
Initiating basal insulin in type 2 diabetes mellitus ACG
Last updated 21 May 2026
Published on 20 Nov 2017
Last Updated on 29 Nov 2024
Overview
This ACE Clinical Guideline (ACG) highlights the importance of not delaying insulin therapy for patients with type 2 diabetes mellitus and offers a practical guide on initiating basal insulin. It also provides evidence-based practice points on how to prevent and manage hypoglycaemia. First published in 2017, this ACG been updated in 2024 to reflect recent changes in insulin product availability and incorporate the latest evidence where relevant.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Start basal insulin if glycaemic targets are not met despite optimal treatment with non-insulin T2DM medications.
Review concomitant T2DM medications when starting basal insulin and continue them at the current or lower dose where appropriate.
Educate patients and their caregivers on how to use insulin safely and effectively, including how to prevent and manage hypoglycaemia.
Download the ACG and references
Initiating basal insulin in type 2 diabetes mellitus (Nov 2024) [PDF]
Initiating basal insulin in type 2 diabetes mellitus references (Nov 2024) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Approximately 1 in 4 Singaporeans with diabetes mellitus have poor glycaemic control, hence are at increased risk of diabetes-related complications and poor clinical outcomes.1-4 For patients with type 2 diabetes mellitus (T2DM), non-insulin T2DM medications can help patients to achieve initial glycaemic control but may not be able to do so in the long term. Patients with T2DM who are unable to reach their glycaemic targets despite optimal treatment with non-insulin T2DM medications alone should be started on insulin therapy.5
Patient education and shared decision making is integral to the successful initiation of insulin for patients with T2DM. Health care professionals play an important role in empowering patients and their caregivers by engaging them in discussions relating to insulin use, from addressing insulin-related concerns, to appropriate and safe use, and preventing and managing hypoglycaemia.
Recommendation 1: Start basal insulin if glycaemic targets are not met despite optimal treatment with non-insulin T2DM medications.
When progression of type 2 diabetes requires the introduction of insulin therapy, the use of basal insulin alone is one of the simplest and most convenient ways to do so. Basal insulin is used to control fasting blood glucose and can be categorised into intermediate- or long-acting insulin according to the time-action profile (see Table 1 below).
Intermediate-acting insulin isophane, or neutral protamine Hagedorn (NPH), has traditionally been used. It is usually injected once daily at bedtime. Long-acting insulin analogues (LAIAs) are as effective asNPH in lowering fasting blood glucose. LAIAs are associated with fewer hypoglycaemic events, especially nocturnal hypoglycaemia, but are more expensive than insulin NPH.6
The various LAIAs registered in Singapore (insulin detemir, insulin glargine, insulin degludec) are comparable in efficacy and safety. To achieve similar glycaemic control, insulin degludec and insulin glargine are usually injected once daily, whereas insulin detemir may need to be injected twice daily.7,8 Insulin degludec has the longest duration of action, which results in less nocturnal hypoglycaemia than insulin detemir and insulin glargine.8-11 Include cost considerations in choosing a basal insulin.
Notepad: Other indications for insulin therapy in T2DM This ACG focuses on the initiation of insulin therapy for patients with T2DM who are suboptimally controlled on other non-insulin diabetes medications. Insulin therapy should also be considered for patients with T2DM who are experiencing symptoms of hyperglycaemia or showing signs of ongoing catabolism (e.g. unexpected weight loss), regardless of their current non-insulin diabetes medications or stage of T2DM.5 Further assessment or referral may be warranted for such patients |
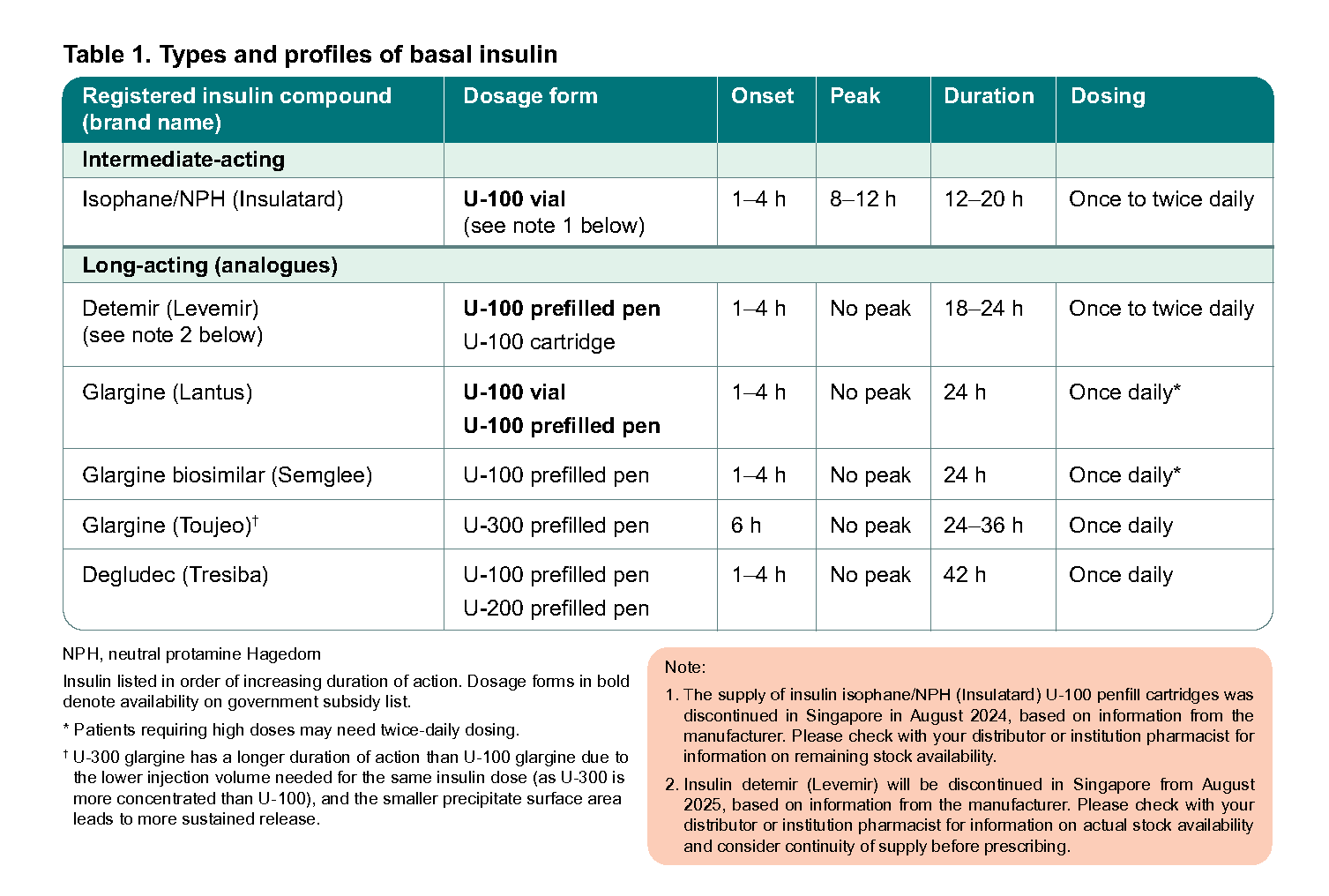
Table 1. Types and profiles of basal insulin
Notepad: Notes on insulin prescribing Different insulin compounds (Table 1), even within the same time-action category, are not identical and the decision to switch between products should be evaluated by the clinician. Include brand names when prescribing to distinguish between products and minimise errors. Biosimilars are biological products with physicochemical characteristics, biological activity, safety, and efficacy similar to their originator reference products12 and they may offer some cost savings. Insulin glargine biosimilars are non-inferior to reference insulin glargine in efficacy and safety.13 |
Notepad: Addressing concerns about starting insulin Many patients have concerns about starting insulin, with reported barriers including stigma and perceived failure, fear of injection and pain, concerns about weight gain, and fear of hypoglycaemia.14 These barriers contribute to a delay in the timely initiation of insulin, which is associated with suboptimal glycaemic control,15 and for some patients, the development of diabetes-related complications.16 Early conversations about the potential need for insulin and regular patient education can help address these barriers.17 |
Explaining the need for insulin therapy
|
Recommendation 2: Review concomitant T2DM medications when starting basal insulin and continue them at the current or lower dose where appropriate.
When starting basal insulin for a patient with T2DM, review the use of concomitant T2DM medications regularly, taking into account their benefits and risks, and considering the patient’s need for them as well as overall treatment burden.
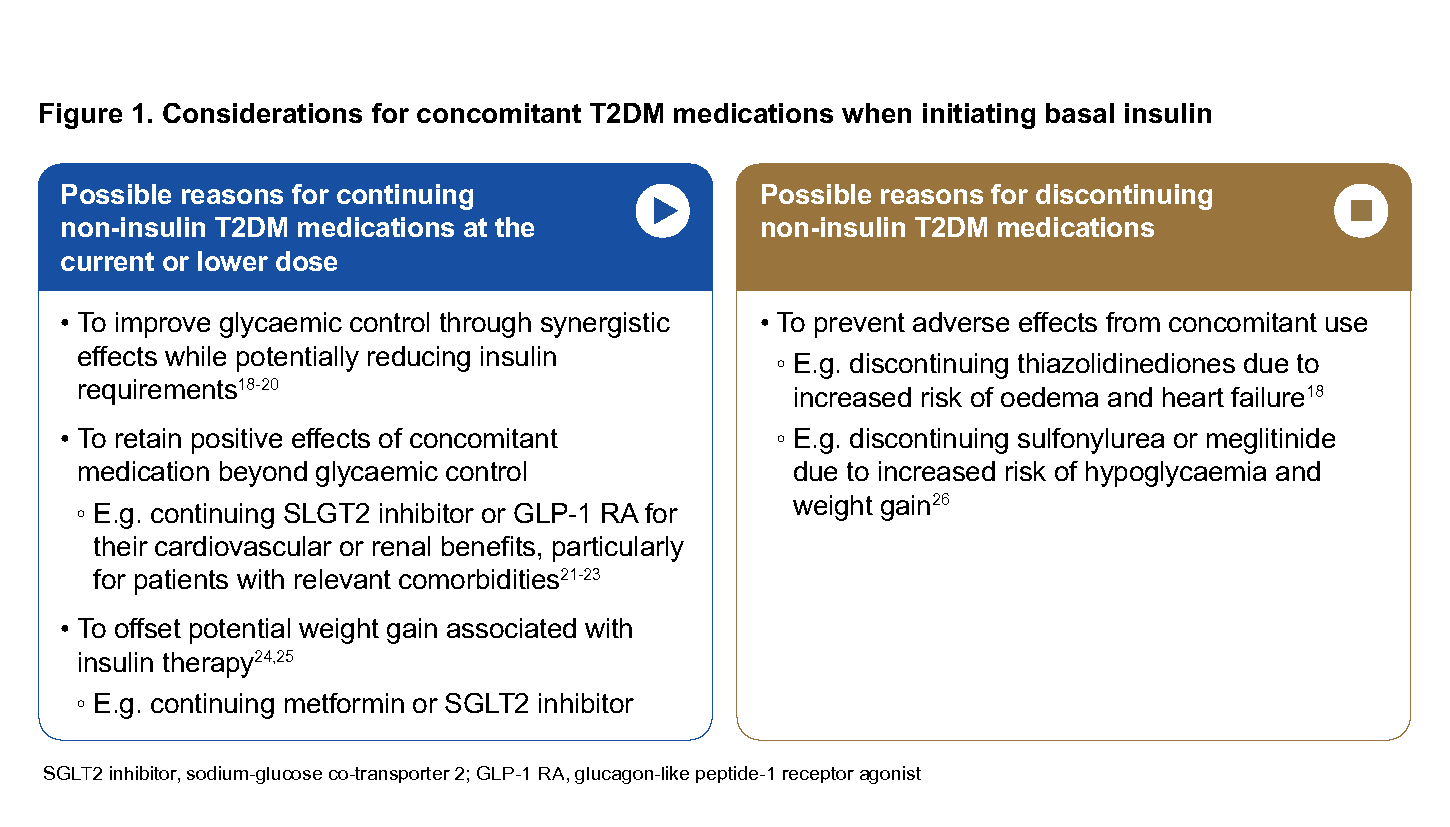
Figure 1. Considerations for concomitant T2DM medications when initiating basal insulin
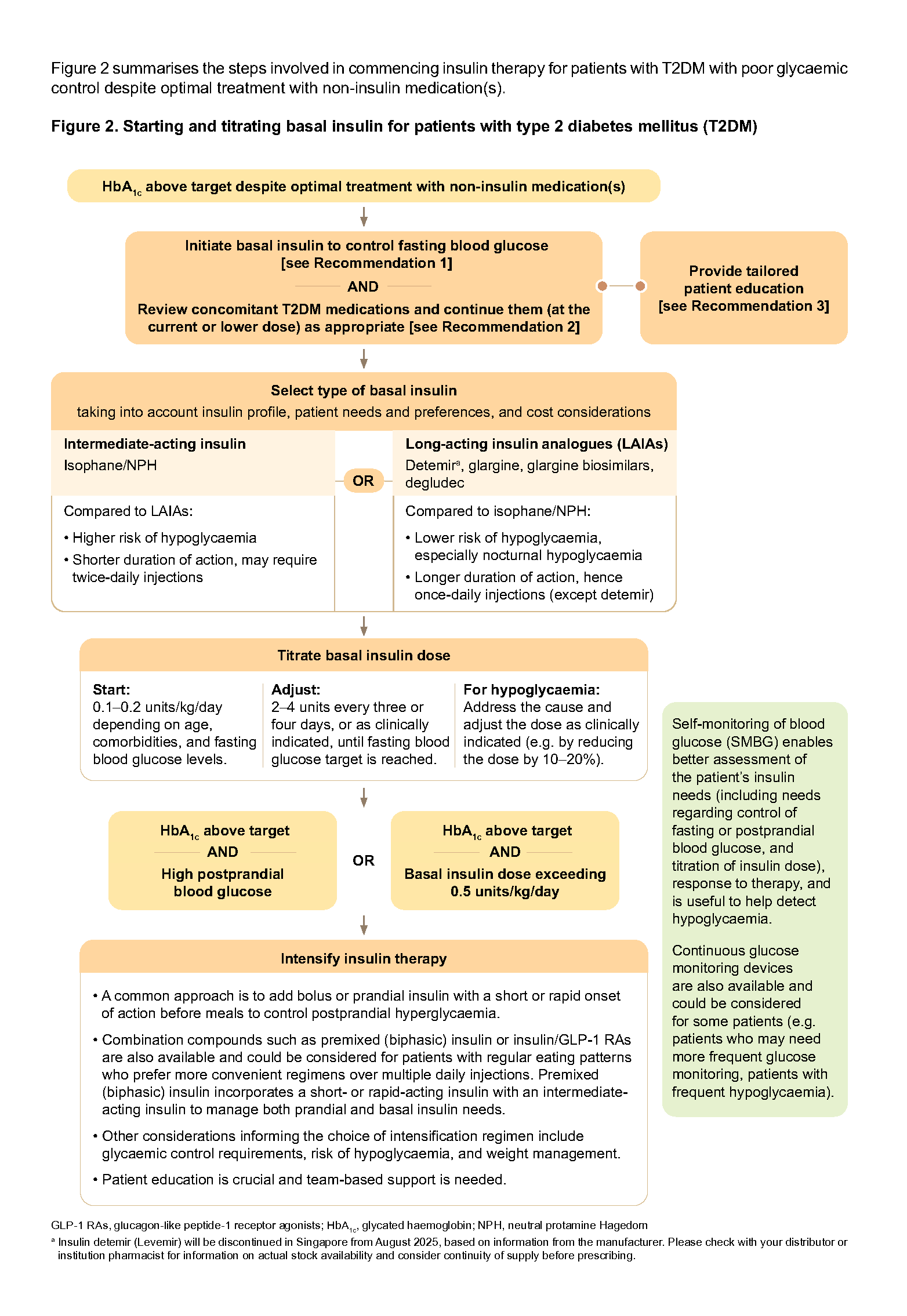
Figure 2. Starting and titrating basal insulin for patients with type 2 diabetes mellitus (T2DM)H
Click here for larger version of the image
Recommendation 3: Educate patients and their caregivers on how to use insulin safely and effectively, including how to prevent and manage hypoglycaemia.
When starting insulin therapy, it is critical to ensure that the patient and their caregiver are engaged in the process, and are equipped to manage their insulin use so that insulin therapy is not only safe, but also effective. Where feasible, enlist the support of other healthcare professionals in educating the patient and their caregiver.
Given the wide array of topics to cover, the discussion about insulin therapy needs to be tailored to each individual and the stage they are at. Some topics need to be addressed prior to starting (e.g. concerns with insulin use – see ‘Addressing concerns about starting insulin’ on page 3), others at the start of treatment (e.g. preventing and managing hypoglycaemia; insulin use and storage), and others as they become relevant across the patient’s life journey (e.g. fasting during Ramadan, or travelling while on insulin).
Preventing and managing hypoglycaemia
Hypoglycaemia (blood glucose level below 4 mmol/L) is a potentially serious adverse effect of insulin therapy. Hypoglycaemia is, therefore, a major limiting factor in achieving good glycaemic control. Prevention and prompt management of hypoglycaemia are crucial.
Hypoglycaemia is associated with many symptoms (Table 2) but is sometimes not perceived or experienced by the patient, including lack of early warning symptoms. This is known as hypoglycaemia unawareness and can be detected through blood glucose monitoring.
Patients who are at increased risk of hypoglycaemia include those with:
Advanced age
Renal impairment
Intensive or high-dose insulin regimens
Poor oral intake or prolonged fasting with high activity levels
Concurrent illness, such as infection or sepsis
Cognitive dysfunction
Polypharmacy or medication non-adherence
Individualise glycaemic targets for these patients as appropriate, and review insulin regimens (and concomitant T2DM medications) for patients with frequent hypoglycaemia or hypoglycaemia unawareness.
Notepad: Hypoglycaemia unawareness (HU) HU or impaired awareness of hypoglycaemia significantly increases the risk of severe hypoglycaemia, and HU has been reported in 9 to 18% of patients with insulin-treated T2DM.27 Patients with HU do not experience or perceive typical early warning symptoms of hypoglycaemia (such as tremors, palpitations, sweating) when their blood glucose is low. This may occur in patients with repeated hypoglycaemic events or in those with concomitant autonomic neuropathy. Advise patients with HU to raise their glycaemic targets for several weeks to months to avoid hypoglycaemia.28-30 Use of continuous glucose monitoring could be helpful. |
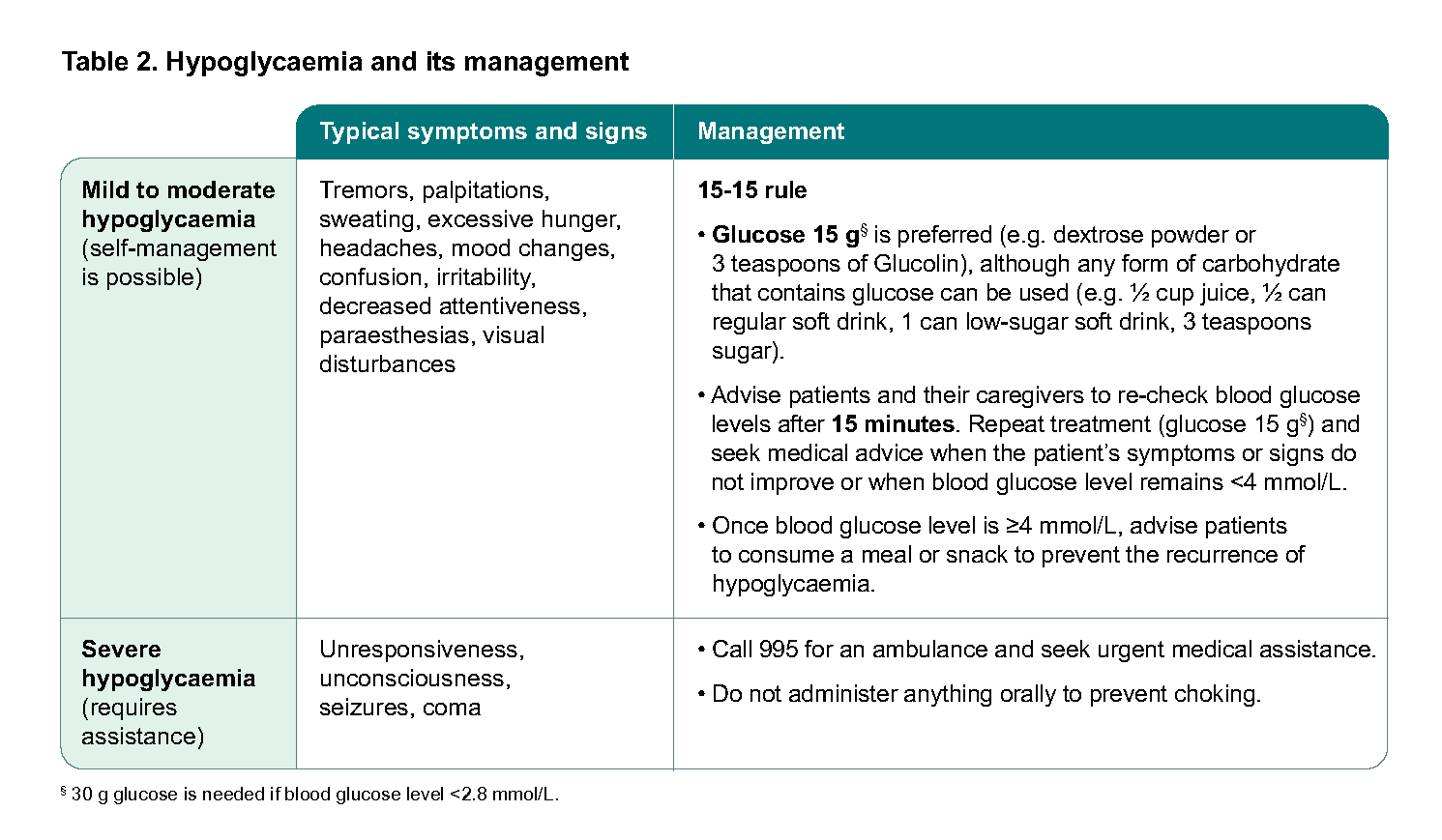
Table 2. Hypoglycaemia and its management
Insulin administration and storage
|
Diet
|
Fasting and physical activity
|
Sick days
|
Travel
|
Notepad: Patient information and resources on insulin Click the links below to access examples of patient information and resources from HealthHub which can be used to complement patient education about insulin.
|
Expert Group
Lead Discussant
A/Prof Goh Su-Yen, Endocrinology (SGH)
Chairperson
A/Prof Michelle Jong, Endocrinology (TTSH)
Members
Ms Kala Adaikan, Dietetics (SGH)
Ms Debra Chan Shu Zhen, Pharmacy (TTSH)
Dr Anthony Chao, Family Medicine (Boon Lay Clinic & Surgery Pte Ltd)
Dr Cheah Ming Hann, Family Medicine (NUP)
Dr Khoo Chin Meng, Family Medicine (NUHS)
Ms Lee Hwee Khim, Nursing (SHP)
Prof Joyce Lee, Pharmacy (UC Irvine)
Dr Phua Eng Joo, Endocrinology (KTPH)
Dr Darren Seah, Family Medicine (NHGP)
Clin Asst Prof Gilbert Tan Choon Seng, Family Medicine (SHP)
A/Prof Thai Ah Chuan, Endocrinology (NUH)
Feedback
Click here to give us feedback on this ACG.
Related ACGs
Type 2 diabetes mellitus – personalising management with non-insulin medications
Gestational diabetes mellitus — an update on screening, diagnosis, and follow-up
Other related resources
Diabetic Retinal Photography (DRP) Screening Technical Reference Guide
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Initiating basal insulin in type 2 diabetes mellitus. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2024. Available from: go.gov.sg/acg-initiating-basal-insulin-in-type-2-diabetes-mellitus
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.