
Gout — achieving the management goal ACG
Last updated 16 June 2026
Overview
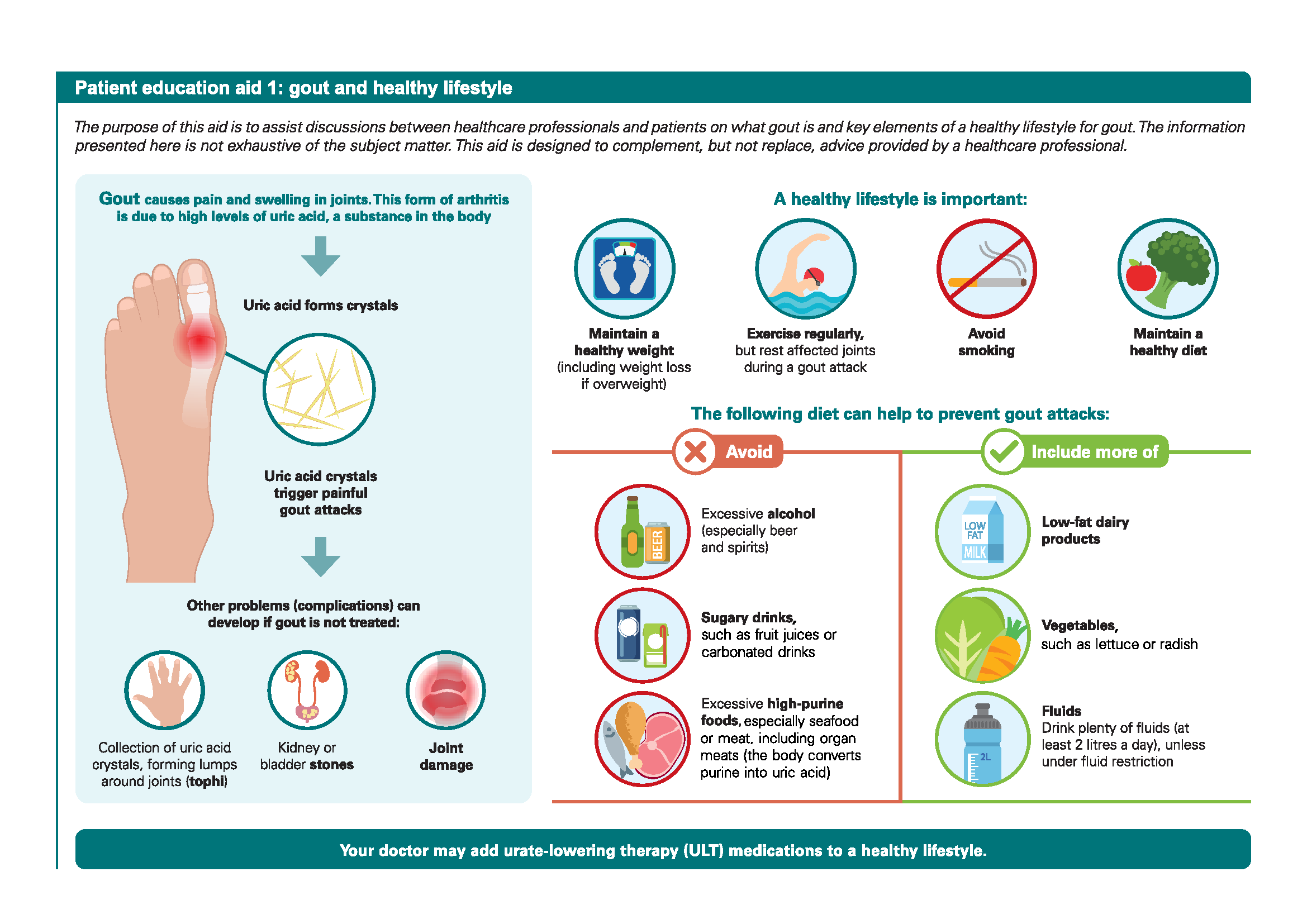
This ACE Clinical Guideline (ACG) highlights the pharmacological and non-pharmacological aspects of long-term management of gout, with a focus on urate-lowering therapy (ULT), prophylaxis, and acute flare treatment. Specifically, the ACG offers evidence-based recommendations on initiation of ULT for patients who meet the treatment criteria, provision of prophylaxis during the initial period of ULT, monitoring and risk mitigation for severe cutaneous adverse reactions (SCARs), as well as management of acute flares. Two patient education aids are included to assist discussions between healthcare professionals and patients.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Initiate urate-lowering therapy (ULT) for patients who meet the ULT treatment criteria, starting at a low dose and slowly titrating upwards as needed.
Provide prophylaxis with colchicine; if colchicine is not suitable, consider a low-dose oral nonsteroidal anti-inflammatory drug (NSAID), or a low-dose oral corticosteroid if NSAIDs are not suitable.
Mitigate the risk of developing severe cutaneous adverse reactions (SCARs) and provide counselling on SCAR monitoring for patients on allopurinol or febuxostat.
Manage acute flares as soon as possible, including treatment with colchicine, NSAIDs, or corticosteroids.
Download the ACG and references in PDF
Gout – achieving the management goal (Dec 2023) [PDF]
Gout – achieving the management goal references (Dec 2023) [PDF]
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.

Introduction
Gout, a form of inflammatory arthritis, is due to deposition of monosodium urate (MSU) crystals in one or more joints, and is a result of chronic serum urate elevation. Although gout is a chronic condition, it usually presents episodically with intense joint pain, swelling, and redness. Without appropriate long-term management, acute flares may increase in frequency or severity. Crystal build-up may form tophi that could lead to joint damage or functional impairment. In addition, renal complications, such as urate nephrolithiasis or chronic kidney disease (CKD) may develop. As CKD is also a known risk factor for gout, the relationship between the two is bidirectional. Also, patients with gout often have multiple comorbidities, including obesity, metabolic syndrome, type 2 diabetes mellitus, and cardiovascular disease.
This ACG highlights the need for improved management of gout as a chronic condition, beyond managing acute, episodic exacerbations. When lifestyle management is insufficient, urate-lowering therapy (ULT) is the mainstay of the long-term management approach to gout.1,2
Ensuring long-term management
The management goal for gout is resolution of symptoms and signs, so as to reduce the risk of further complications. A long-term approach to managing gout should be in place for all patients, and this includes going beyond episodic treatment of acute flares:
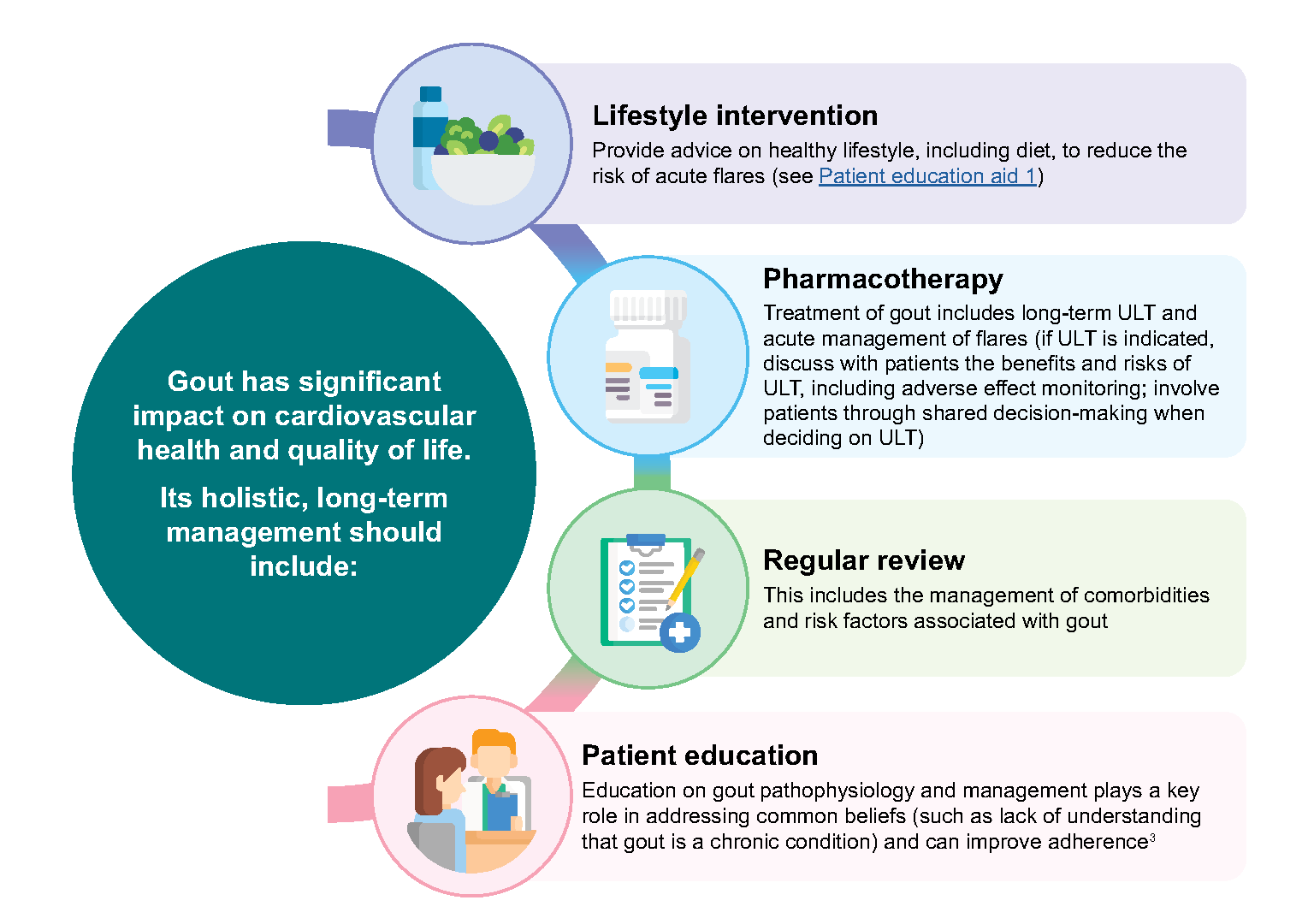
Figure 1 provides an overview of long-term management of gout.
Notepad: Gout and asymptomatic hyperuricaemia Gout is the clinical manifestation of MSU crystal deposition from chronic serum urate elevation. In contrast, asymptomatic hyperuricaemia refers to elevated serum urate without symptoms or signs.4 Unlike in gout management, evidence on using ULT to treat asymptomatic hyperuricaemia is not established, and advice on lifestyle could be given to patients with persistent asymptomatic hyperuricaemia. Although gout stems from chronic serum urate elevation, serum urate naturally fluctuates, and therefore serum urate levels may not always correspond to clinical features of gout. |
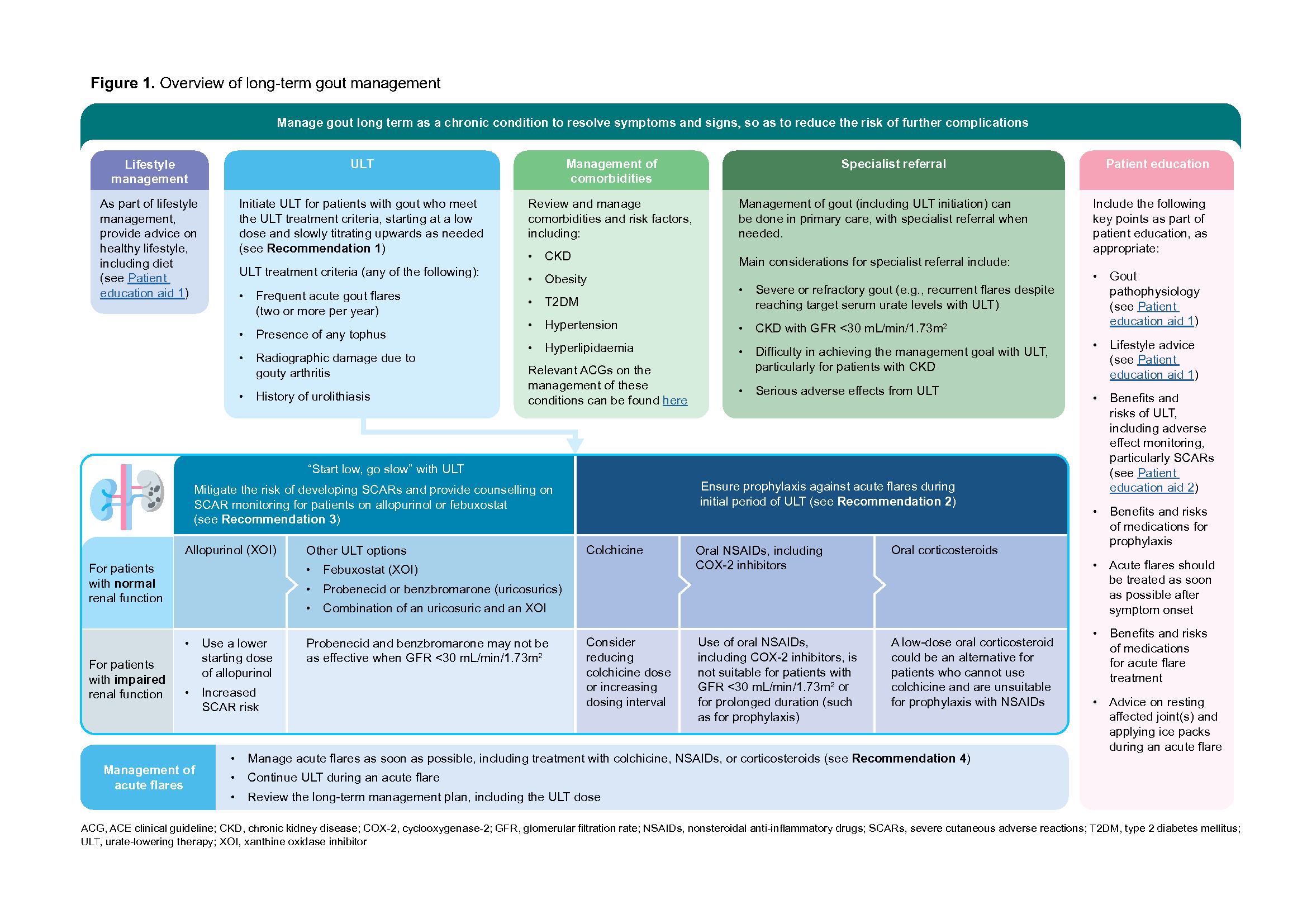
Figure 1. Overview of long-term gout management
Click here for larger version of the image
ULT for gout management
Using ULT to achieve the management goal
The management goal for gout focuses on resolution of symptoms and signs, to minimise risk of complications. This includes resolving tophi and reducing acute flares, which can be achieved through lowering of serum urate with ULT.
Recommendation 1: Initiate urate-lowering therapy (ULT) for patients who meet the ULT treatment criteria, starting at a low dose and slowly titrating upwards as needed.
Consider starting patients on ULT, particularly when they meet ULT treatment criteria (see Table 1). Involve patients through shared decision-making when deciding on ULT. Generally, the effects of ULT on decreasing acute flare frequency and tophi number or size are greater when serum urate is reduced and maintained <360 μmol/L (6 mg/dL) for the long term.8-10 Further reductions in flare frequency and tophi may be experienced with lower serum urate levels11 such as below 300 μmol/L (5 mg/dL), although higher ULT doses may be required.
When using ULT, consider starting with allopurinol – a xanthine oxidase inhibitor (XOI) that is effective, generally well tolerated, and commonly used. Febuxostat is a newer XOI. While allopurinol and febuxostat have similar benefitsa for reducing acute flare frequency8,12 or tophi,10,13,14 research suggests a higher risk of all-cause and cardiovascular death with febuxostat compared to allopurinol for patients with gout and major cardiovascular disease (CVD).15 Among patients without CVD, recent evidence indicates the cardiovascular risk of these two XOIs may not differ.16
Table 1. ULT treatment criteria
Any of the following: |
|---|
|
|
|
|
ULT, urate-lowering therapy |
When initiating allopurinol, start at a low dose (typically 50–100 mg/day). Slowly titrate upwards in 50–100 mg increments every four to eight weeks, informed by serum urate and clinical features (“start low, go slow”). Allopurinol doses of more than 300 mg/day may be needed to achieve the management goal. Doses could be increased up to a maximum of 900 mg/day in patients with normal renal function.b
Notepad: Allopurinol in renal impairment In patients with renal impairment,c use a lower starting dose of allopurinol.17 The maximum maintenance dose of allopurinol in patients with renal impairment is not well established, although doses higher than 300 mg/day could be used safely with adequate patient education and monitoring.1 |
Information in this notepad was sourced from package insert and supplemented with information from UpToDate (www.uptodate.com). Please refer accordingly for full details on allopurinol.
Uricosuric agents are another class of ULT, and include probenecid and benzbromarone. As they promote urate excretion through the kidneys, these agents are less effective in patients with renal impairmentc (see Table 2). An uricosuric agent could be used alone or in combination with an XOI (usually allopurinol) for enhanced effectiveness, if there is inadequate response to an XOI alone. Benzbromarone is not commonly used locally.
“Start low, go slow” with ULT, informed by serum urate and clinical features.
a Comparing febuxostat 80 mg/day to allopurinol 300 mg/day.
b Information sourced from package insert. Please refer to package insert or drug information references for full details on allopurinol.
c In this ACG, ‘CKD’ refers to the specific condition defined by the diagnostic criteria of glomerular filtration rate <60 mL/min/1.73m2, urine albumin:creatinine ratio ≥3 mg/mmol (≥30 mg/g), or other marker of kidney damage, for at least three months. ‘Renal impairment’ is used as a broader term that includes CKD as well as acute kidney impairment.
Addressing clinical precautions of using ULT
A summary of clinical precautions when using ULT is presented in Table 2. Main considerations for specialist referral and key points for patient education can be found in Figure 1.
Table 2. Key clinical precautions with ULT*
Xanthine oxidase inhibitors | Uricosuric agents | ||
|---|---|---|---|
Allopurinol† | Febuxostat | Probenecid† | Benzbromarone |
|
|
| |
Risk of haemolytic anaemia in patients with G6PD deficiency | Withdrawn in some countries following reports of hepatotoxicity18 | ||
May precipitate acute flares during initial period of ULT (see section “Prophylaxis against acute flares during initial period of ULT” below) | |||
GFR, glomerular filtration rate; G6PD, glucose-6-phosphate dehydrogenase; SCARs, severe cutaneous adverse reactions; ULT, urate-lowering therapy
* Information sourced from package inserts and UpToDate (www.uptodate.com). Please refer accordingly for full details on these medications.
†Available on government subsidy list
Prophylaxis against acute flares during initial period of ULT
Recommendation 2: Provide prophylaxis with colchicine; if colchicine is not suitable, consider a low-dose oral nonsteroidal anti-inflammatory drug (NSAID), or a low-dose oral corticosteroid if NSAIDs are not suitable.
To mitigate the risk of acute flares when initiating ULT, provide prophylaxis with colchicine, typically 0.5 mg or 0.6 mg once daily. Prophylaxis with colchicine is generally recommended for up to six months.19 However, prophylaxis duration could be tailored depending on the occurrence of acute flares. Starting ULT at a low dose before slowly titrating upwards also helps to mitigate the risk of acute flares.20
For patients who cannot use colchicine, consider a low-dose oral nonsteroidal anti-inflammatory drug (NSAID), including a cyclooxygenase-2 (COX-2) inhibitor. Alternatively, a low-dose oral corticosteroid could be considered for patients who cannot use colchicine, and who are unsuitable for prophylaxis with NSAIDs (such as patients with renal impairment). Optimal prophylaxis duration with these non-colchicine medications is not established.
Notepad: Colchicine adverse effects and interactions Nausea, vomiting, and diarrhoea are the most common adverse effects of colchicine. The frequency of adverse effects increases with higher doses or longer duration of use. Colchicine has the potential for many drug-drug (such as macrolide antibiotics, azole antifungals, statins, verapamil, or diltiazem) and drug-food interactions.‡ Monitor for adverse effects due to drug-drug interactions and consider reducing the dose of colchicine or increasing dosing interval as required. Clinical decisions should be individualised, taking into consideration the importance of patients’ concurrent medications for their respective conditions. Patients with renal or hepatic impairment are at increased risk of toxicity, including myopathy, neuropathy, and pancytopenia.‡ |
Medications for prophylaxis are also used to treat acute flares (see section “Managing acute flares” below). If an acute flare occurs during prophylaxis and the same medication for prophylaxis is chosen to treat the acute flare, use the higher acute flare treatment dose instead of the prophylactic dose. Reinitiate the prophylactic dose after the acute flare resolves. If a different medication is chosen to treat the acute flare, exercise more caution with the combination of an oral NSAID plus an oral corticosteroid due to the increased risk of gastrointestinal ulcer or bleeding.
Notepad: Anti-inflammatory medications in renal impairment Renal impairment affects treatment options both in prophylaxis and treatment of acute flares:
|
‡ Please refer to package insert or drug information references for full details on prophylactic medications, including contraindications.
Understanding severe cutaneous adverse reactions (SCARs) in ULT
Recommendation 3: Mitigate the risk of developing severe cutaneous adverse reactions (SCARs) and provide counselling on SCAR monitoring for patients on allopurinol or febuxostat.
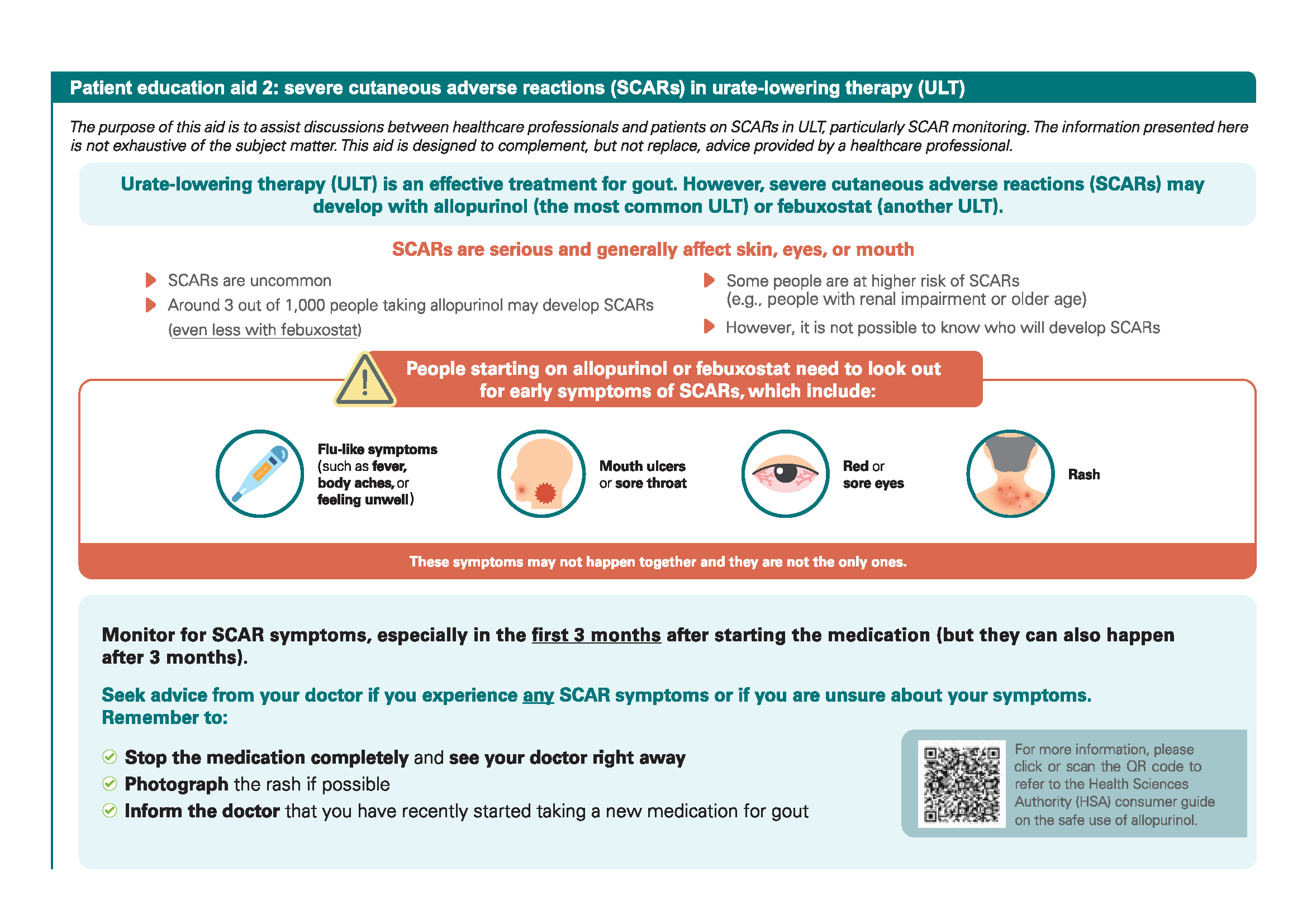
Allopurinol/febuxostat-induced SCARs are uncommon. They include Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS). SCARs may result in long-term complications and even be life-threatening. Most SCARs occur within the first few weeks to months after therapy initiation. Monitoring for SCARs in patients starting on allopurinol or febuxostat is important to ensure early detection and prompt management. While a number of SCAR risk factors exist, the acronym RASHES below presents key factors to guide clinical decision-making.
Around 3 out of 1,000 patients on allopurinol may develop SCARs21 (even less with febuxostat)22
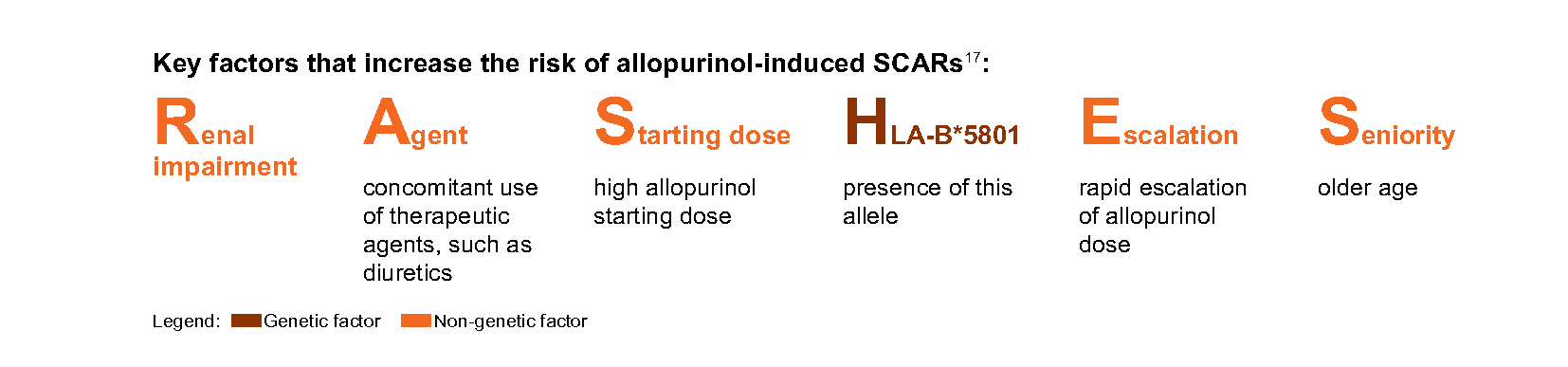
Assess the RASHES factors in all patients starting on allopurinol. Mitigate the risk of developing SCARs by addressing the RASHES factors where possible, for example by starting allopurinol at a low dose and slowly titrating upwards. Patients with renal impairment or older age are inherently at increased risk of SCARs. Nonetheless, monitoring for SCARs is important in all patients starting on allopurinol. This includes educating patients on the early symptoms of SCARs and actions to take if such symptoms are experienced (see Patient education aid 2). Abnormalities in laboratory tests such as full blood count, alanine aminotransferase, and aspartate transaminase may be indicative of SCARs.d
While the HLA-B*5801 allele is a known risk factor for allopurinol-induced SCARs, reactions may still develop without the allele as there are non-genetic factors that increase the risk. The positive predictive value (PPV) of HLA-B*5801 for allopurinol induced SCARs is estimated at around 2% (around 2 out of 100 patients with the allele starting on allopurinol may develop SCARs). The low PPV limits the overall value of routine genotyping in the Singapore population before initiation of allopurinol and routine genotyping of all patients with gout is not recommended. For patients assessed to already be at higher risk of allopurinol-induced SCARs with renal impairment or older age, the option of HLA-B*5801 genotyping may be considered prior to allopurinol initiation, taking into account cost considerations. For patients who have already well tolerated long-term allopurinol treatment, genotyping is not required.
For more information on allopurinol induced SCARs, please click here to access the 2021 reminder of the Ministry of Health (MOH) – Health Sciences Authority (HSA) Drug Safety Information No. 59 summary (first published on 21 September 2016). |
SCARs have also been reported with febuxostat, although the risk is significantly lower than with allopurinol.22 Post-marketing surveillance found that some of the patients who developed SCARs with febuxostat had renal impairment or a history of hypersensitivity to allopurinol.23
“Start low, go slow” with ULT to minimise the risk of adverse effects. Inform patients of SCAR risk and provide counselling on SCAR monitoring (see Patient education aid 2).
dPlease refer to the Chronic Disease Management Programme handbook for further information on care components for patients with gout, including monitoring parameters and frequencies.
Managing acute flares
Recommendation 4: Manage acute flares as soon as possible, including treatment with colchicine, NSAIDs, or corticosteroids.
Acute flares should be treated as soon as possible. Anti-inflammatory medications for treatment of acute flares include:
Colchicine
Oral NSAIDs, including COX-2 inhibitors
Oral corticosteroidse
Intra-articular or intramuscular corticosteroids
Monotherapy or a combination of medications can be used. However, exercise more caution with the combination of an oral NSAID plus an oral corticosteroid. See notepads under section “Prophylaxis against acute flares during initial period of ULT” for more information on anti-inflammatory medications.
Notepad: Low-dose colchicine for acute flares Use one of the following low-dose colchicine regimens for acute flare treatment: One-off treatment with 1 mg or 1.2 mg loading dose, followed by one dose of 0.5 mg or 0.6 mg one hour later24 OR 0.5 mg or 0.6 mg two to three times per day until the acute flare resolves Historically, acute flares were treated with a higher dose of colchicine, starting with 1 mg loading dose, followed by 0.5 mg every four hours until acute pain improved, patient felt sick, or had diarrhoea.§ However, there is a greater likelihood of gastrointestinal adverse effects with higher doses of colchicine, without added benefits.24 |
§ Information sourced from package insert.
Practice considerations when managing an acute flare: |
|---|
Determine the choice of treatment by considering patient characteristics such as comorbidities (e.g., renal impairment), concomitant medications, and patient preferences. |
Advise patients to rest affected joint(s) and apply ice packs. |
ULT could be initiated during an acute flare provided that the acute flare is adequately treated, followed by prophylaxis. However, delaying the initiation until after the acute flare subsides is also an option. |
For patients who are on ULT, continue ULT during an acute flare. Review the long-term management plan, including the ULT dose. As serum urate naturally fluctuates, serum urate levels may be normal or low during an acute flare. |
eOral corticosteroids, such as prednisolone 20 to 30 mg/day for three to seven days for treatment of an acute flare.
Click here for larger version of the image
Click here for larger version of the image
Expert group
Lead discussants
Dr Koh Kim Hwee, Family Medicine (SHP)
Dr Tan Teck Choon, Rheumatology (KTPH)
Chairperson
Adj A/Prof Bernard Thong Yu Hor, Rheumatology (TTSH)
Members
Dr Wilson Eu Tieng Juoh, Family Medicine (Sennett Medical Clinic)
Dr Goh Su Mein, Nephrology (TTSH)
Dr Lee Haur Yueh, Dermatology (SGH)
Dr Richard Lee Meng Kam, Family Medicine (NHGP)
Ms Cheryl Lim Yu Ling, Pharmacy (SGH)
Dr Sharon Ngoh Hui Lee, Family Medicine (AMK FMC)
Dr Poh Yih Jia, Rheumatology (SGH)
Dr Adrian Poh Zhongxian, Family Medicine (OneCare Medical)
Dr Teng Gim Gee, Rheumatology (Alexandra Hospital)
Dr Cynthia Wong Sze Mun, Family Medicine (NUP)
Dr Wong Wei Mon, Family Medicine (St Luke’s Hospital)

Feedback
Click here to give us feedback on this ACG.
Related ACGs
Chronic kidney disease — early detection
Chronic kidney disease — delaying progression and reducing cardiovascular complications
Type 2 diabetes mellitus — personalising management with non-insulin medications
Hypertension — tailoring the management plan to optimise blood pressure control
Lipid management: focus on cardiovascular risk
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Gout – achieving the management goal. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-gout-achieving-management-goal
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.