
Gestational diabetes mellitus — an update on screening, diagnosis, and follow-up ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) features recommendations for identification of diabetes during pregnancy. It focuses on screening for pre-existing diabetes in women at increased risk, and on universal screening for gestational diabetes mellitus in all women at 24 to 28 weeks of gestation using IADPSG 2010 glucose thresholds. The ACG also highlights the importance of long-term follow-up and postpartum management for all women diagnosed with diabetes during pregnancy.
First published in 2018, this ACG has been updated in 2022 to incorporate the latest evidence where relevant.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
During their first trimester, screen for pre-existing diabetes in women at increased risk of it using non-pregnancy glucose thresholds. If results are normal, re-evaluate women for gestational diabetes mellitus (GDM) at 24 to 28 weeks of gestation.
At 24 to 28 weeks of gestation, screen all women for GDM using 3-point 75 g oral glucose tolerance test (OGTT) unless they have already been diagnosed with diabetes or pre-diabetes.
At 6 to 12 weeks after delivery, reassess glycaemic status in women with diabetes diagnosed during pregnancy using 2-point 75 g OGTT. If results are normal, screen women with a history of diabetes diagnosed during pregnancy for diabetes every 1 to 3 years (ideally annually) from then on.
Download the ACG and references in PDF
GDM – an update on screening, diagnosis, and follow-up (Aug 2022) [PDF]
GDM – an update on screening, diagnosis, and follow-up references (Aug 2022) [PDF]
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Managing GDM to improve outcomes
Women with diabetes during pregnancy (defined as glucose levels higher than normal, including diabetes, GDM, and pre-diabetes) are at increased risk of maternal and neonatal complications (such as pre eclampsia, macrosomia, and shoulder dystocia) compared to those without diabetes.1 When diabetes is first identified during pregnancy, this may represent undiagnosed pre-existing diabetes. GDM is diabetes diagnosed in the second or third trimester. The pathophysiology is often underlying ß-cell dysfunction or insulin resistance worsened by decreased insulin sensitivity during pregnancy.1,2
The prevalence of GDM in Eastern and Southeast Asian countries is approximately 1 in 10, which is higher than Western and African countries.3 In Singapore, GDM occurs in around 1 in 4 to 5 pregnant women—a higher prevalence than other countries in the Eastern and Southeast Asian region.3-5 History of GDM is associated with increased lifetime risk of diabetes for both the women and their babies.6-9 Appropriate management of GDM with diet, exercise, or insulin therapy can lower the risk of maternal and neonatal complications by up to 60%.10,11
First trimester: Screen for undiagnosed pre-existing diabetes in women at increased risk
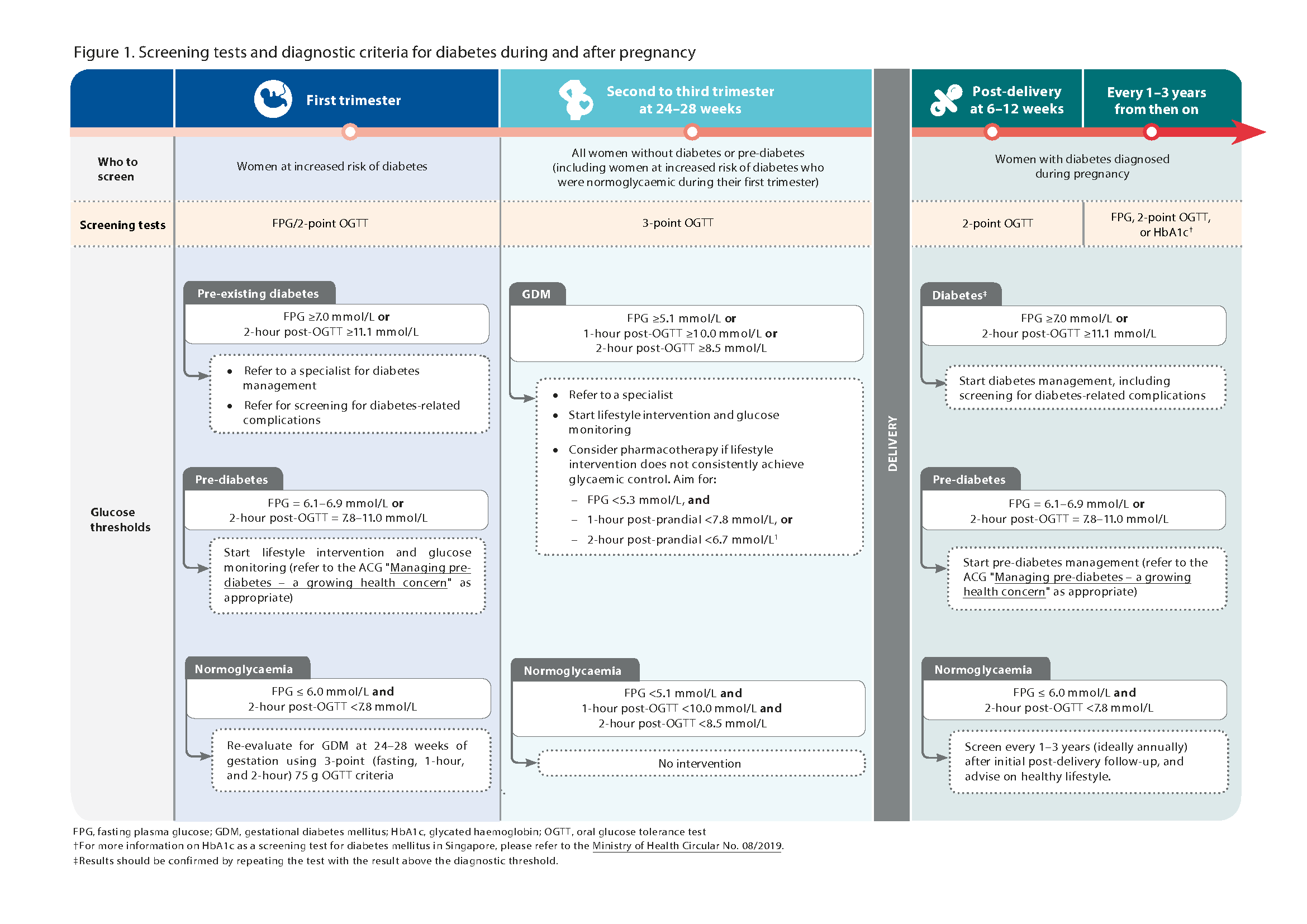
Before conception or during the first prenatal visit (first trimester), it is recommended to screen for pre-existing diabetes in women at increased risk of it using non-pregnancy thresholds.1
Women are considered to be at increased risk of pre existing diabetes if any risk factor is present, such as:
Pre-pregnancy body mass index (BMI) ≥ 23 kg/m2
History of GDM (or delivered a baby ≥ 4 kg)
History of polycystic ovary syndrome
History of pre-diabetes
Age ≥ 40 years
Family history of diabetes (first degree relative)–
Hypertension
Individual patient circumstances should also be taken into consideration when evaluating the need to test with fasting plasma glucose (FPG)/2-point 75 g OGTT.
If results are normal, re-evaluate women for GDM at 24 to 28 weeks of gestation.
While all women with diabetes diagnosed during pregnancy (including GDM) require timely management (including lifestyle intervention), those with pre-existing diabetes are at higher risk of poor diabetes outcomes than those with GDM. Hence, women with pre-existing diabetes require more stringent measures to reduce their risk of diabetes complications, including tighter glycaemic control and screening for complications (such as eye checks).1,7
24–28 weeks: Screen for GDM in all women without diabetes or pre-diabetes
Screening for GDM is recommended at 24 to 28 weeks of gestation because this phase coincides with an increase in gestational insulin resistance.12 With the higher prevalence of GDM in Asian populations, universal screening is favoured over risk-based screening for GDM.3,14
Apart from detecting more women with GDM, universal screening is associated with improved maternal and neonatal outcomes compared to risk based screening.14 At 24 to 28 weeks of gestation, use 3-point 75 g OGTT to screen all women for GDM—unless they have already been diagnosed with diabetes or pre-diabetes. This includes re-evaluating women at increased risk of pre-existing diabetes who had normal test results in their first trimester.
The International Association of Diabetes and Pregnancy Study Group (IADPSG) 3-point diagnostic criteria for GDM using 75 g OGTT have been adopted by many organisations, including the World Health Organization and Singapore's College of Obstetricians and Gynaecologists.15,16 These criteria are based on findings from the Hyperglycaemia and Adverse Pregnancy Outcomes study, a large observational study which included patients from Singapore.17
GDM is diagnosed if any of the IADPSG 3-point diagnostic criteria is met (Table 1). Compared to the previously used 2-point criteria,18 the IADPSG 3-point criteria identify a higher proportion of women at risk of adverse maternal and neonatal outcomes, so more women and their babies can benefit from appropriate GDM management.19
Table 1. GDM diagnostic criteria
Plasma glucose levels | IADPSG 3-point criteria* |
|---|---|
Fasting | ≥5.1 |
1-hour post-OGTT | ≥10.0 |
2-hour post-OGTT | ≥8.5 |
GDM, gestational diabetes mellitus; IADPSG, International Association of Diabetes and Pregnancy Study
Group; OGTT, oral glucose tolerance test
*All values in mmol/L.
Notepad: Avoiding HbA1c for screening and diagnosis of diabetes during pregnancy Glycated haemoglobin (HbA1c) should not be used to screen for or diagnose diabetes during pregnancy. It is not sensitive in detecting postprandial hyperglycaemia and is generally lower during pregnancy because of increased red blood cell turnover. Screening for diabetes during pregnancy with HbA1c has also not been validated locally. |

Post-pregnancy: Follow up women with diabetes diagnosed during pregnancy
Usually, plasma glucose reverts to pre-pregnancy levels six weeks after delivery. It is recommended that women whose diabetes was diagnosed during pregnancy (including diabetes, GDM, and pre-diabetes) be tested with 2-point (fasting and two-hour) 75 g OGTT between 6 to 12 weeks after delivery, to assess glycaemic status using non-pregnancy thresholds.20
Women with diabetes diagnosed during pregnancy who are found to have normal glycaemic status at 6 to 12 weeks after delivery should be regularly screened for diabetes every 1 to 3 years (ideally annually) from then on.1
Women with a history of GDM are about 10 times more likely to develop type 2 diabetes mellitus (T2DM) than women who had a normoglycaemic pregnancy.7 In Singapore, it is estimated that 4 in 10 women with a history of GDM develop T2DM or pre-diabetes within 4 to 6 years from delivery.21,22 Among women with a history of GDM, more frequent follow-up may be required for those who received insulin during pregnancy or those with other risk factors for developing diabetes such as non-pregnancy BMI ≥23 kg/m2 or a family history of diabetes.1,22
All women with diabetes diagnosed during pregnancy should receive timely management, including adopting a healthy lifestyle. For women with a history of GDM, lifestyle intervention (including healthy diet and increased physical activity) has been shown to reduce the progression from pre-diabetes to T2DM by 35% over 10 years.23
Click here for larger version of the image
Expert group
Lead discussants
Dr Claudia Chi (MEH)
Prof Chong Yap Seng (NUHS)
Chairperson
Prof Tan Kok Hian (KKH)
Group members
A/Prof Goh Su-Yen (SGH)
A/Prof Michelle Jong (TTSH)
Dr Khoo Chin Meng (NUHS)
A/Prof Lim Su Chi (KTPH)
Dr Ng Lai Peng (SHP)
Dr Desmond Ong (NUP)
Dr Adrian Tan (Healthmark Pioneer Mall Clinic)
A/Prof Tan Lay Kok (KKH)
Dr Teh Kailin (NHGP)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Managing pre-diabetes — a growing health concern
Initiating basal insulin in type 2 diabetes mellitus
Type 2 diabetes mellitus – personalising management with non-insulin medications
Foot assessment in people with diabetes mellitus
Diabetic Retinal Photography (DRP) Screening Technical Reference Guide
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Gestational diabetes mellitus – an update on screening, diagnosis, and follow-up. Appropriate Care Guide (ACG), Ministry of Health, Singapore. 2022. Available from: go.gov.sg/acg-gestational-diabetes-mellitus-an-update-on-screening diagnosis-and-follow-up
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.