
Chronic obstructive pulmonary disease – diagnosis and management ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) highlights the diagnostic approach for chronic obstructive pulmonary disease (COPD), including differential diagnosis with relevant conditions such as asthma. Diagnostic recommendations are complemented by a supplementary guide on how to interpret spirometry reports, as well as a list of spirometry sites in Singapore that are open to external referrals. The ACG also covers non-pharmacological and pharmacological management options for patients with stable COPD, with a focus on the importance of smoking cessation, and appropriate use of bronchodilators or inhaled corticosteroids.
First published in 2018, guideline on COPD has been updated in 2024 to consolidate diagnosis and management recommendations in one ACG, incorporating the latest evidence where relevant. In December 2024, links have been added to the ACG for the new patient education aids on the use of inhalers in COPD and spirometry testing.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Suspect chronic obstructive pulmonary disease (COPD) in any patient with at least one relevant symptom and risk factor.
Diagnose COPD in patients with relevant symptoms and risk factors who have airflow obstruction detected via spirometry (post‐bronchodilator FEV1/FVC <0.7).
Regularly assess symptoms and exacerbation risk for all patients with COPD.
Explain the benefits of smoking cessation on COPD progression and strongly encourage those who smoke to quit.
Start bronchodilator treatment, preferably a long-acting bronchodilator, for patients with infrequent or less intense symptoms and lower risk of exacerbation.
Start dual bronchodilator therapy with long-acting muscarinic antagonist (LAMA) + long-acting beta2-agonist (LABA) for patients with frequent or intense COPD symptoms, or a higher risk of exacerbations.
Consider triple therapy with LAMA + LABA + inhaled corticosteroid (ICS) for patients with frequent COPD exacerbations and eosinophilia.
Assess inhaler technique and medication adherence at every visit and provide support to ensure optimal benefits from medications.
Download the ACG and references in PDF
Chronic obstructive pulmonary disease – diagnosis and management (Dec 2024)
Chronic obstructive pulmonary disease – diagnosis and management references (Dec 2024) [PDF]
Supplementary guide on open-access spirometry in Singapore (June 2024) [PDF]
Supplementary guide on interpreting spirometry reports (June 2024) [PDF]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
COPD is a heterogenous lung condition characterised by chronic respiratory symptoms due to abnormalities of the airways or alveoli that cause persistent, often progressive, airflow obstruction.1 Globally, in 2019, COPD is the third most common cause of death and an increasingly important contributor to morbidity due to an ageing population, urbanisation, and persistence of risk factors.2, 3 In Singapore, COPD is estimated to be the tenth highest cause of death and seventeenth highest cause of disability-adjusted life years.4 Locally, COPD contributes to chronic respiratory disease-related hospitalisations and emergency department visits, and was estimated to have an annual societal cost of SGD$3,304 per capita in 2022.a 5 COPD exacerbations account for the greatest proportion of the total COPD burden on the healthcare system.6
Although COPD is not fully reversible, once diagnosed it can be effectively managed in primary care. Primary care plays an important role in detecting new cases in the community to generate early intervention opportunities, including counselling to quit smoking, and initiating pharmacotherapy to reduce symptoms and future risk of exacerbations.1 Research and treatment options for COPD continue to evolve, therefore up-to-date guidance on accurate diagnosis and optimal management can support clinical improvements in COPD care, including better quality of life for patients.
aAdjusted from 2009 to 2022 $SGD using the Singapore healthcare consumer price index.
Establishing a diagnosis of COPD
Recommendation 1: Suspect COPD in any patient with at least one relevant symptom and risk factor.
A thorough history-taking is important for establishing COPD diagnosis and should include:
Past medical history (for example, early life events, respiratory disease, respiratory infections in childhood, history of exacerbations or previous hospitalisations for respiratory disorder), and existing comorbidities;
Family history of COPD or other chronic respiratory disease; and
COPD risk factors and symptoms (see Figure 1).
The index of suspicion for COPD should be raised when the patient presents with chronic unexplained dyspnoea or reduced effort tolerance that tends to worsen over time, chronic cough with or without sputum production, or inspiratory/expiratory wheezing. Symptoms may vary from day-to-day and can be under-reported by patients, who often attribute them to ageing, smoker’s cough, or other disorders.
COPD risk factors include tobacco smoking, environmental or occupational sources of lung irritants, history of severe childhood infections, pulmonary tuberculosis, abnormal lung development, and age 40 or more years. Rare risk factors of COPD include genetic components, such as alpha-1 antitrypsin deficiency. In the absence of risk factors, COPD is unlikely. However, exercise clinical judgement in light of individual patient circumstances, and consider spirometry testing if suspicion of COPD remains high after exploring differential diagnoses (see section “Differential diagnoses of COPD”).
Figure 1 provides an overview of the diagnosis and management of COPD, including COPD symptoms and risk factors commonly available from history-taking.
Recommendation 2: Diagnose COPD in patients with relevant symptoms and risk factors who have airflow obstruction detected via spirometry (post-bronchodilator FEV1 /FVC <0.7).
There are three key factors required for COPD diagnosis (see Figure 2):
COPD risk factor(s);
COPD symptom(s); and
Concordant spirometry findings.
Ensuring that all three components are met prior to diagnosis increases the ability to differentiate COPD from other similar respiratory conditions, including asthma.
Once COPD is suspected based on the presence of relevant risk factors and symptoms, spirometry is required for diagnosis for all patients, except for those with active respiratory infectious disease like tuberculosis, heart disease, or other contraindications to the test.7 COPD is characterised by persistent, and often progressive airflow limitation, which is defined as spirometry value of FEV1 /FVC <0.70. Post-bronchodilator FEV1 /FVC <0.70 in patients with pertinent risk factors and symptoms confirms COPD.1,8 Spirometry findings are to be interpreted in the overall context of patient presentation, including symptoms and risk factors. For example, the fixed FEV1 /FVC cut-off alone might result in overdiagnosis of COPD in the elderly. Refer to the supplementary guide on “Interpreting spirometry reports” for examples that elucidate the importance of assessing a history of symptoms and risk factors.
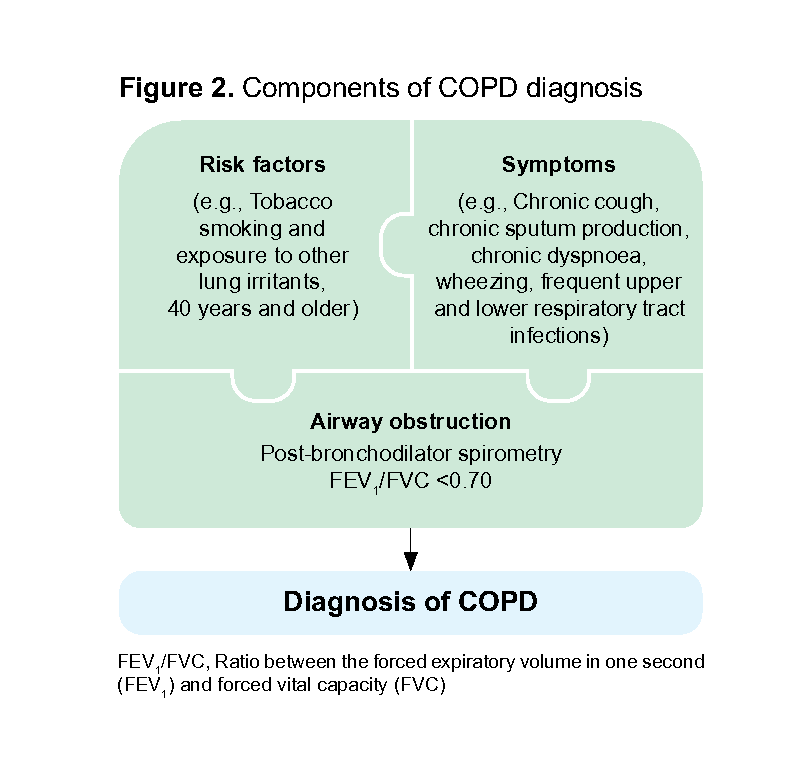
Figure 2. Components of COPD diagnosis
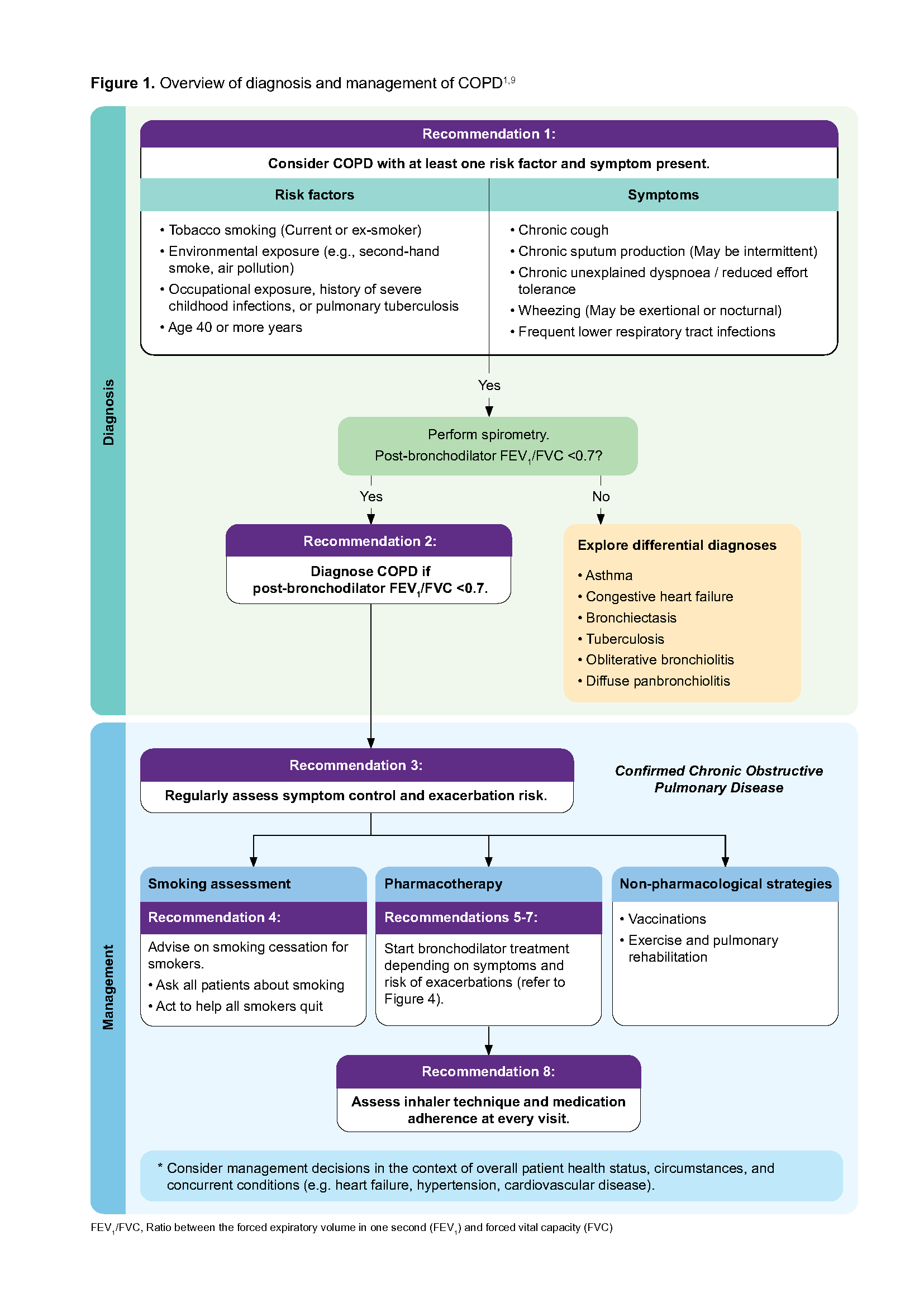
Figure 1. Overview of diagnosis and management of COPD1,9
Click here for larger version of the image
Notepad: Practice point on spirometry
|
Differential diagnoses of COPD
Due to similarities in symptoms, these differential diagnoses should be considered when assessing a patient presenting with symptoms and risk factors suggestive of COPD.1
Asthma
Congestive heart failure
Bronchiectasis
Tuberculosis
Obliterative bronchiolitis
Diffuse panbronchiolitis
Further investigations such as chest X-ray forms part of the initial assessment of a patient presenting with respiratory symptoms suggestive of COPD, for assessing comorbidities, or excluding alternative diagnoses.1
COPD and asthma
The clinical presentations of COPD and asthma can be similar, and differentiating between the two conditions is necessary to provide the appropriate treatment. COPD treatment is centred on using inhaled bronchodilators (beta2-agonists and antimuscarinics), and inhaled corticosteroids play a targeted role.1 In contrast, controller therapy in asthma is anchored on inhaled corticosteroids.12
In most cases, a detailed history of symptoms and risk factors, and objective spirometry test results can separate COPD from asthma (see Table 1). Knowing if a patient has more asthma or COPD features increases diagnostic accuracy.12
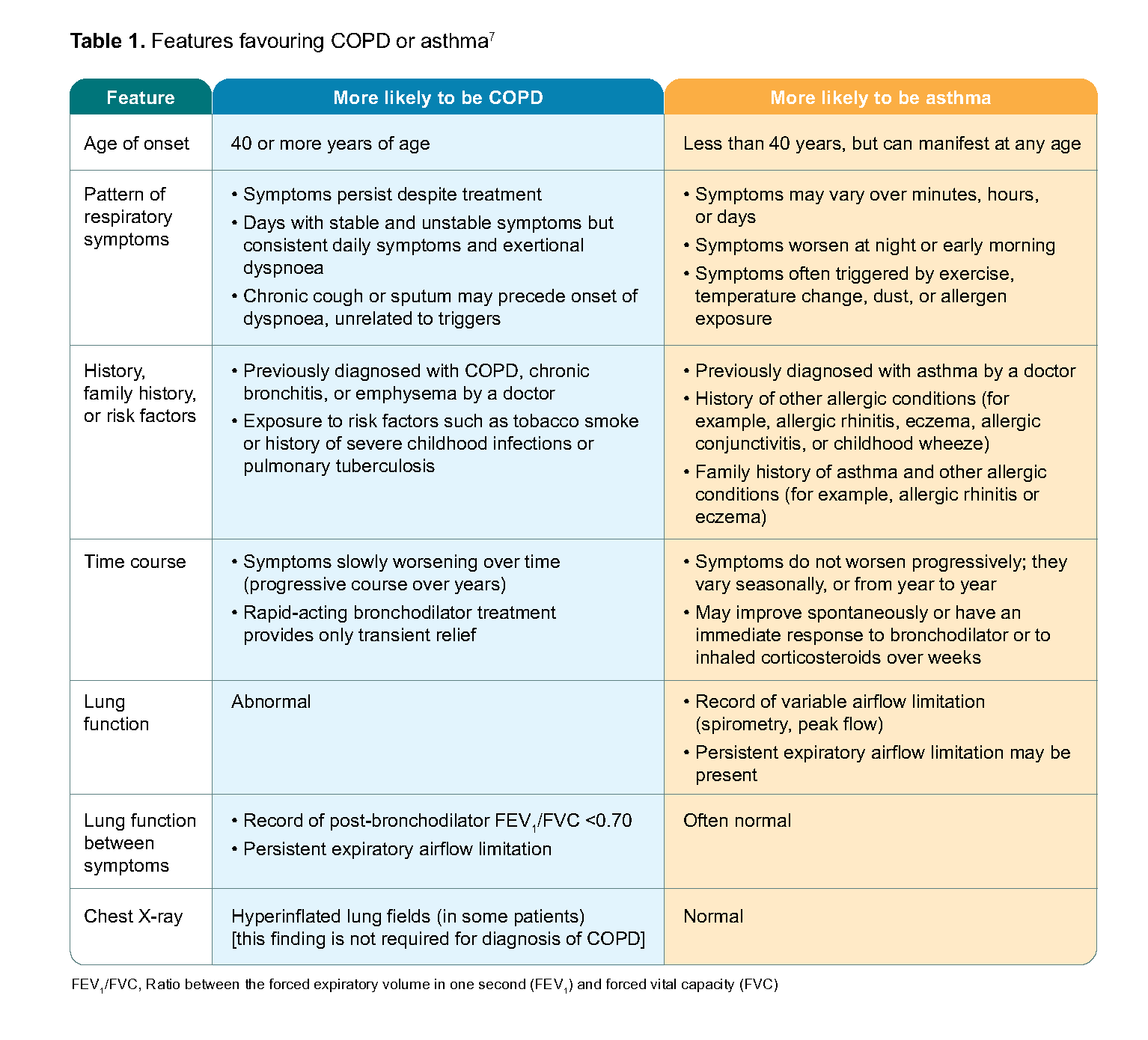
Table 1. Features favouring COPD or asthma7
In some cases, it may be challenging to distinguish between COPD and asthma. Some patients may have features of both asthma and COPD which is characterised by persistent airflow limitation with clinical features that are consistent with both conditions.1,12
If a concurrent diagnosis of asthma is suspected, the pharmacotherapy options should follow asthma guidelines.1 If the distinction between COPD and asthma is unclear, consider a trial of asthma treatment first. For information on asthma assessment and management click here to see the ACG “Asthma – optimising long-term management with inhaled corticosteroid”.
Initial and ongoing COPD assessment
Recommendation 3: Regularly assess symptoms and exacerbation risk for all patients with COPD.
Regular assessment for patients with COPD13 includes evaluating their current symptoms by checking:
Frequency and intensity of symptoms;
Use of reliever medications; and
Impact on activities of daily living.
Symptoms assessment should be conducted at least yearly, and more frequently for patients who are more symptomatic, have more frequent exacerbations, or have recent escalation in treatment. Questionnaires are available to guide COPD symptoms assessment. For example, the COPD Assessment Test (CAT)14 is a validated 8-item questionnaire that was developed (translated and validated for use in many languages) to assess the health status in patients with COPD. The Modified British Medical Research Council (mMRC) dyspnoea scale,15 although simple to use, was developed to measure breathlessness, which may not account for the other symptoms of COPD.
In addition to symptoms, the history of exacerbations due to COPD informs the patient’s risk of future exacerbations.16 Patients with COPD are at increased risk of future exacerbations if they had:
Two or more exacerbations requiring antibiotics or steroids in the previous year; or
One leading to hospitalisation in the previous year.1
Notepad: Acute exacerbation of COPD A COPD exacerbation is defined as an event characterised by dyspnoea and/or cough and sputum that worsens in <14 days which may be accompanied by tachypnoea and/or tachycardia and is often associated with increased local and systemic inflammation caused by infection, pollution, or other insults to the airways.9 Differential diagnoses that may present similarly should be excluded, such as pneumonia, congestive heart failure, or pulmonary embolism.1 Treatment of COPD acute exacerbations should be initiated with short-acting inhaled beta2-agonists with or without antimuscarinics. Consider additional therapy with systemic corticosteroids or antibiotics where indicated.1 those who fail to respond to initial treatment.1 Patients who should be considered for treatment in the tertiary setting include those with severe signs and symptoms, unstable vitals (for example, respiratory rate ≥24 breaths/minute, heart rate ≥95 beats/minute, resting oxygen saturation <92% on room air and/or change >3% [when known]), serious comorbidities, or After the episode, check blood eosinophils levels to guide the adjustment of maintenance therapy as necessary (see Figure 4). Additionally, provide patients with an exacerbation action plan, or discuss and agree changes to the existing one. |
Management of stable COPD
The main goals in managing stable COPD are reducing symptoms and risk of future exacerbations.1 Both pharmacological and non-pharmacological measures are important to achieve COPD management goals, and reduce associated morbidity and mortality.
Choice of COPD long-term treatment is based on individualised symptom and exacerbation risk assessment. A stepwise approach to add or change inhaler medication classes is recommended for patients with persistent symptoms or further exacerbations.
Patients with COPD often coexist with other comorbidities such as cardiovascular diseases, heart failure, and hypertension.1 Although the presence of comorbidities generally does not alter COPD treatment, clinicians should consider management decisions in the context of overall patient health status, circumstances, and concurrent conditions.
Smoking cessation
Recommendation 4: Explain the benefits of smoking cessation on COPD progression and strongly encourage those who smoke to quit.
Smoking is the commonest risk factor for COPD and smoking cessation is the single most effective intervention for managing the disease. Stopping smoking reduces decline in lung function (see Figure 3)17 and mortality. Check smoking status in every patient with COPD and encourage those who smoke to quit smoking. Studies have shown that even brief clinician advice—less than three minutes—produces long-term smoking abstinence rates of 13.4%.18
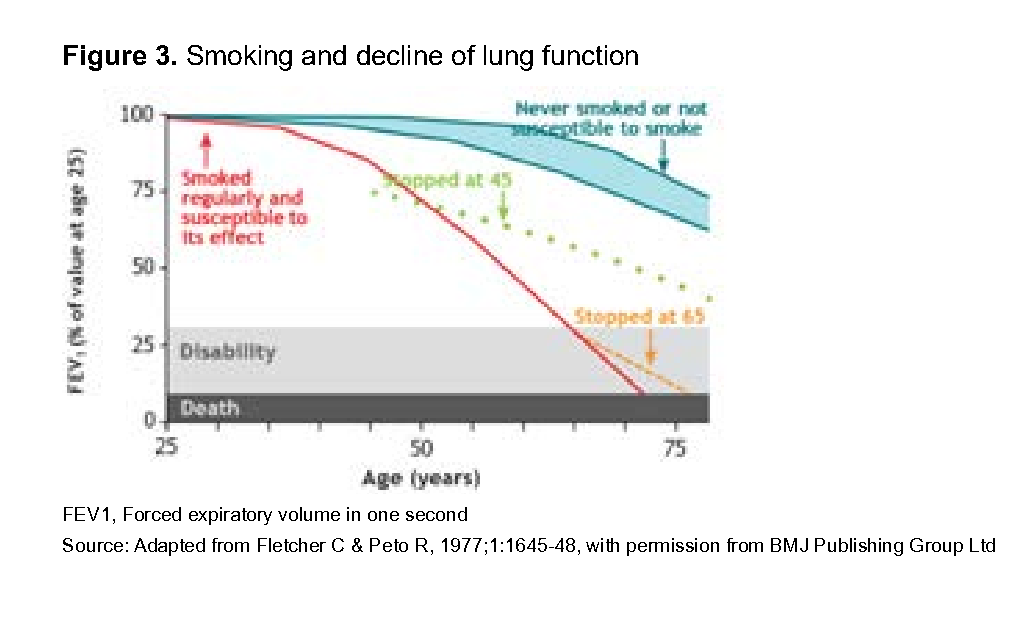
Figure 3. Smoking and decline of lung function
Patient resources on smoking cessation, including cessation programmes, can be found at HealthHub’s I Quit Programme webpage. Click here to find out more.
Notepad: Smoking cessation – the 2As Routinely use the 2As approach as a brief opportunistic first-line intervention during consultations.19 Ask all patients about smoking Act to help all smokers quit20 Consider a more comprehensive approach to smoking cessation if time permits, or refer for smoking cessation services. Click here for the HealthierSG care protocol on smoking cessation. |
Pharmacotherapy
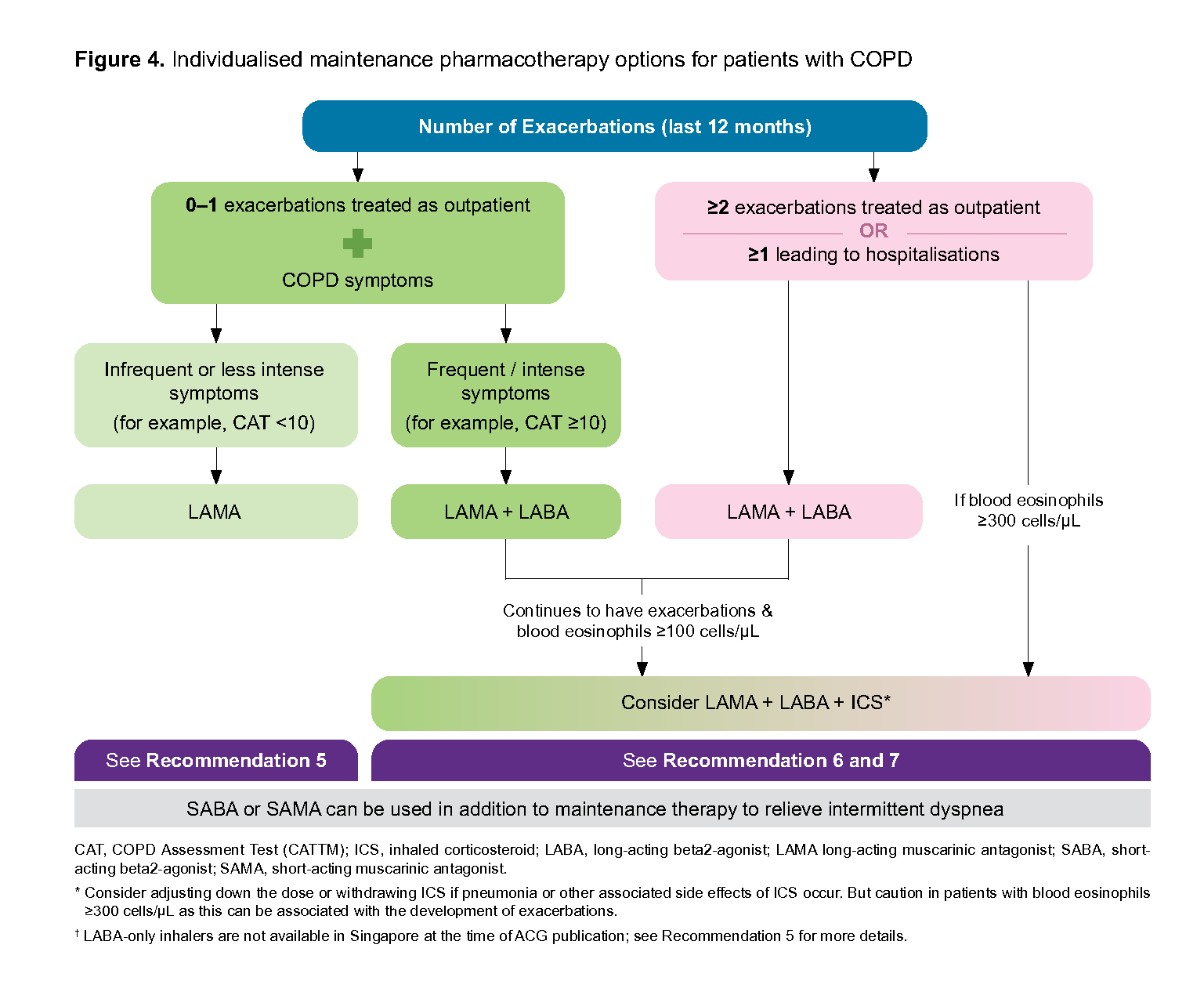
Figure 4. Individualised maintenance pharmacotherapy options for patients with COPD
Recommendation 5: Start bronchodilator treatment, preferably a long-acting bronchodilator, for patients with infrequent or less intense symptoms and lower risk of exacerbations.
Inhaled bronchodilators relax bronchial smooth muscles, relieving bronchospasm and dyspnoea. They are central in preventing or reducing COPD symptoms.1 They comprise beta2-agonists and antimuscarinics, and can be short- or long-acting.
Long-acting bronchodilators are preferred as the initial maintenance therapy. Regular use of long-acting bronchodilators improves lung function, dyspnoea, health status, and reduces exacerbation rates.1 Long-acting muscarinic antagonists (LAMAs) are usually preferred over long-acting beta2-agonists (LABAs), with evidence suggesting some reduction in exacerbation rates with LAMAs compared to LABAs.21 At the time of ACG publication, there are no LABA-only inhalers available in Singapore.
Short-acting bronchodilators alone can be considered in patients with very occasional dyspnoea.1 Short-acting beta2-agonist (SABA) or short-acting muscarinic antagonist (SAMA) can be used as needed to relieve intermittent dyspnoea in all COPD patients.
Recommendation 6: Start dual bronchodilator therapy with LAMA + LABA for patients with frequent or intense COPD symptoms, or a higher risk of exacerbations.
For patients with frequent or intense COPD symptoms (for example, CAT ≥10) or at a higher risk of future exacerbations (for example, have had at least two COPD exacerbations or one COPD exacerbation requiring hospitalisation in the past year), LAMA + LABA combination has a greater ability to reduce COPD exacerbations compared to monotherapy with a long-acting bronchodilator. 1,22
Recommendation 7: Consider triple therapy with LAMA + LABA + ICS for patients with frequent COPD exacerbations and eosinophilia.
Initial treatment with triple therapy (LAMA + LABA + ICS)
Initiating treatment with triple therapy (LAMA + LABA + inhaled corticosteroid [ICS]) could be considered if the patient is assessed to be at a higher risk for exacerbations (for example, two or more exacerbations of COPD requiring antibiotics or steroids per year or history of hospitalisation(s) for COPD) and have blood eosinophils ≥300 cells/µL. Although there is limited evidence for initiating treatment with triple therapy, this is a practical recommendation based on inferences from randomised controlled trials which have shown that increased eosinophil counts were associated with increased COPD exacerbation rates in patients already on treatment.1,23-25
Other factors which would favour the use of ICS include the history of asthma. ICS therapy plays a role for patients with features of both asthma and COPD.1 Consider specialist referral for this group of patients.
Escalation to triple therapy (LAMA + LABA + ICS)
For patients who continue to have frequent exacerbations on LAMA + LABA therapy and have elevated blood eosinophil levels (blood eosinophils ≥100 cells/µL), addition of inhaled corticosteroid (ICS) to LAMA + LABA therapy should be considered.1 It has been shown to improve lung function, patient reported outcomes, and reduce exacerbations when compared to dual long-acting bronchodilator therapy.23,24,26
Side effects and complications associated with the use of ICS include oral thrush, hoarse voice, skin bruising, and pneumonia. Regular use of ICS increases the risk of pneumonia,27 especially when using high dose/high-potency ICS, or in certain subgroups of patients with COPD, such as patients with severe disease, smokers, aged 55 or more years, BMI <25 kg/m2, and a previous history of exacerbation or pneumonia. As such, ICS is not recommended for patients with recurrent pneumonia events, blood eosinophils <100 cells/µL, or history of mycobacterial infections.1
Blood eosinophil levels have been found to have reasonable repeatability during stable disease (at least 14 days after an exacerbation).28 Clinicians are reminded to do a full blood count to check blood eosinophil levels before starting ICS in COPD patients – this can be done after an episode of exacerbation (see Figure 4).
Notepad: Alternatives to Single-Inhaler Triple Therapy (SITT) If combination treatment involving LAMA + LABA + ICS is required for the patient, prescribing single-inhaler triple therapy (SITT), which combines all three drugs into a single inhaler, will simplify the dosing regimen for patients, and avoid confusion in using different types of inhaler devices. Prescribing more than one device or inhaler to achieve the desired triple therapy effect is an alternative option. Clinicians should engage in a tailored discussion with the patient about their management goals to determine the most appropriate treatment for them – including patient affordability factors. |
Inhaled bronchodilators and ICS registered in Singapore for the management of COPD are listed in Figure 5.
Other medications for management of COPD
Methylxanthines such as theophylline, mucolytics, and macrolides are not within the scope of this clinical guideline. Overall, they should be reserved as adjuncts to inhaled therapy.
Assessment of inhaler technique
Recommendation 8: Assess inhaler technique and medication adherence at every visit and provide support to ensure optimal benefits from medications.
Incorrect inhaler technique is common. Before stepping up therapy, assess whether patients are adhering to their recommended treatment and using their inhalers correctly. Provide patients with sufficient information and demonstration on correct inhaler use for optimal benefits. Click here for more related information (for example, inhaler technique videos).
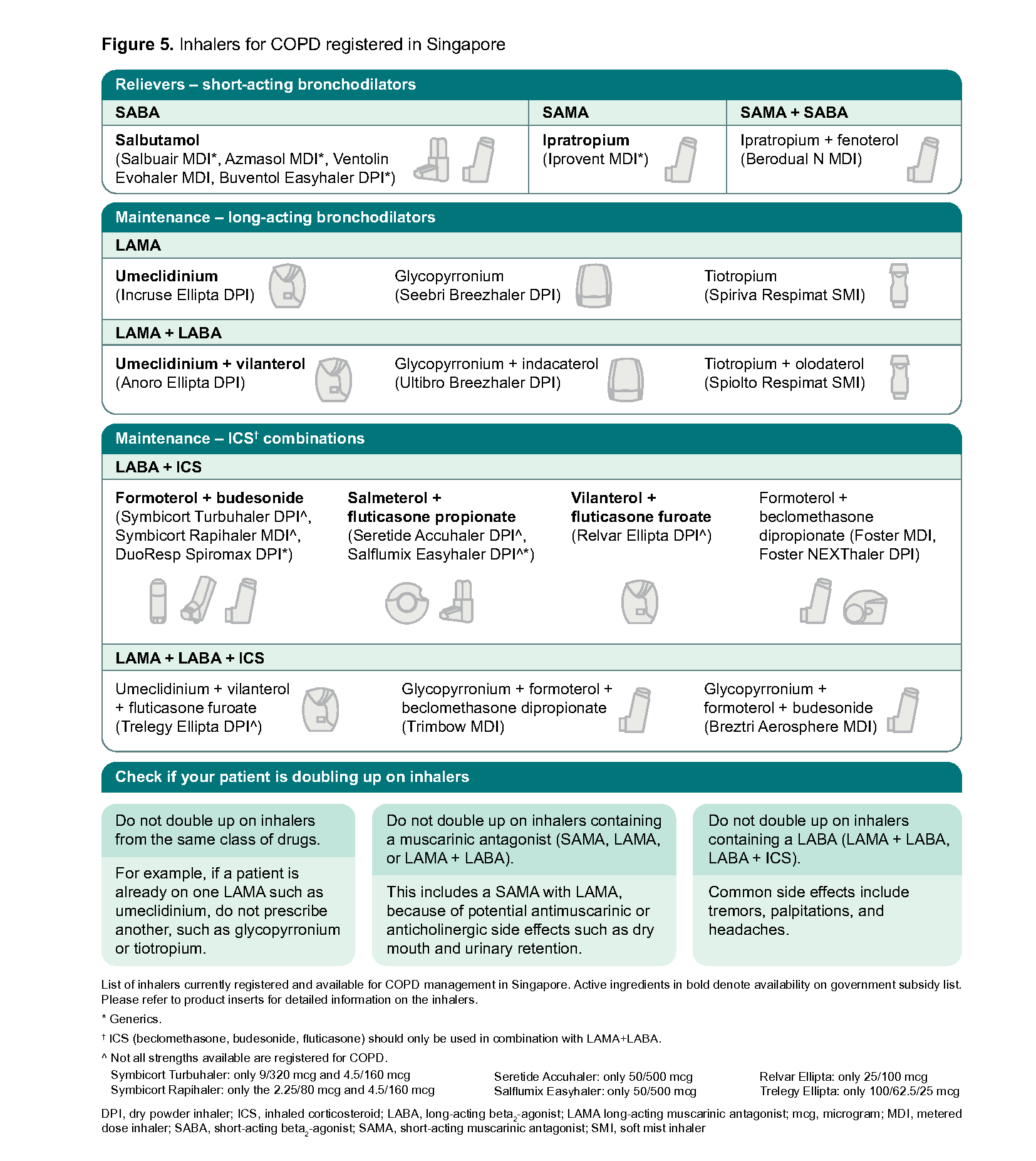
Figure 5. Inhalers for COPD registered in Singapore
Click here for larger version of the image
Non-pharmacological strategies for the management of COPD |
|---|
Vaccinations that lower risk of respiratory tract infections Both influenza and pneumococcal vaccinations decrease lower respiratory tract infections.1 Offer patients with COPD both these vaccinations in alignment with the National Adult Immunisation Schedule.29 Patients who have not received vaccination against Pertussis should also receive the Tdap vaccine.1,30 |
Exercise and pulmonary rehabilitation Reduced physical activity is common in patients with COPD and results in poorer outcomes. Encourage patients to exercise regularly. Simple aerobic exercises such as walking three to four times a week for 20 to 30 minutes is beneficial. Coupling this with strengthening exercises such as repeated movements with weights has additional benefits.31 Pulmonary rehabilitation programmes are available in hospitals. They improve symptoms, quality of life, and exercise tolerance. A key component of pulmonary rehabilitation programmes is structured exercise training, recommended twice a week for six to eight weeks. Education and self-management strategies are also incorporated to target behavioural change, with the aim of improving patient well-being and long- term adherence to health-enhancing behaviours.1 |
Long-Term Oxygen Therapy (LTOT) COPD patients managed in the primary care setting may be on LTOT. It is indicated when1:
If prescribed, LTOT should achieve SaO2 ≥90%, and clinicians should review their patient’s condition and SaO2 at room air every 60 to 90 days to adjust the oxygen therapy accordingly.1 |
Nutritional Support In patients with COPD, weight loss and malnutrition develop as the disease progresses and indicates a poor prognosis. Malnutrition in COPD is associated with impaired lung function, poor exercise tolerance, worsened quality of life, increased hospitalisations and mortality.1 As such, nutritional repletion (including protein supplementation) plays an important role for such patients, and should be coupled with optimisation of lung function, regular exercise, and oxygenation if needed.1 |
Notepad: Specialist referral Indications for referring to a specialist include diagnostic uncertainty (such as patients with features of both asthma and COPD), unusual symptoms (such as haemoptysis), severe COPD, onset of cor pulmonale, bullous lung disease, COPD <40 years of age, and frequent chest infections.32 |
Notepad: Palliative and supportive care Palliative care aims to optimise quality of life at all stages of disease by achieving symptom control and maximising function. In the context of palliative or supportive care for patients with COPD, treatment options to reduce dyspnoea include opioids,33 pulmonary rehabilitation,34 patient self-management education for breathing techniques,1 neuromuscular electrical stimulation,35 chest wall vibration,36 and blowing air onto the face – in addition to treatment with inhalers.37 Referral to palliative care services can aid in managing refractory dyspnoea. As COPD is a progressive disease with difficult prognostication, advanced care planning should be performed early without waiting for life expectancy to be considered limited in the short term. Recent hospitalisation may be an opportunity to initiate such discussions. |
Expert group
Chairpersons
Prof Lim Tow Keang, Respiratory (NUH)
Dr Valerie Teo Hui Ying, Primary Care (NHGP)
Members
A/Prof John Abisheganaden, Respiratory (TTSH)
A/Prof Gerald Chua, Respiratory (NTFGH)
Dr Eng Soo Kiang, Primary Care (CCK – 24 Hour Family Clinic)
Ms Goh Chee Yen, Nurse Clinician (TTSH)
Mr Lee Tingfeng, Pharmacy (TTSH)
A/Prof Loo Chian Min, Respiratory (SGH)
Adj A/Prof Tan Hsien Yung David, Primary Care (NUP)
Adj Assoc Prof Tan Tze Lee, Primary Care (The Edinburgh Clinic)
Adj A/Prof Augustine Tee, Respiratory (CGH)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Asthma ─ optimising long-term management with inhaled corticosteroid
Patient education aid — Bronchodilator inhalers for COPD [PDF]
Patient education aid — Spirometry test for lung conditions [PDF]
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE) Chronic obstructive pulmonary disease – Diagnosis and management. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2024. Available from: go.gov.sg/acg-copd
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.