable.
Preferred treatment of mild to moderate MDD
Psychological treatments (supportive counselling or psychotherapy) are preferred over antidepressants for mild to moderate MDD. Supportive counselling has proven to reduce depression symptoms, although it may be less efficacious than psychotherapy.30
In circumstances where these are not acceptable to the patient or not feasible, antidepressants may be required.
For example:
The healthcare professional assesses a need for, or the patient prefers, initiating treatment sooner (than waiting time allows)
The healthcare professional assesses that some symptomatic improvement is required before the patient can adequately engage in psychological treatment
The patient is unwilling to engage in psychological treatment
The patient is unable to attend or commit to regular therapy sessions
The patient is unable to participate in or understand tasks for therapy sessions (for example, due to cognitive impairment)
As MDD severity is dynamic, antidepressants can be started pre-emptively to supplement psychological treatment if clinical assessment indicates that the patient’s symptoms may worsen soon.
If referring to another healthcare professional for counselling or psychotherapy, provide information on MDD severity and other patient factors evaluated (Recommendations 1 and 2). Selection and delivery of an evidence-based psychotherapy is tailored to the patient’s therapeutic needs and preferences (see notepad Selecting and delivering psychotherapy for MDD on the next page for more information on evidence-based psychotherapies and delivery formats).
a In this ACG, psychological treatment is used as an umbrella term to include both psychotherapy and supportive counselling. Psychotherapies are structured upon specific objectives (for example, cognitive behavioural therapy guides patients in identifying the impact of their thought patterns and actions on their emotions and behaviours). Supportive counselling tends to be more unstructured, focusing on listening skills and developing a robust therapeutic alliance with the patient.16
Notepad: Selecting and delivering psychotherapy for MDD: | |
Choice of psychotherapy Various psychotherapies have proven efficacy in RCTs, with no significant differences between them. These include:31-33
| Delivery formats Various formats of administering psychotherapy have been found to be equally efficacious, including:34
Guided internet-delivered therapy is an emerging treatment format for MDD: psychotherapy materials are provided for the patient to work through, with guidance from a trained professional.16 Current evidence indicates that this treatment format is effective for treating depression, although treatment dropout may be higher compared to the other delivery formats. Unguided internet-delivered therapy has not proven efficacious for treatment of depression.34 |
Recommendation 4: For patients with moderately severe or severe MDD; a) Offer a combination of a second-generation antidepressant with psychotherapy, or psychotherapy alone; b) Consider a second-generation antidepressant when psychotherapy is not feasible or acceptable.
Preferred treatment of moderately severe and severe MDD
Combining a second-generation antidepressant with psychotherapy, or psychotherapy alone, are preferred for treating moderately severe and severe MDD, given greater efficacy and more favourable benefit-risk balance respectively (Recommendation 4a). Nonetheless, similar to mild to moderate MDD, some patients may be unwilling or unable to engage in psychotherapy. In these cases, treatment with a second-generation antidepressant on its own is an accepted alternative (Recommendation 4b). Co-management or referral to a specialist may be required, especially for severe MDD, depending on the healthcare professional’s experience.
Notepad: First and second-generation antidepressants First-generation antidepressants refer to tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs), while second-generation antidepressants include selective serotonin reuptake inhibitors (SSRIs), serotonin–norepinephrine reuptake inhibitors (SNRIs), and other newer agents. Second-generation antidepressants are recommended as the first-line antidepressants for treatment of MDD.16,18,19 First-generation antidepressants are not preferred for routine use16,18,19 due to their low therapeutic index (i.e. small margin between effective and toxic doses), which results in a greater likelihood of toxicity;16,35,36 and, potentially serious adverse events (for example, seizures, arrhythmias, and coma).16,37 Nonetheless, first-generation antidepressants could be reserved as an option on a case-by-case basis for selected patients with recurrent MDD who had previously responded to, and safely tolerated, them. |
Prescribing antidepressants for MDD
Refer to Table 1 for key considerations to guide selection of an antidepressant for MDD treatment. Table 1 provides a list of all locally-registered second-generation antidepressants with proven efficacy over placebo in achieving remission, with some variation in efficacy and tolerability (though these differences are mostly statistically insignificant).38 Antidepressants are associated with different adverse effects, contraindications, drug interactions, and costs, which reinforces the importance of shared decision-making with the patient when selecting pharmacotherapy.
Routine use of pharmacogenomic tests to select the choice and dose of antidepressants for newly-diagnosed patients with MDD is not currently recommended due to the inconsistent and low-certainty evidence, biased by lack of blinding.10, 39
When initiating antidepressant therapy, start at a low dose to reduce the risk of adverse effects and facilitate adherence.17 During the initial months of treatment and dose changes, monitor patients closely for emergent suicidal thoughts and behaviour, especially those under 25 years of age or with pre-existing suicide risk.40 Advise patients to seek medical attention immediately if symptoms emerge.
Among patients with depression, observational data suggests that the risk of suicidal behaviour and self-harm may be highest during the initial one to three months after starting an antidepressant and one month after stopping an antidepressant.41 Closer monitoring during these periods is therefore warranted.
Patient communication points at new onset of MDD Discussion regarding MDD and its treatment includes the following key points:
|
§ Some international guidelines prefer the term ‘withdrawal symptoms’, as this reflects the potential for physical dependence to develop when antidepressants are taken for weeks to months. This ACG uses ‘discontinuation symptoms’, acknowledging its familiarity to clinicians in the local context.
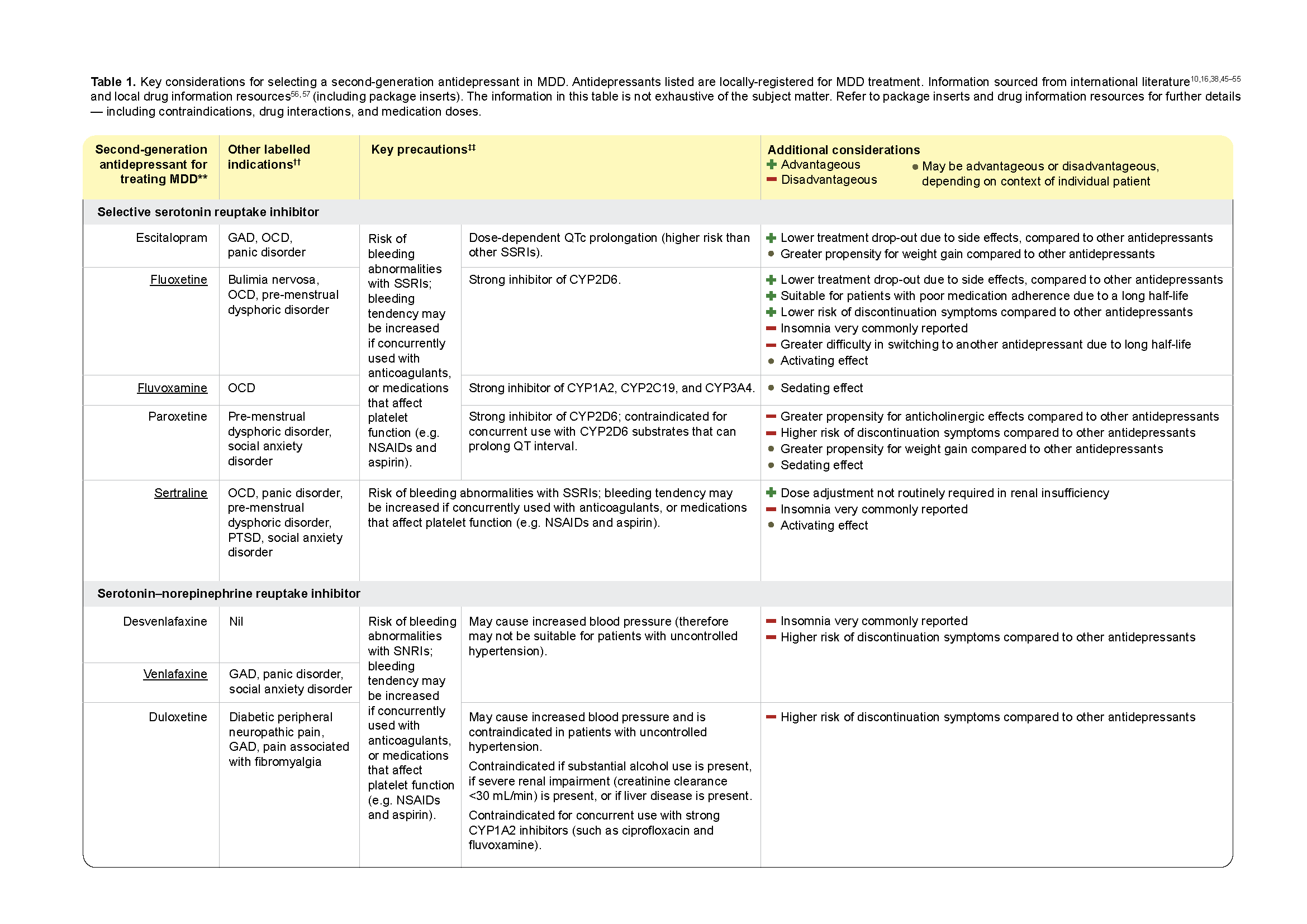
Table 1. Key considerations for selecting a second-generation antidepressant in MDD. (Part 1)
Click here for larger version of the image
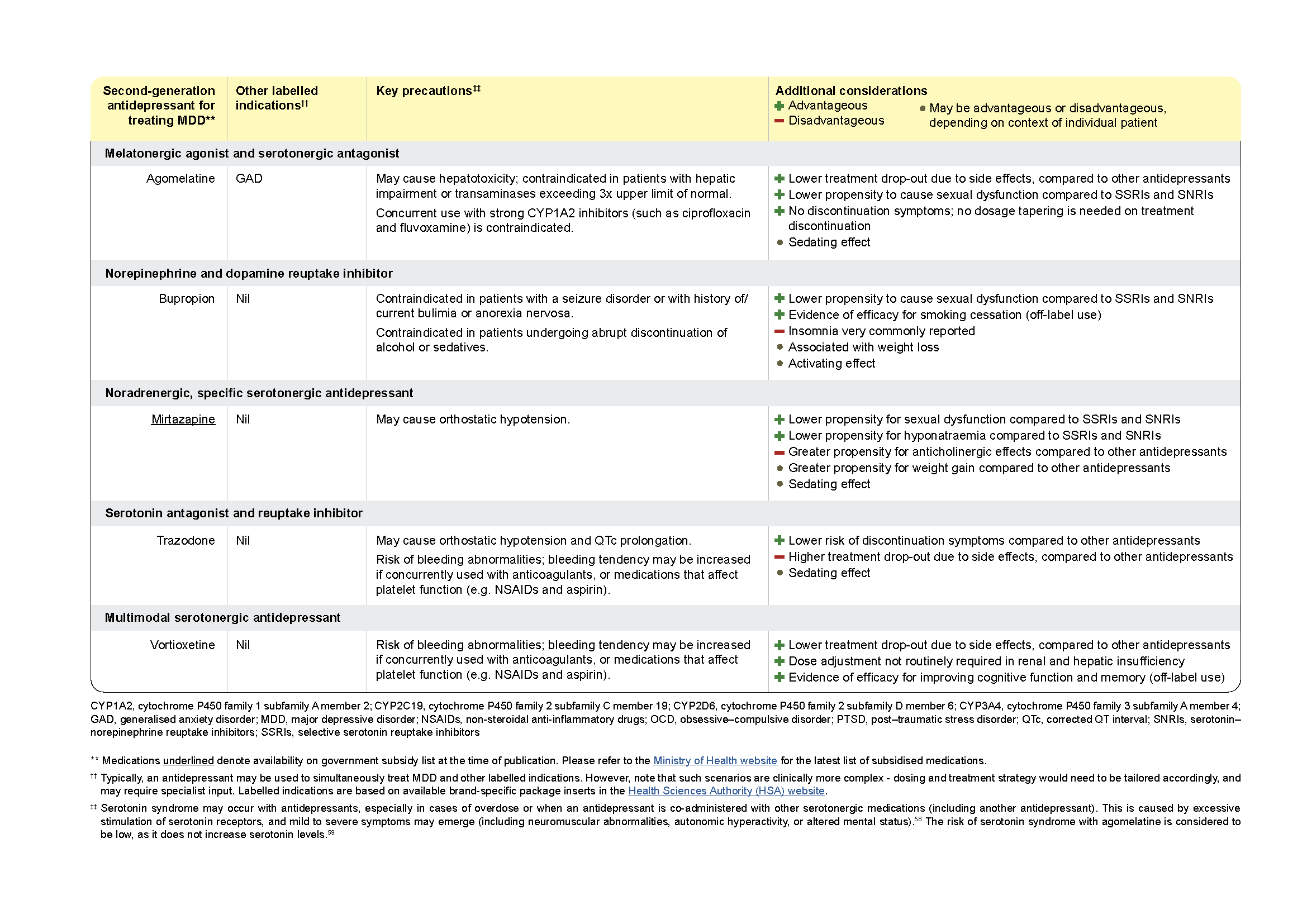
Table 1. Key considerations for selecting a second-generation antidepressant in MDD. (Part 2).
Click here for a larger version of this image
Management considerations for special populations |
|---|
Older adults (65 years old and above) Psychotherapy remains an effective treatment of depression for older adults.60 The efficacy of antidepressants among this population is less established,61 especially SSRIs.62 Therefore, where acceptable to the patient (i.e. receptive and able to engage in therapy) and feasible, psychotherapy is preferred for older patients with MDD. If prescribing an antidepressant, lower doses and more gradual titration may be required due to physiological changes that accompany advancing age. Note that antidepressants (especially SSRIs and SNRIs) have been associated with hyponatraemia, although such events are overall not very common.54 Consider also the potential for drug-drug interactions, as elderly patients may already be prescribed other medications for comorbid conditions. |
Patients with comorbid dementia The magnitude of depression symptom reduction with psychotherapy may be small for patients with dementia,63 although other non-pharmacological interventions have been found to reduce depression symptoms among this population.64 Efficacy of antidepressants for treating depression in this cohort is not established.65,66 |
Patients with comorbid anxiety symptoms Comorbidity with anxiety symptoms is associated with reduced likelihood of remission in MDD,67,68 and thus represents a higher severity of illness. More extensive interventions may therefore be warranted (for example, combination of an antidepressant with psychotherapy). Evidence of antidepressant anxiolytic effects in MDD is limited but indicate that antidepressants (including SSRIs,69 SNRIs, 70,71 bupropion,69 and vortioxetine72) reduce anxiety symptoms in MDD. No significant differences between agents have been reported.69,71 Overall, the presence of comorbid anxiety symptoms does not influence selection of antidepressant for MDD.10 However, if patients are diagnosed with generalised anxiety disorder (GAD), note that SSRIs or SNRIs are preferred: please refer to the GAD ACG for further details. |
Patients with neurodevelopmental disorders (for example, intellectual disability, autism spectrum disorder, or attention-deficit/ hyperactivity disorder) Patients with neurodevelopmental disorders may have atypical presentation of depression. Involve specialist care in assessment and treatment planning, as needed. Interventions should be adapted to the person’s needs (for example, developmental level and communication skills). |
Patient communication points on other treatments for MDD In addition to antidepressants and psychological treatment, various other treatments exist for MDD: |
|---|
Exercise Encourage exercise as a complement to pharmacotherapy or psychological treatment for all patients with MDD, as even simple activities like walking and jogging have been found to reduce depression symptoms.73 |
St John’s Wort Evidence suggests St. John’s Wort reduces depression symptoms. However, different extract preparations were employed in RCTs,74 limiting recommendations for St John’s Wort in international guidelines.17–19 Caution patients that St. John’s Wort may interact adversely with other medications, and emphasise that it should not be taken alongside antidepressants due to the risk of serotonin syndrome.75 |
Acupuncture While recent systematic reviews have found a positive effect of acupuncture on depression symptoms, the quality of the underlying evidence remains insufficient (for example, due to risk of bias concerns in RCTs).76,77 For patients interested in receiving acupuncture for treating MDD, advise them not to discontinue mainstay treatment (antidepressant and/or psychological treatment) |
Social prescribing of community-based programmes Emerging evidence suggests that community interventions such as music therapy, art therapy, exercise programmes, and community gardening may help reduce depression symptoms. However, more research is needed to better understand their effectiveness.78–80 For patients interested in joining community-based programmes, advise that they may be used as a complement to mainstay treatment (antidepressant and/or psychological treatment). |
Management of suboptimal response to initial treatment
Recommendation 5: If response to initial treatment is suboptimal, assess possible reasons before adjusting management strategy.
Some improvement in symptoms may occur as early as 2 weeks after starting antidepressant treatment, although the full benefit is typically observed between 4 to 12 weeks, with adequate dosing.42,43 Periodically monitor treatment progress in terms of symptom reduction (for example, via PHQ-9) and adverse effects of medications. Use this information to guide treatment decisions (for example, if dose or choice of antidepressant needs to be changed), as such measurement-based care enhances treatment adherence and remission rates.81 Note that high antidepressant doses may not be required to elicit a treatment response. For example, the balance between SSRIs’ efficacy and acceptability tends to be optimal at lower doses (fluoxetine: between 20 mg and 40 mg per day; escitalopram: between 10 mg and 20 mg per day; paroxetine: between 20 mg and 30 mg per day; sertraline: between 50 mg and 100 mg per day;82 fluvoxamine: evidence on optimal dose is less established due to greater imprecision, but a recent systematic review suggests that its efficacy may not be increased with doses above 150 mg per day).83
Suboptimal response may also be observed with psychological treatment. As evidence suggests that improvement in depression symptoms may be most rapid within the first 8 to 9 sessions of psychotherapy,84 a lack of improvement during this period may indicate the therapy is ineffective.
If treatment response remains suboptimal - for example, less than 50% reduction in depression symptom scores -after an adequate treatment trial (about 4 to 12 weeks of antidepressant at appropriate therapeutic dose and/ or about 8 to 9 sessions of psychotherapy), assess possible reasons for this.16 Reasons may include:16, 18, 19, 85
Ongoing psychosocial stressors and poor coping mechanisms
For example, financial pressure, interpersonal conflicts, or recent diagnosis of a severe medical condition.
Suboptimal treatment adherence
Routinely check compliance to treatment: patients may independently stop taking medication or reduce the dose in response to adverse effects or if they perceive treatment is ineffective.
Diagnostic inaccuracy or presence of other mental health conditions
For example, missed diagnosis of bipolar or psychotic depression, addictive disorder, or personality disorder. Note that the emergence of manic or hypomanic symptoms during antidepressant treatment may indicate the presence of bipolar depression.5
Comorbid conditions that may limit response to treatment or mimic depression symptoms such as fatigue
For example, anaemia, hypothyroidism, poor glycaemic regulation, or antidepressant-induced hyponatraemia.
If response remains suboptimal after assessing, and where possible, addressing reasons for treatment ineffectiveness, a change in management strategy may be required (please refer to Figure 4 for recommended strategies).
Referral considerations Specialist involvement may be required for assessing and addressing reasons for initial treatment ineffectiveness (for example, to detect and treat comorbid psychosis). If the second treatment attempt (Figure 4) still produces suboptimal response, patients may benefit from referral to specialist services. |
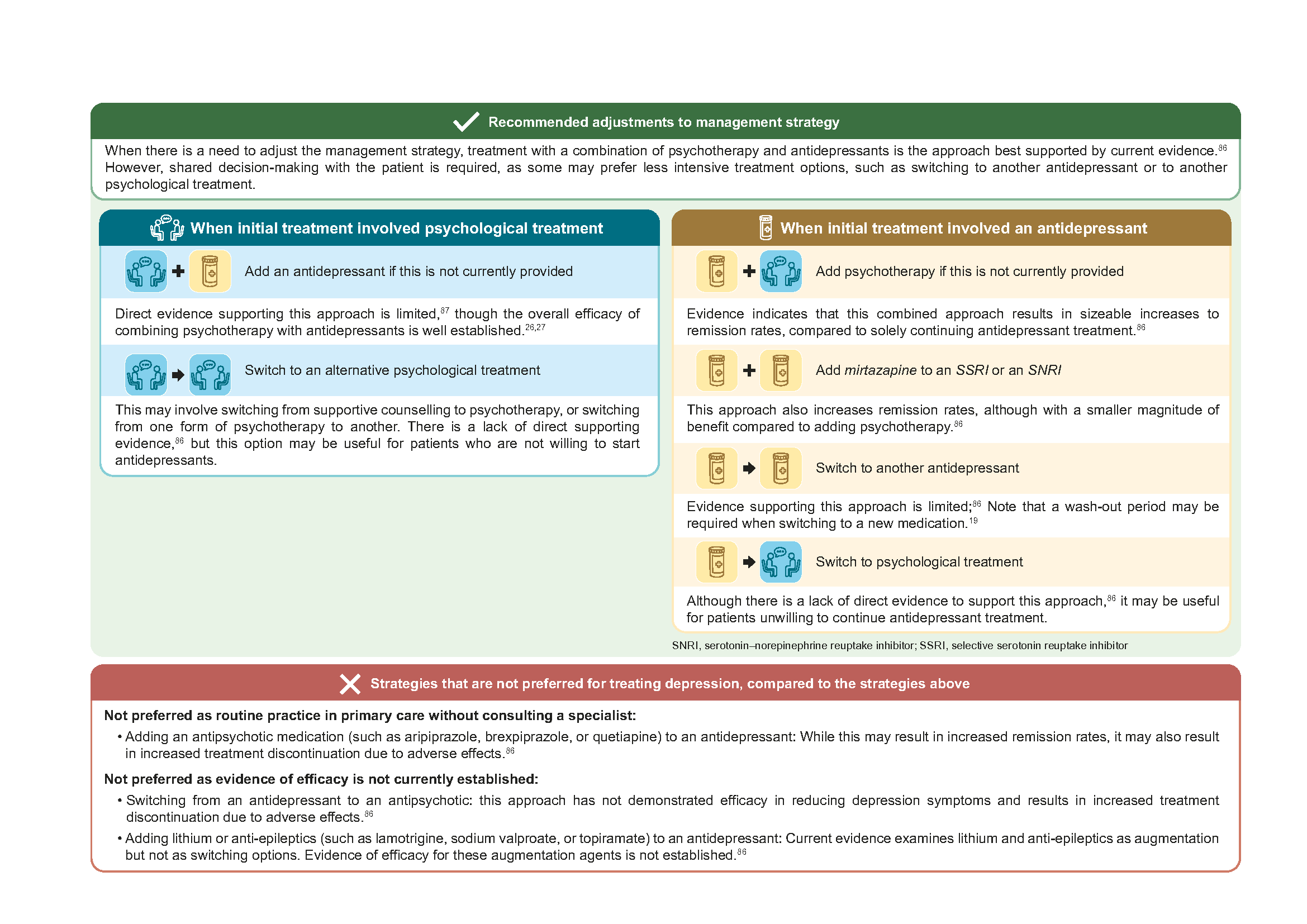
Figure 4. Changes in management strategy when initial response in suboptimal
Management to reduce risk of relapse
Recommendation 6: Continue treatment after remission to reduce relapse risk; if antidepressants are prescribed, continue at optimal dose for at least 6 months after remission
After remission from the acute MDD episode, patients who receive no treatment are at higher risk of relapse compared to those who do.13,14 Therefore, it is important to provide maintenance treatment post-remission. Current evidence indicates that the following treatments are effective in reducing relapse risk:13–15
Continuation of antidepressant treatment.
Provision of psychological treatment (effective even with tapering of antidepressants). Tailor the duration of psychological treatment based on individual patient’s needs.
Combination of psychological treatment and antidepressants.
Continuation of antidepressants for at least 6 months after remission is recommended because relapse occurs most frequently during this time.14 Maintain the same dose that achieved remission in the acute phase (optimal dose),16,19 unless there are reasons to adjust it (for example, due to adverse effects).19 After 6 months, initiate a conversation with the patient for shared decision-making regarding further continuation of antidepressants. Consider the following key factors (Figure 5) when making a shared decision with the patient.
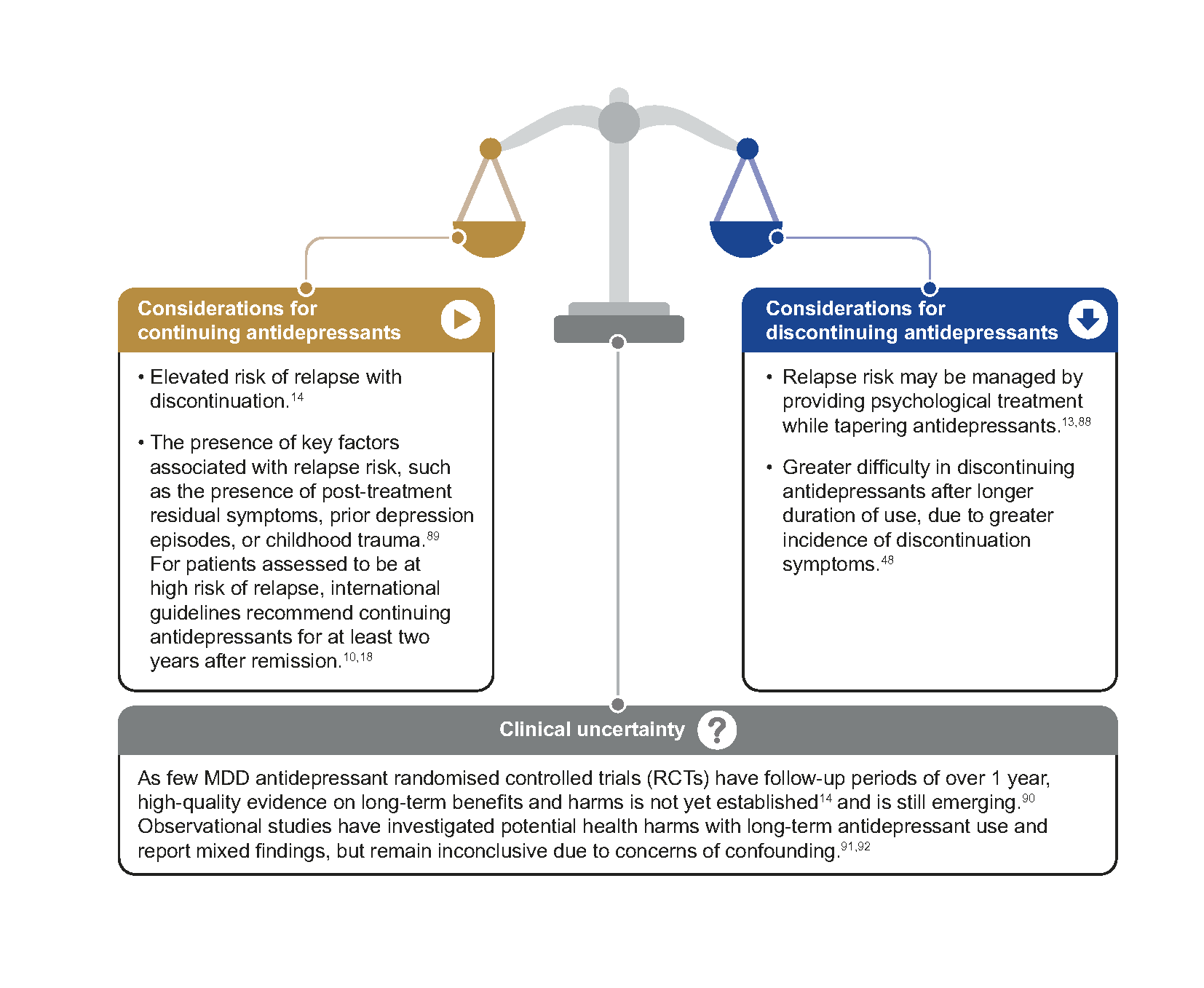
Figure 5. Key considerations for continuing or discontinuing antidepressants after 6-month maintenance treatment
If a decision is made to discontinue antidepressant treatment, minimise discontinuation symptoms by gradually reducing (tapering) the antidepressant dose.17 Longer duration of antidepressant use is associated with greater incidence of discontinuation symptoms. Hence, slower tapering may be required.48 Antidepressants with a short half-life also need to be tapered more slowly.19
Among patients with depression, observational data suggests that the risk of suicidal behaviour and self-harm may be highest during the initial one to three months after starting an antidepressant and one month after stopping an antidepressant.41 Closer monitoring during these periods is therefore warranted.
Patient communication points after remission
|
Supplementary materials
Supplement 1. MDD management considerations for perinatal populations
Supplement 2. MDD management considerations for children and adolescents
Expert group
Chairpersons
Dr Koot David, Family Medicine (SHP)
Adj Asst Prof Mok Yee Ming, Psychiatry (IMH)
Members
Dr Paul Ang Teng Soon, Family Medicine (Zenith Medical Clinic)
Dr Evelyn Boon, Psychology (SGH)
Dr James Cheong, Family Medicine (C3 Family Clinic)
Dr Goh Tze Chien Kelvin, Family Medicine (United PCN Clinical Lead)
Dr Guo Xiaoxuan, Family Medicine (SHP)
Ms Jiang Lina, Nursing (CGH)
Ms Amy Leo Wen Ling, Pharmacy (IMH)
Ms Lin Yijun Carol, Psychology (NHGP)
Mr Jeffrey Loh, Nursing (AH)
Dr Shaikh Abdul Matin Mattar, Internal Medicine (SGH)
Dr Ng Beng Yeong, Psychiatry (Mt Elizabeth Hospital)
Mr Ng Boon Tat, Pharmacy (IMH)
Dr Ng Mae Ling, Family Medicine (NUP)
Dr Winnie Soon, Family Medicine (NHGP)
Dr Wong Mei Yin, Psychology (Singapore Psychological Society)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Generalised anxiety disorder – easing burden and enabling remission
National Mental Health and Well-being Strategy (2023)
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Major depressive disorder – achieving and sustaining remission. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2025. Available from: go.gov.sg/acg-mdd
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties