
Chronic kidney disease — early detection ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) highlights the importance of early identification of patients at increased risk of chronic kidney disease (CKD), providing evidence-based recommendations for timely detection, diagnosis, and staging of CKD.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Identify patients at increased risk of CKD by assessing their risk factors and determine the need to evaluate for CKD.
Diagnose CKD if any of the following is present for at least three months:
GFR < 60 mL/min/1.73m2
UACR ≥ 3 mg/mmol (≥ 30 mg/g)
Other marker of kidney damage
Determine the stage of CKD based on GFR, UACR, and the cause(s) of CKD.
For patients diagnosed with CKD, discuss the diagnosis and management options with the patient.
For patients who do not have CKD but are at increased risk, monitor for CKD regularly.
Referral to a specialist could be made at any point.
Download the ACG and reference in PDF
CKD – early detection (Oct 2022) [PDF]
CKD – early detection References (Oct 2022) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.Callout content
Introduction
Chronic kidney disease (CKD) is defined as abnormalities of kidney function or structure persisting for at least three months, with implications for health.1 In 2017, the estimated global prevalence of CKD was 9.1%.2 In Singapore, the prevalence of CKD among residents aged 18 to 74 years was 8.8% in 2019–2020,3 and CKD has remained in the top ten causes of death from 2009 to 2019 with CKD-related deaths rising by 76% within that decade.4
Timely CKD detection and management play a major part in slowing down or preventing progression to kidney failure or other complications. Early detection is particularly significant given that patients are asymptomatic in the early stages of CKD. Primary healthcare professionals play an essential role in identifying patients at increased risk of CKD to detect it early.
Identification of patients at increased risk of CKD
Recommendation 1: Identify patients at increased risk of CKD by assessing their risk factors and determine the need to evaluate for CKD.
Identifying patients at increased risk who will benefit from evaluation for CKD enables timely detection and management of CKD.1 This involves assessing the patient’s overall risk of CKD, as well as other aspects of the patient’s health status (for example, their age and frailty) to determine the extent to which they can benefit from evaluation for CKD.
Key risk factors associated with the overall risk of CKD are listed in Table 1.
Table 1. Risk factors for CKD*
Cardiometabolic risk factors | Renal risk factors | Other risk factors |
Cardiovascular disease | Family history of CKD or ESKD | Age (especially ≥ 65 years) |
Diabetes mellitus+ | Hereditary kidney disease | Hyperuricaemia or gout |
Hypertension+ | History of AKI | Nephrotoxic medications (including frequent or chronic NSAID use) |
Obesity (BMI ≥ 27.5 kg/m2) | Recurrent kidney stones | |
Metabolic syndrome | Multi-system diseases that impact the kidneys (such as SLE) | Smoking |
AKI, acute kidney injury; BMI, body mass index; CKD, chronic kidney disease; ESKD, end-stage kidney disease; NSAID, non-steroidal anti-inflammatory drug; SLE, systemic lupus erythematosus
*This table presents more commonly known risk factors for CKD; it is not an exhaustive list. Bolding denotes risk factors that are particularly important for CKD.
+Including presentations associated with pregnancy.
Cardiovascular disease, diabetes, hypertension, and obesity are particularly important risk factors for CKD (in bold in Table 1). The cardiometabolic risk inherent in these risk factors, that is, high blood glucose, high blood pressure, and high BMI─along with related risk factors such as hyperlipidaemia and smoking─are modifiable and can be managed to reduce the patient’s risk of CKD and associated significant comorbidities or complications, including cardiovascular mortality.
While recognising risk factors is integral to assessing the patient’s overall risk of CKD, this does not mean that all patients with CKD risk factors would require evaluation for CKD. For example, evaluation for CKD may be prudent for a healthy 40-year-old patient with a strong family history of CKD despite their young age, but may not be warranted for a healthy 40-year-old patient who is a social smoker.
Recommendation 2 under CKD diagnosis and Recommendation 3 under CKD staging provide more details on evaluation for CKD.
CKD diagnosis
Recommendation 2: Diagnose CKD if any of the following is present for at least three months:
-GFR <60 mL/min/1.73m2
-UACR ≥3 mg/mmol (≥30 mg/g)
-Other marker of kidney damage
Evaluation for CKD involves investigating for abnormalities of kidney function or structure in relation to the diagnostic criteria for CKD as shown above.
Evaluating kidney function─GFR
Glomerular filtration rate (GFR) is generally accepted as the best overall index of kidney function.1 As measuring ‘true’ GFR is cumbersome and difficult to perform accurately, serum creatinine-based estimating equations are commonly used to obtain the estimated GFR (eGFR). GFR is a more sensitive marker for CKD than serum creatinine alone.1,5,6 GFR <60 mL/min/1.73m2 is internationally accepted as the threshold for CKD, and is associated with increased risk of adverse renal outcomes (including higher risk of CKD progression, dialysis, CKD-related death, and AKI), cardiovascular and all-cause mortality.7-10
Notepad: eGFR equations: MDRD and CKD-EPI The Modification of Diet in Renal Disease (MDRD) and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations both estimate GFR based on serum creatinine, age, gender, and are adjusted for body surface area. CKD-EPI is more accurate, particularly at higher GFR, enabling reporting of numeric values for GFR up to 90 mL/min/1.73m2 (relevant for more detailed staging of CKD─see Recommendation 3 starting on page 5). |
Notepad: Acute kidney injury Acute kidney injury (AKI) is defined as any of the following:11,12
While evaluating patients for CKD, be cognisant of the possibility of AKI. If AKI is suspected, repeat a serum creatinine test as soon as practicable (other tests may also be required). Patients with eGFR <60 mL/min/1.73m2, particularly when AKI is suspected, should have a repeat serum creatinine as soon as practicable to rule out AKI. |
Evaluating kidney damage─UACR or other markers of kidney damage
Albuminuria is a common marker of kidney damage, as albumin is the main protein found in urine in many presentations of kidney diseases, including CKD resulting from diabetes or hypertension. Urine albumin:creatinine ratio (UACR) is the recommended measure of albuminuria instead of urine protein:creatinine ratio (UPCR) because UACR is better than UPCR for detecting early progressive kidney damage. 1,13-15 UACR ≥3 mg/mmol (≥30 mg/g) is internationally accepted as the threshold for CKD, and is associated with increased risk of adverse renal outcomes (including higher risk of CKD progression, dialysis, CKD-related death, and AKI), cardiovascular and all-cause mortality.7-10
Other markers of kidney damage may be used for diagnostic purposes in addition to, or instead of, albuminuria. Examples include urine sediment abnormalities (such as casts) and imaging abnormalities (such as hydronephrosis on ultrasound). A history of kidney transplantation is also considered a marker of kidney damage and immediately qualifies as CKD (regardless of GFR or UACR levels).
Notepad: Albuminuria threshold For ease of clinical application and in line with international consensus, this clinical guidance adopts a common albuminuria threshold of UACR ≥3 mg/mmol (≥30 mg/g) for both males and females,1 while acknowledging that gender-specific thresholds may still be used in some practice settings in Singapore. Patients should be appropriately tested and followed up whether common or gender-specific thresholds are used. |
Table 2. Key information for ordering and interpreting eGFR and UACR
eGFR | UACR | |
|---|---|---|
When to repeat the test | Repeat 3 months after the initial test to confirm if patient has CKD (may also be repeated sooner if clinically indicated). | Repeat 3 months after the initial test to confirm if patient has CKD (may also be repeated sooner if clinically indicated). |
Factors that could influence the test results (without necessarily affecting kidney function) | Factors that could increase serum creatinine (hence decrease eGFR) include:1,16 • High muscle mass • High-protein diet • Medications that increase serum creatinine without necessarily affecting kidney function (for example, trimethoprim) Factors that could decrease serum creatinine (hence increase eGFR) include: 1,16 • Low muscle mass (for example, patients with sarcopaenia, paraplegia, amputation, or muscular dystrophy) • Malnutrition, inflammation, or deconditioning (for example, patients with cancer or severe cardiovascular disease, hospitalised patients) • Low-protein diet | Factors that could increase albuminuria (hence increase UACR) include:1,17 • Menstruation • Urinary tract infection • Heavy exercise within last 24 hours • Congestive heart failure Factors that could decrease urine creatinine (hence increase UACR):1 • Female gender • Older age • Low muscle mass (for example, patients with sarcopaenia, paraplegia, amputation, or muscular dystrophy) |
Practical considerations | Advise patient to abstain from high-protein food such as meat for 12 hours prior to the test.18 Patients with eGFR <60 mL/min/1.73m2 should have a repeat serum creatinine as soon as practicable to rule out AKI, particularly when AKI is suspected. | A 24-hour collection is not necessary. An early morning spot urine sample is preferred as it correlates well with 24-hour protein excretion, and has relatively low intra-individual variability. A UACR ≥3 mg/mmol (≥30 mg/g) based on a random urine sample should be repeated on an early morning urine sample. |
AKI, acute kidney injury; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; UACR, urine albumin:creatinine ratio
Notepad: Incidental dipstick findings19 During routine health screening, such as annual medical examinations, a urine dipstick test may detect proteinuria or haematuria. False-positive and false-negative results are not unusual in dipstick urinalysis. Any findings of concern, for example persistent proteinuria or haematuria, should prompt further investigations to rule out serious aetiologies. |
CKD staging
Recommendation 3: Determine the stage of CKD based on GFR, UACR, and the cause(s) of CKD.
Once CKD is diagnosed, the stage of CKD needs to be determined to inform prognosis and management. CKD staging is based on cause and severity, with the latter reflected by GFR and UACR. This is a shift away from previous approach where CKD staging only focused on GFR.1 GFR and UACR are categorised quantitatively, while cause is described qualitatively. All three form essential components of CKD staging.
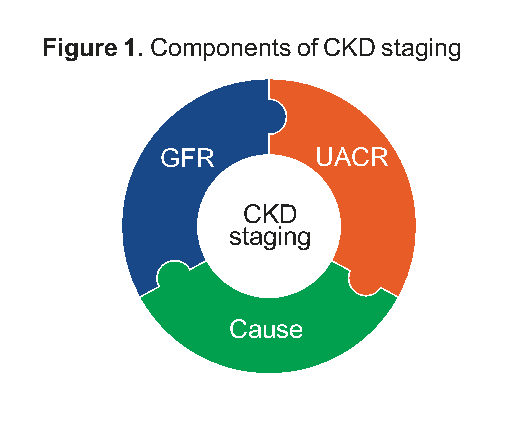
Figure 1. Components of CKD staging
GFR continues to be used in CKD staging as the overall marker of the severity of reduced kidney function.
Category | Description | GFR range (mL/min/1.73m2)‡ |
|---|---|---|
G1 | Normal or high | ≥90 |
G2 | Mildly decreased | 60-89 |
G3a | Mildly to moderately decreased | 45-59 |
G3b | Moderately to severely decreased | 30-44 |
G4 | Severely decreased | 15-29 |
G5 | Kidney failure | <15 |
‡Range based on kidney disease: Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.1
UACR (measuring albuminuria) is included as another component of CKD staging not only because it is a marker of kidney damage severity, but also because it is associated with the progression of kidney disease.
Category | Description | UACR range§ | |
|---|---|---|---|
(mg/mmol) | (mg/g) | ||
A1 | Normal to mildly increased | <3 | <30 |
A2 | Moderately increased | 3-30 | 30-300 |
A3 | Severely increased | >30 | >300 |
§Range based on Kidney Disease: Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.1
The cause of disease is included as part of CKD staging as it is fundamentally important in prognostication and choice of cause-specific treatments. The cause of CKD should be established by considering findings from the patient’s history and physical examination. For many patients, the risk factor(s) prompting evaluation for CKD in the first place (such as diabetes, hypertension, or family history of CKD) may offer a plausible cause of CKD. Clinical judgement needs to be exercised regarding whether this provides a sufficient explanation, or whether further investigations are warranted to determine the cause (or in some cases, additional causes), for example:1
Complete urinalysis (including urine microscopy) to detect haematuria, pyuria, or casts
Ultrasound to examine kidney structure
Serum and urine electrolytes to investigate for renal tubular disorders
Unlike GFR and UACR which can be quantified and categorised numerically in CKD staging, cause is described qualitatively. Collectively, the quantitative (GFR and UACR) and qualitative (cause) components of CKD staging provide essential information to determine the patient’s prognosis and most appropriate management. The importance of each component of CKD staging is illustrated through some clinical scenarios in Figure 2 below.
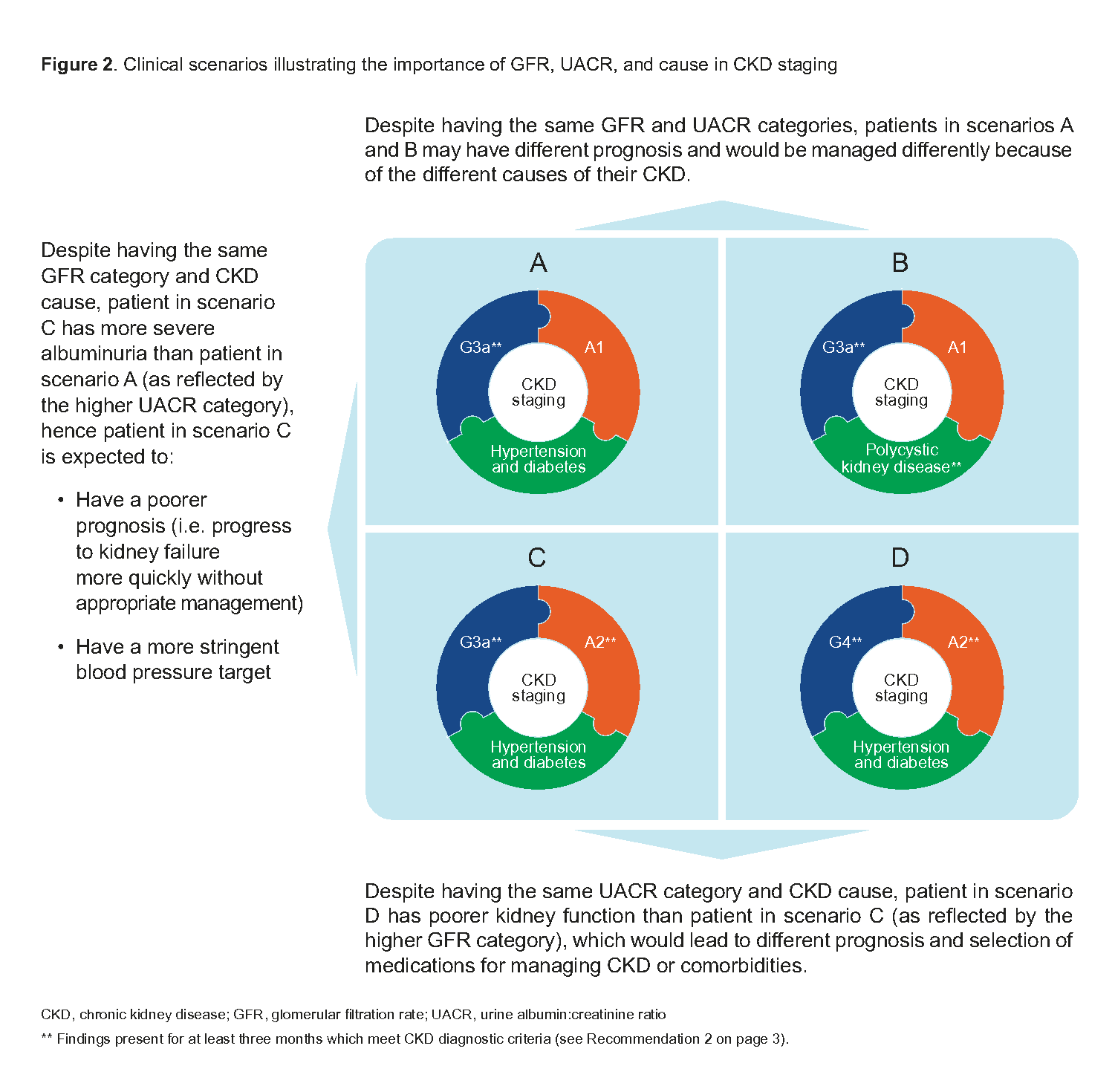
Figure 2. Clinical scenarios illustrating the importance of GFR, UACR, and cause in CKD staging
Management, patient education, and follow-up for patients with CKD
Recommendation 4: For patients diagnosed with CKD, discuss the diagnosis and management options with the patient.
Once CKD is diagnosed and staged, appropriate management is critical to slow down or prevent progression of CKD to kidney failure or other complications. Management of CKD (including pharmacotherapy) will be the focus of a separate clinical guidance.
Patient education and involvement are widely accepted as integral parts of chronic disease management. Increased patient knowledge about CKD can improve health outcomes.20 Conversely, a patient’s lack of knowledge, passive attitude towards self-management, and insufficient patient-healthcare professional communication can be barriers to optimal CKD management.21 Therefore, it is important for healthcare professionals to engage patients with CKD in a discussion about their diagnosis and management options. Points to include when discussing CKD with patients should be tailored to the patient’s individual circumstances:
Explaining what CKD is, including current stage of CKD, health implications and likely prognosis.
Reassuring the patient that proper management can slow down the progression of CKD.
Explaining the possible cause(s) and risk factor(s) contributing to the patient’s CKD, and how these can be further assessed.
Discussing the management options with the patient, including emphasising the importance of managing modifiable cause(s) and risk factor(s), and optimising management of related comorbidities.
Explaining how medications can help the patient manage some of the cause(s) and risk factor(s), and the importance of adhering to the medications prescribed.
Explaining how the patient can actively participate in their own care (for example, attend regular follow-up visits and maintain a healthy lifestyle, including a balanced diet, physical activity, and smoking cessation).
Follow-up for patients at increased risk of but do not have CKD
Recommendation 5: For patients who do not have CKD but are at increased risk, monitor for CKD regularly.
Patients who are at increased risk but do not have CKD should still be followed up regularly. While all patients at increased risk of CKD should be followed up at least annually, closer monitoring may be indicated in some cases, for example when risk factors are poorly controlled.
Referral
Recommendation 6: Referral to a specialist could be made at any point.
Specialist referral could be considered at any point, and is usually indicated for patients who have CKD with:
GFR <30mL/min/1.73m2 (GFR categories G4 and G5)1,18,22,23
Persistent significant albuminuria [UACR category A3 (UACR >30 mg/mmol (>300 mg/g))]1,18,22
Hypertension refractory to optimised antihypertensive treatment1,18,22,23
Sustained decline in GFR of >5 mL/min/1.73m2 per year23
Persistent microscopic haematuria or an episode of gross haematuria
Known or suspected rare or genetic causes of CKD18,23
Known or suspected renal artery stenosis1,18,23
The choice of specialist depends on the reason for referral.
Expert group
Chairperson
Prof Chan Choong Meng, Nephrology (SGH)
Members
Dr Andrew Ang Teck Wee, Family Medicine, Eunos Polyclinic (SHP)
Adj Asst Prof Manohar Giliyar Bairy, Nephrology (TTSH)
Dr Daphne Gardner Tan Su-Lyn, Endocrinology (SGH)
Adj Asst Prof Pankaj Kumar Handa, General Medicine (TTSH)
Dr S Suraj Kumar, Family Medicine (Drs Bain and Partners)
Dr Titus Lau Wai Leong, Nephrology (NUH)
Dr Edwin Lim Boon Howe, Family Medicine (Lakeside Family Medicine Clinic)
Dr Lim Chee Kong, Family Medicine (NHGP)
Asst Prof Lin Weiqin, Cardiology (NUHCS)
Dr Low Lip Ping, Cardiology (Low Cardiology Clinic)
Dr Sharon Ngoh Hui Lee, Family Medicine (Ang Mo Kio Family Medicine Clinic)
Dr Sitoh Yih Yiow, Geriatric Medicine (Age-Link Specialist Clinic for Older Persons)
Dr Abel Soh Wah Ek, Endocrinology (Abel Soh Diabetes, Thyroid and Endocrine Clinic)
Dr Tan Seng Hoe, Nephrology (SH Tan Kidney and Medical Clinic)
Dr Cynthia Wong Sze Mun, Family Medicine (National University Polyclinics)

Related ACGs
Chronic kidney disease – delaying progression and reducing cardiovascular complications
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Chronic kidney disease – early detection. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2022. Available from: go.gov.sg/acg-chronic-kidney-disease-early-detection
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.