
Chronic kidney disease — delaying progression and reducing cardiovascular complications ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) highlights the importance of personalised management for patients with early-stage chronic kidney disease (CKD) to delay progression and reduce cardiovascular complications. The ACG offers evidence-based recommendations on optimising blood pressure and albuminuria, with considerations for management in the context of associated comorbid conditions. Principles of tailored lifestyle intervention, regular follow-up, and options for shared or multidisciplinary care are also discussed.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Personalise the management plan based on CKD stage, including underlying cause.
Optimise blood pressure control and albuminuria management with an ACE inhibitor or ARB, and titrate to maximum tolerated dose as needed.
Add an SGLT2 inhibitor to ACE inhibitor/ARB therapy for patients with CKD and persistent albuminuria, regardless of DM status.
Optimise management of CKD-related comorbidities.
Encourage and provide education on lifestyle intervention through shared decision-making
Regularly follow up all patients with CKD, with more frequent review for those at increased risk of disease progression.
Consider shared or multidisciplinary care depending on CKD progression and other clinical needs.
Download the ACG and reference in PDF
CKD – delaying progression and reducing cardiovascular complications (Oct 2023) [PDF]
CKD – delaying progression and reducing cardiovascular complications references (Oct 2023) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Chronic kidney disease (CKD) is a major public health problem worldwide.1, 2 Patients with CKD have increased risk of cardiovascular (CV) complications such as coronary artery disease, heart failure, arrhythmia, or sudden cardiac death.3 Furthermore, patients with commonly associated comorbidities such as hypertension, dyslipidaemia, or diabetes mellitus carry an even higher CV risk – underscoring the importance of optimised management of comorbidities and overall CV riskfor all patients.4
In Singapore, CKD prevalence among residents aged 18–74 years was 8.8% in 2019-2020.5 This is estimated to triple by 2035, with CKD stages G1-2 accounting for most cases.1 Locally, the number of people detected with CKD stages G1-2 had increased significantly during the last decade and their annual rate of decline in kidney function was also found to be higher compared to those in the later stages – highlighting the need for timely and effective management early. This ACG focuses on management of early-stage CKD to slow down disease progression and to reduce risk of renal and CV complications.
Overall approach to management of CKD
Recommendation 1: Personalise the management plan based on CKD stage, including underlying cause.
CKD staging is based on three main components: GFR, UACR, and cause(s) such as other renal structural abnormalities. Collectively, these quantitative (GFR and UACR) and qualitative (cause) components of CKD staging provide essential information to determine the patient’s prognosis and guide appropriate management.
For example, management of CKD may differ in patients with same GFR and albuminuria categories if the underlying cause is different. Similarly, the rate of CKD progression (i.e. the decline in GFR or worsening albuminuria),6, 7 risk of progression to end-stage renal disease (ESRD), and CV risk may differ depending on underlying causes or risk factors. Therefore, the assessment and management of underlying cause(s) and risk factor(s) is key to optimising and personalising each patient’s treatment. See the ACG “Chronic kidney disease – early detection” for more details. Figure 1 provides an overview of management principles for patients with early-stage CKD, based on relevant comorbidities.
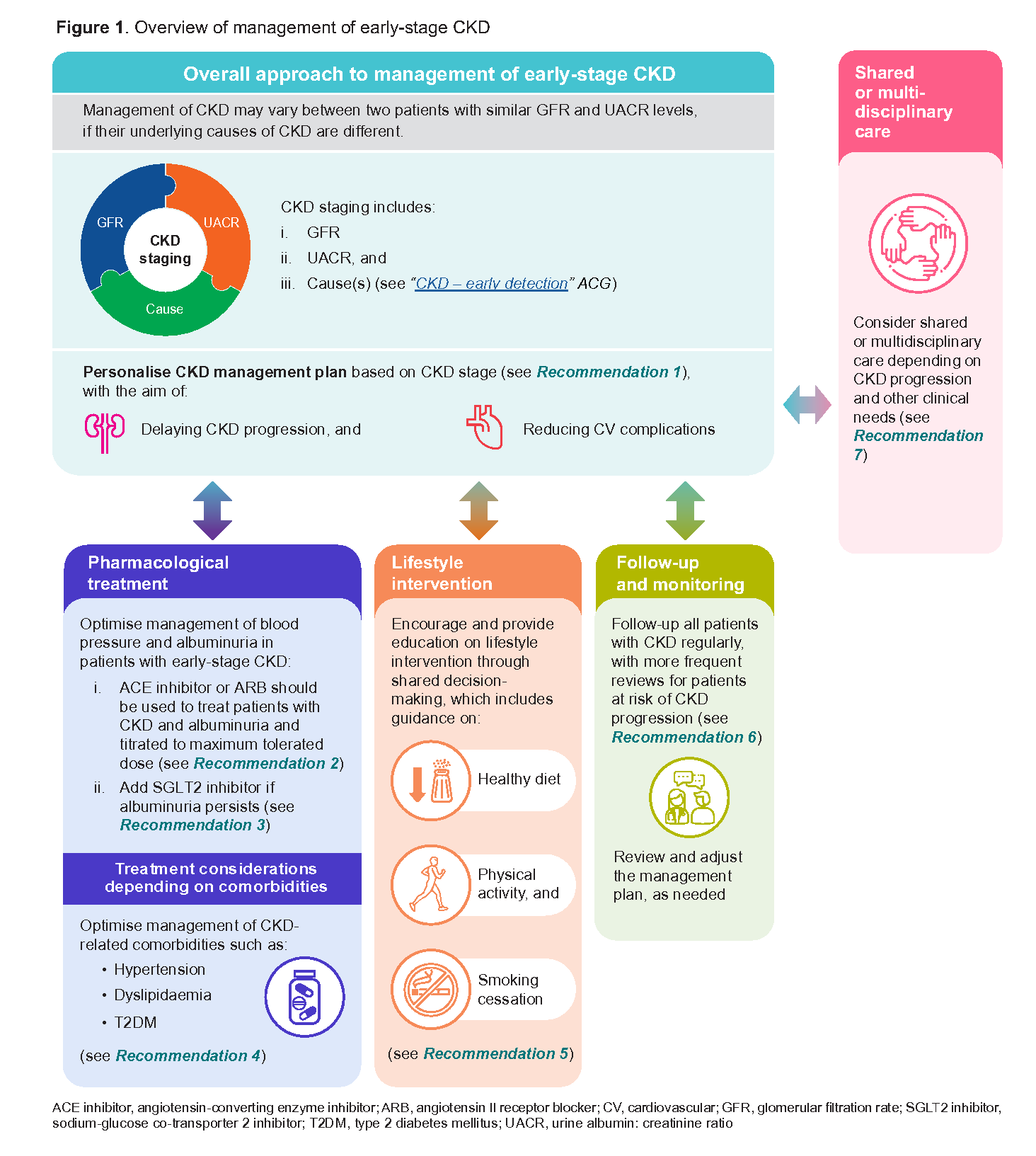
Figure 1. Overview of management of early-stage CKD
Pharmacological treatment
Recommendation 2: Optimise blood pressure control and albuminuria management with an ACE inhibitor or ARB, and titrate to maximum tolerated dose as needed.
Optimisation of blood pressure (BP) and albuminuria levels is a key management goal for patients with CKD to delay disease progression and reduce risk of CV complications.
Angiotensin-converting enzyme inhibitors (ACE inhibitors) and angiotensin II receptor blockers (ARBs) are the mainstay treatment options for patients with CKD and albuminuria, due to their beneficial effects in reducing the risk of major CV events and kidney failure.8, 9 The dose-dependent effects of these agents10-12 mean they can be started at low doses and up-titrated according to the patients' need for BP control, and their albuminuria levels. This approach reduces the risk of possible side effects associated with high doses and improves patient compliance (See Supplementary Table 1: Dosing information of ACE inhibitors and ARBs for patients with early-stage CKD for recommended starting and maximum doses). While initiation with an ACE inhibitor or ARB may be accompanied by a decline in GFR, treatment need not be discontinued if the GFR decline is less than 25% from baseline.13 However, if the eGFR decline is ≥25% from baseline, some of the follow-up actions can be found in Table 1 below.
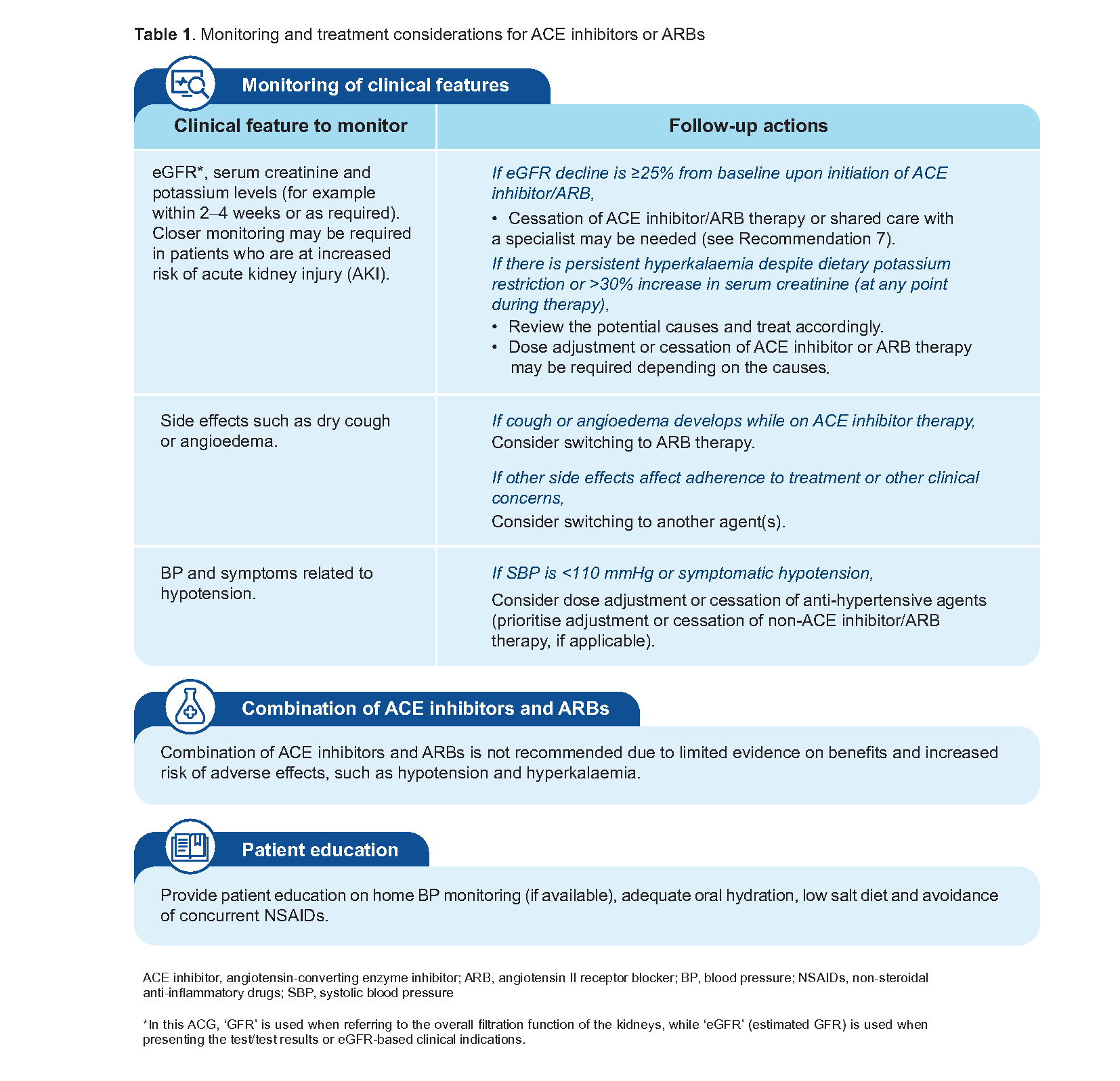
Table 1. Monitoring and treatment considerations for ACE inhibitors or ARBs
Recommendation 3: Add an SGLT2 inhibitor to ACE inhibitor/ARB therapy for patients with CKD and persistent albuminuria, regardless of DM status.
Sodium-glucose co-transporter 2 inhibitors (SGLT2 inhibitors) have been shown to reduce risk of worsening kidney function, onset of kidney failure or death from renal causes,14–16 with the added benefit of reducing the risk of CV events in patients with CKD.14, 15, 17 Notably, these renal outcomes were observed in patients with or without concomitant diabetes mellitus (DM).b
Important factors when considering SGLT2 inhibitors
For patients with CKD, the improvements in cardiorenal outcomes are independent of the glucose-lowering effects of an SGLT2 inhibitor. Guide the choice of medication and starting dose according to the patient’s eGFR level (See Table 2 below). Reported side effects from SGLT2 inhibitors include increased risk of recurrent urinary or genitourinary tract infections, and increased risk of euglycaemic ketoacidosis. Absence of contraindications and a careful assessment of the benefit-risk balance can inform the decision to add an SGLT2 inhibitor for patients with CKD and persistent albuminuria, in light of individual patient circumstances. When adding an SGLT2 inhibitor to ACE inhibitor/ARB therapy, measure serum creatinine within 4 weeks of initiation if there are concerns of a higher risk of AKI, such as in patients on concurrent diuretic therapy, or in elderly patients.
Notepad: GFR decline after initiation of SGLT2 inhibitors An acute eGFR decline may occur at 2–4 weeks after initiation of an SGLT2 inhibitor. In the absence of haemodynamic instability or an alternate cause of AKI, the initial rise in serum creatinine of up to 30% is not associated with long-term kidney function loss, and treatment with SGLT2 inhibitors should not be discontinued. |
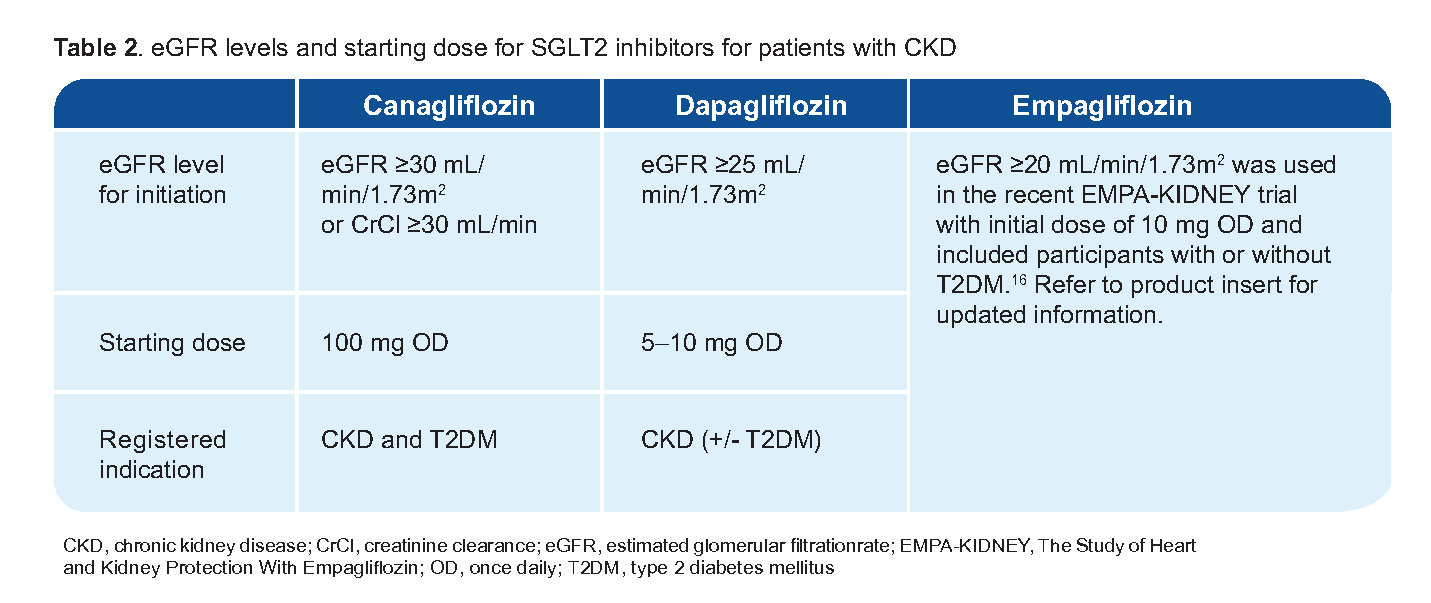
Table 2. eGFR levels and starting dose for SGLT2 inhibitors for patients with CKD
Notepad: Role of non-steroidal mineralocorticoid receptor antagonists (MRA) in patients with CKD and T2DM Finerenone (a non-steroidal MRA) was found to improve composite cardiovascular and renal outcomes in patients with CKD and T2DM who have albuminuria despite maximum tolerated dose of ACE inhibitors or ARBs.18 Currently, no head-to-head trials are available that compare finerenone and SGLT2 inhibitors. Indirect evidence from a network meta-analysis of trials evaluating finerenone and SGLT2 inhibitors with placebo favours SGLT2 inhibitors in reducing risk of kidney function progressionc and hospitalisation for heart failure.19 Limited evidence on the efficacy of finerenone compared to SGLT2 inhibitors, its relatively high cost and limited availability locally position finerenone only as a possible add-on therapy after SGLT2 inhibitor therapy in patients with CKD and T2DM who have persistent albuminuria. Monitoring of serum potassium (due to increased risk of hyperkalaemia) and renal function is recommended before and during treatment with finerenone.18,20,21 |
bSGLT2 inhibitors compared to placebo result in a 28-39% reduction in primary composite outcomes including doubling of serum creatinine level, ESRD, worsening kidney function (i.e. eGFR decline ≥50%), progression of kidney disease (i.e. eGFR decline ≥40%), onset of kidney failure, or death due to kidney diseases or CV causes, in patients with CKD with or without DM.14-16
cDefined as a composite of a sustained decrease of at least 40% in the eGFR from the baseline or a doubling of the serum creatinine level, kidney failure (a composite of end-stage kidney disease or sustained decrease in eGFR to <15 mL/min/1.73m2), or renal death.
Treatment considerations depending on comorbidities
Recommendation 4: Optimise management of CKD-related comorbidities.
A key management principle for early-stage CKD is to delay CKD progression and CV complications. As such, treatment plans should take into consideration the patient’s CKD stage, comorbidities, and the need to meet individualised treatment targets. The sections below focus on the major comorbid conditions associated with CKD in Singapore: hypertension, dyslipidaemia, and T2DM.
CKD and hypertension
Optimisation of BP control in patients with CKD is associated with a reduction in the risk of cardiorenal complications and CKD progression.22 A BP target of <130/80 mmHg can be used for most patients with CKD (with or without DM) to guide management. Less stringent BP targets (for example <140/90 mmHg) can be considered for patients with CKD; this is particularly important in patients for whom there is limited evidence on benefits of specific BP targets and increased risk of complications, such as older patients, those with high risk of frailty or falls, and those with multi-comorbidities.23, 24
ACE inhibitors or ARBs are still the preferred treatment options due to their effectiveness in reducing both BP and albuminuria. Other BP-lowering medications such as calcium channel blockers or diuretics may be considered as additional add-on therapy to ACE inhibitors/ARBs depending on patient factors, or the need to meet therapeutic targets.
CKD and dyslipidaemia
Management of dyslipidaemia (including hyperlipidaemia) is important to reduce overall CV risk and prevent associated complications, including for patients with early stages of CKD. Even though the association between dyslipidaemia and risk of CKD progression (i.e. risks of renal replacement therapy or death) is unclear,25 the association between reduction of LDL-cholesterol (LDL-C) levels and prevention of major atherosclerotic events in patients with CKD is established.26
Optimisation of lipid profile should be one of the key management goals for patients with CKD to reduce the risk of CV complications. Moderate-intensity statin therapy is the mainstay of treatment for reducing overall CV risk, with or without ezetimibe.27 Setting appropriate LDL-C targets should be based on overall CV risk and other patient-related factors (such a sage or frailty). An LDL-C target of <2.6 mmol/L can be used for most patients with CKD and hyperlipidaemia to guide management; more stringent LDL-C targets such as <1.8 mmol/L can be considered in patients with a history of atherosclerotic cardiovascular disease (ASCVD), comorbid DM or additional risk factors, if tolerated.
In addition to optimising medications based on eGFR, possible side effects (for example, increased risk of myopathy/myalgia with statins in patients with more advanced CKD), cost and management of potential drug-drug interactions should be taken into account when deciding on lipid-lowering therapy in patients with CKD.
CKD and T2DM
Patients with CKD and T2DM are at increased risk of ESRD, and cardiovascular morbidity and mortality.28, 29 Generally, an HbA1c target of ≤7% is recommended for most patients with early-stage CKD to reduce the incidence of albuminuria and help to slow down the progression of CKD.30 More flexible targets (e.g. <6.5% or <8.0%) can be considered depending on factors such as age, frailty, or multiple comorbidities. See the ACG “Type 2 diabetes mellitus – personalising management with non-insulin medications” for more details.
For patients with CKD and T2DM who require glycaemic control, metformin remains a good initial treatment choice for most patients with T2DM due to its long-standing effectiveness profile, coupled with generally affordable cost. This includes patients with early-stage CKD who requires glycaemic control although dose adjustments may be needed for patients with eGFR <60 mL/min/1.73m2.6 In addition to glucose-lowering effects, SGLT2 inhibitors have shown cardiorenal protective effects in patients with CKD with or without T2DM (See Recommendation 3) and are associated with weight reduction and low risk of hypoglycaemia, making this class of medications a preferred choice in patients with CKD (alone or as add-on to metformin).31 Other diabetes medications such as glucagon-like peptide-1 receptor agonists (GLP-1 RAs) or dipeptidyl peptidase-4 inhibitors can be used in patients with CKD and T2DM depending on patient factors and clinical needs. In addition to glucose-lowering effects, GLP-1 RAs have shown cardiorenal benefits in patients with CKD and T2DM,d although there is limited evidence for primary renal endpoints in patients with CKD.
dOverall, evidence for GLP-1 RA has shown a 21% reduction in composite kidney outcomes, 26% reduction in macroalbuminuria, 16% reduction in risk of nonfatal stroke, and 14% reduction in major CV events in patients with T2DM with or without CV disease.32, 33
Notepad: Important considerations for medication prescribing in patients with CKD
See Supplementary Table 2: Commonly prescribed medications that should be used with caution (e.g. dose adjustment or temporary cessation may be necessary) in patients with CKD for a non-exhaustive list of common medications that may require caution, with a focus on patients with early-stage CKD (for example, dose adjustment depending on eGFR or creatinine clearance). |
Lifestyle intervention
Recommendation 5: Encourage and provide education on lifestyle intervention through shared decision-making.
Lifestyle changes serve as an important complement to pharmacotherapy in patients with CKD, supporting prevention of disease progression and complications, as well as enhancing the quality of life among patients with CKD.35 Lifestyle intervention needs to be tailored to the individual (considering factors such as comorbidities, age, and social context) and patients should be involved when setting achievable and sustainable goals. For example, in discussing physical activity, patients can select types of exercise that are most manageable and likely to be well-tolerated, with clinician guidance.
Lifestyle changes for patients with CKD include increased physical activity, healthy diet, and smoking cessation. Beyond a healthy and balanced diet, certain nutrient-specific intakes can also be considered as part of lifestyle intervention – depending on CKD stage and clinical features. See Table 3 below for information.
Not all patients with CKD will need dietitian involvement. However, depending on availability of resources, referral to a dietitian could be useful for patients who have more complex dietary requirements or need further assistance to adopt dietary changes.
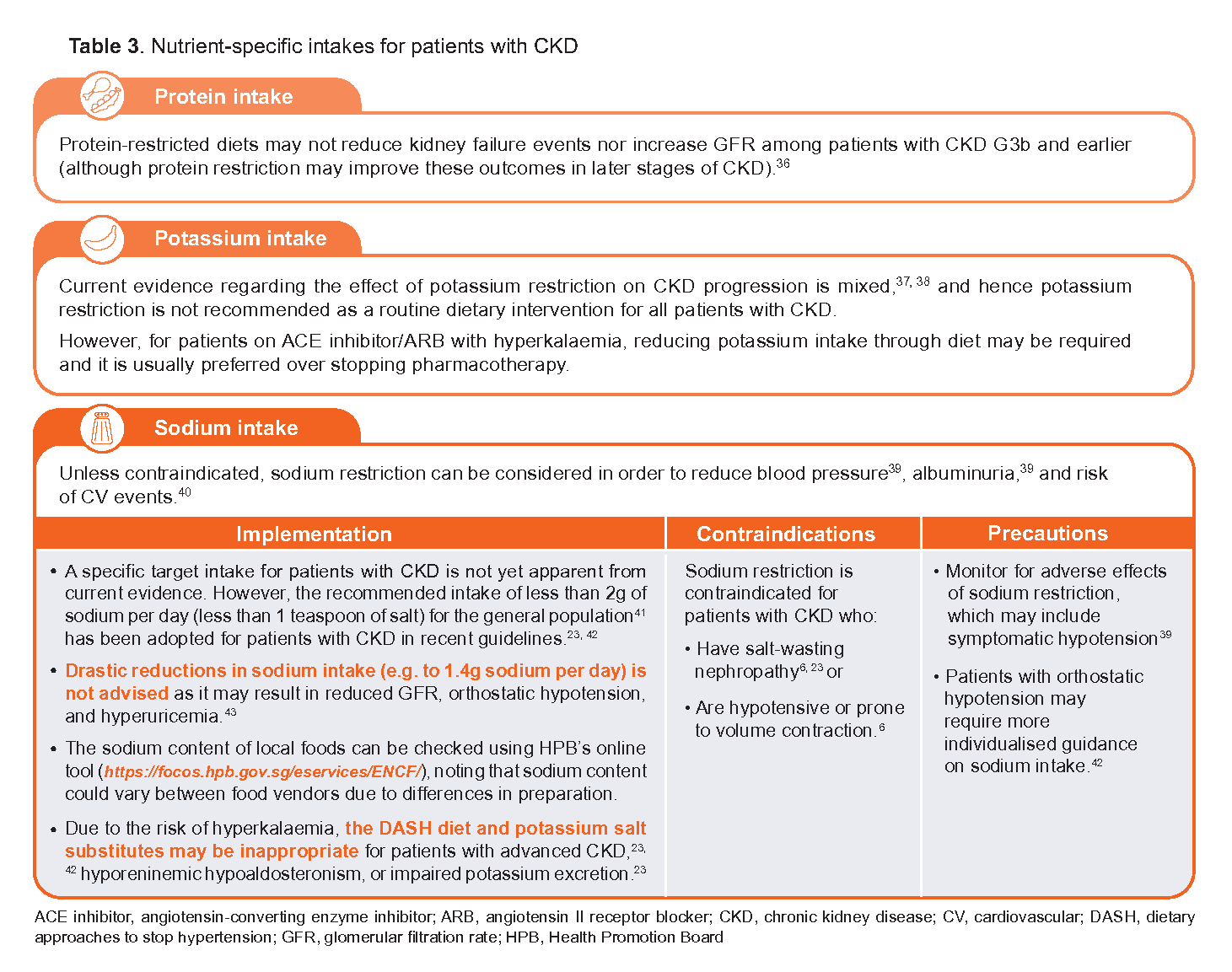
Table 3. Nutrient-specific intakes for patients with CKD
Follow-up and monitoring
Recommendation 6: Regularly follow up all patients with CKD, with more frequent review for those at increased risk of disease progression.
Rate of CKD progression may vary between patients depending on underlying causes or risk factors. Regular follow-up is recommended for all patients with CKD, including for those with early stages of CKD. More frequent review may be required for individuals at increased risk of CKD progression, such as for those with DM (especially when associated with high levels of albuminuria), with high blood pressure, or with increasing albuminuria and decreasing eGFR.44 Regular monitoring of eGFR and albuminuria is indicated for all patients with CKD at least annually. Table 4 below provides general guidance on frequency of review (based on expert opinion and practical considerations – no studies available) and monitoring parameters.
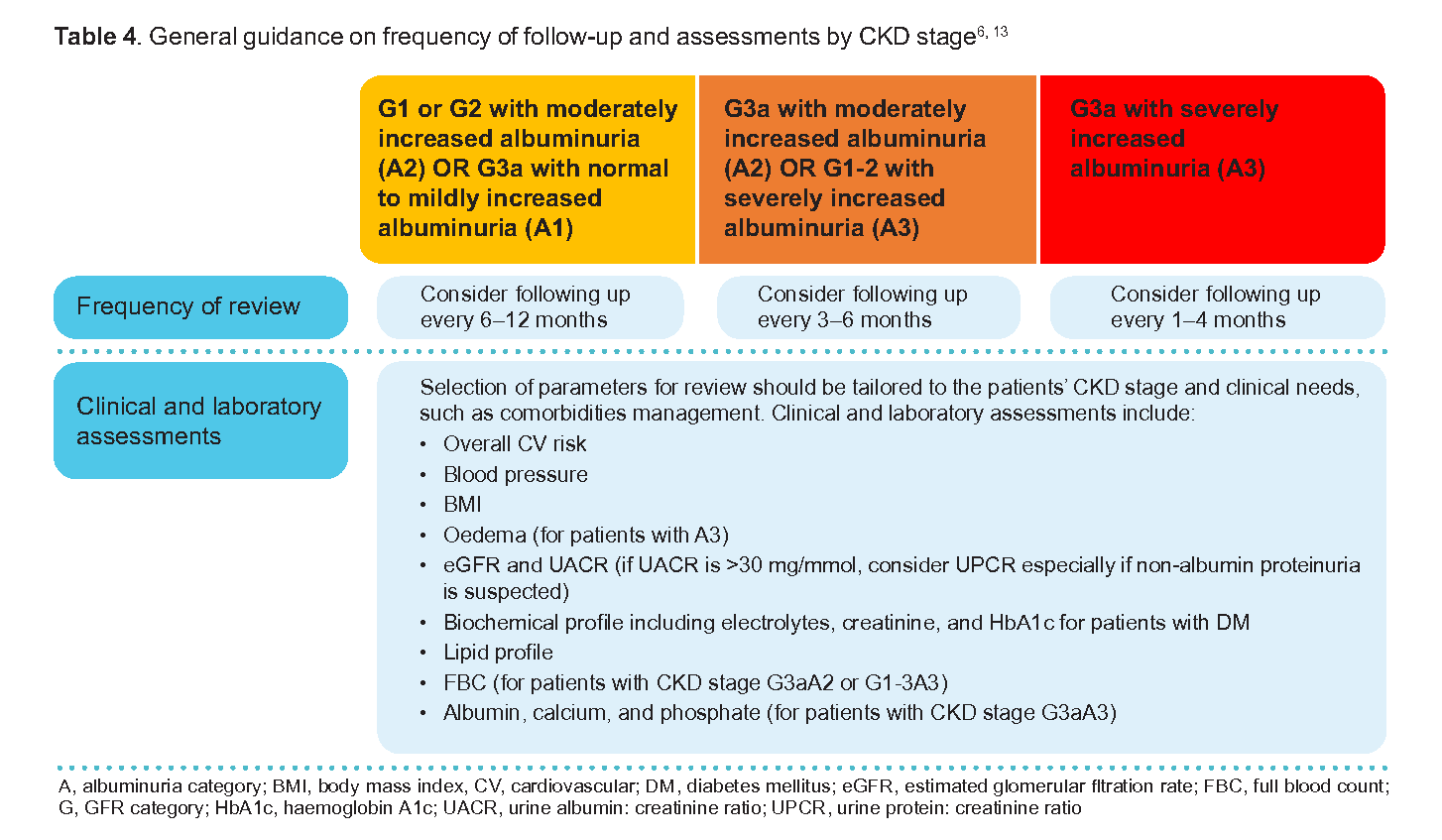
Table 4. General guidance on frequency of follow-up and assessments by CKD stage6, 13
Besides monitoring of clinical parameters, follow-up visits are an opportunity to check with patients on how they are coping with treatment, including factors that may be contributing to poor adherence (such as dosing regimen complexity, safety, tolerability, or cost concerns). Regular follow up should include review of lifestyle changes, reinforcing the importance of these to complement pharmacotherapy. Vaccination status should be reviewed regularly for all patients with CKD, prioritising vaccinations as per the Handbook on Adult Vaccination in Singapore 2020.45
Shared or multidisciplinary care
Recommendation 7: Consider shared or multidisciplinary care depending on CKD progression and other clinical needs.
Shared-care management between primary care providers and specialists may sometimes be necessary and are especially needed for patients at later stages of renal disease. This includes patients on conservative management, including older frail patients suitable for advance care planning, and those on dialysis or planned for transplant. Shared or multidisciplinary care for patients with CKD should be decided based on individual patient needs. It is usually indicated for people:
With later stages of CKD (e.g. CKD G3b-5)
In whom a primary cause of CKD is suspected (e.g. glomerulonephritis or autoimmune diseases)
With nephrotic syndrome
Needing further diagnostic assessment (e.g. kidney biopsy)
With rapidly progressive CKD (i.e. a ≥25% decline in eGFR from baseline or >5 mL/min/1.73m2/year decline) or high risk of kidney failure
With AKI
With anaemia secondary to CKD
With resistant hypertension or refractory hypertension suspected to be secondary to CKD
With multiple comorbidities, such as heart failure or rheumatological conditions
With persistent hyperkalaemia
With bone disease or abnormal calcium metabolism
Supplementary materials
Expert group
Chairperson
Prof Chan Choong Meng, Nephrology (SGH)
Members
Dr Andrew Ang Teck Wee, Family Medicine, Eunos Polyclinic (SHP)
Adj Asst Prof Manohar Giliyar Bairy, Nephrology (TTSH)
Dr Daphne Gardner Tan Su-Lyn, Endocrinology (SGH)
Adj Asst Prof Pankaj Kumar Handa, General Medicine (TTSH)
Dr S Suraj Kumar, Family Medicine (Drs Bain and Partners)
Dr Titus Lau Wai Leong, Nephrology (NUH)
Dr Edwin Lim Boon Howe, Family Medicine (Lakeside Family Medicine Clinic)
Dr Lim Chee Kong, Family Medicine (NHGP)
Asst Prof Lin Weiqin, Cardiology (NUHCS)
Dr Low Lip Ping, Cardiology (Low Cardiology Clinic)
Dr Sharon Ngoh Hui Lee, Family Medicine (Ang Mo Kio Family Medicine Clinic)
Dr Sitoh Yih Yiow, Geriatric Medicine (Age-Link Specialist Clinic for Older Persons)
Dr Abel Soh Wah Ek, Endocrinology (Abel Soh Diabetes, Thyroid and Endocrine Clinic)
Dr Tan Seng Hoe, Nephrology (SH Tan Kidney and Medical Clinic)
Dr Cynthia Wong Sze Mun, Family Medicine (National University Polyclinics)

Related ACGs
Chronic kidney disease – early detection
Type 2 diabetes mellitus – personalising management with non-insulin medications
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Chronic kidney disease – delaying progression and reducing cardiovascular complications. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2023. Available from:go.gov.sg/acg-ckd-management
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.