
Oral anticoagulation for atrial fibrillation ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) highlights the importance of anticoagulation for preventing stroke among patients with atrial fibrillation (AF). The ACG offers evidence-based recommendations and supporting guideline on initiation of anticoagulation, choice of oral anticoagulant (OAC) for different patient groups, and key monitoring parameters as part of regular follow-up of patients on direct oral anticoagulants (DOACs) or warfarin. A supplementary guide on how to switch between medications is included with the ACG.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Estimate stroke risk for patients with AF and start OAC therapy for those with a modified CHA2DS2VASc score ≥ 2.
Choose a DOAC as the preferred OAC therapy for patients with AF, except for patients with mechanical heart valves or moderate-to-severe mitral stenosis for whom warfarin is the treatment of choice.
Conduct monitoring tests and relevant assessments to ensure the safe use of OAC therapy and to minimise bleeding risk.
Reassess stroke risk and review the need for an OAC in patients who are not on OAC therapy at least annually, and when clinical circumstances change.
Download the ACG and references in PDF
Oral anticoagulation for atrial fibrillation (Nov 2023) [PDF]
Oral anticoagulation for atrial fibrillation references (Nov 2023) [PDF]
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
The prevalence of atrial fibrillation (AF) increases with advancing age. Having AF increases a person’s risk of stroke by 3 to 5 times1,2 and locally, about 19% of strokes occurred in patients with AF in 2020.3
Oral anticoagulation has been shown to be beneficial in patients with AF, with direct oral anticoagulants (DOACs) being associated with lower rates of stroke than warfarin.4 Despite the established benefits of OAC therapy, many patients remain inadequately anticoagulated. In Asia, among patients with high stroke risk (CHA2 DS2 VASc ≥ 2) who should have been prescribed OACs, 15.7% were not prescribed any, or were only prescribed antiplatelet medications.5 Even if patients were prescribed DOACs, research involving Asian populations revealed that 20-56% of patients received subtherapeutic doses, putting them at higher risk of stroke, thromboembolism, and death than those who received optimal doses.6-10
Ensuring adequate anticoagulation is important to reduce the risk of AF-related strokes. A holistic approach should be taken to decide the appropriate OAC therapy; advanced age alone is not a contraindication to anticoagulation.11
Assessment of stroke risk
Recommendation 1: Estimate stroke risk for patients with AF and start OAC therapy for those with a modified 𝘮CHA₂DS₂VASc score ≥ 2.
Assessment of stroke risk is required to decide if OAC therapy is clinically indicated for patients with AF. The CHA2DS2VASc score was developed to estimate stroke risk in patients with AF without mechanical heart valves or moderate-to-severe mitral stenosis, with a higher score reflecting a higher stroke risk.
While gender is one of the risk factors in the CHA2DS2VASc score, female gender alone may not increase stroke risk.12,13 Furthermore, anticoagulation therapy seems to have no benefit for patients with CHA2DS2VASc score = 0 for males and CHA2DS2VASc score = 1 for females.14 For these reasons, this ACG uses a modified CHA2DS2VASc (mCHA2DS2VASc), where gender does not contribute to the decision to initiate OAC therapy (see Figure 1).
Notepad: Stroke risks A mCHA2DS2VASc score of 1 is associated with a stroke risk of 1.1 strokes per 100 patients per year, while a score of 2 is associated with a stroke risk more than twice as high.16 |
Considerations when 𝘮CHA₂DS₂VASc = 1
When mCHA2DS2VASc score = 1, the decision to start OAC should consider patient-specific factors such as age or underlying conditions. Stroke risk is higher for these patient groups:15
Age 65-74 years
Heart failure and age ≥ 35 years
Hypertension and age ≥ 50 years
Diabetes mellitus and age ≥ 50 years
Vascular diseases and age ≥ 55 years
Notepad: Patients with exceptionally high thromboembolic risk The presence of either mechanical heart valves or moderate to severe mitral stenosis is associated with exceptionally high thromboembolic risks for patients with AF. For these patients, OAC therapy initiation is warranted, regardless of additional risk factors for stroke. |
Anticoagulation therapy
Recommendation 2: Choose a DOAC as the preferred OAC therapy for patients with AF, except for patients with mechanical heart valves or moderate-to-severe mitral stenosis for whom warfarin is the treatment of choice.
The choice of OAC is based on patient factors (including bleeding risks, age, comorbidities, renal and liver function, individual preferences), concomitant medications, tolerability, and cost considerations.
Review the indication, choice and dose of OAC at least annually and when the patient’s clinical circumstances change (see Recommendations 3 and 4).
Notepad: Shared decision-making Counsel the patient on the risks and benefits of anticoagulation. Discuss therapeutic options to help them make informed decisions about their treatment. This will facilitate management of potential complications and also encourage adherence. |
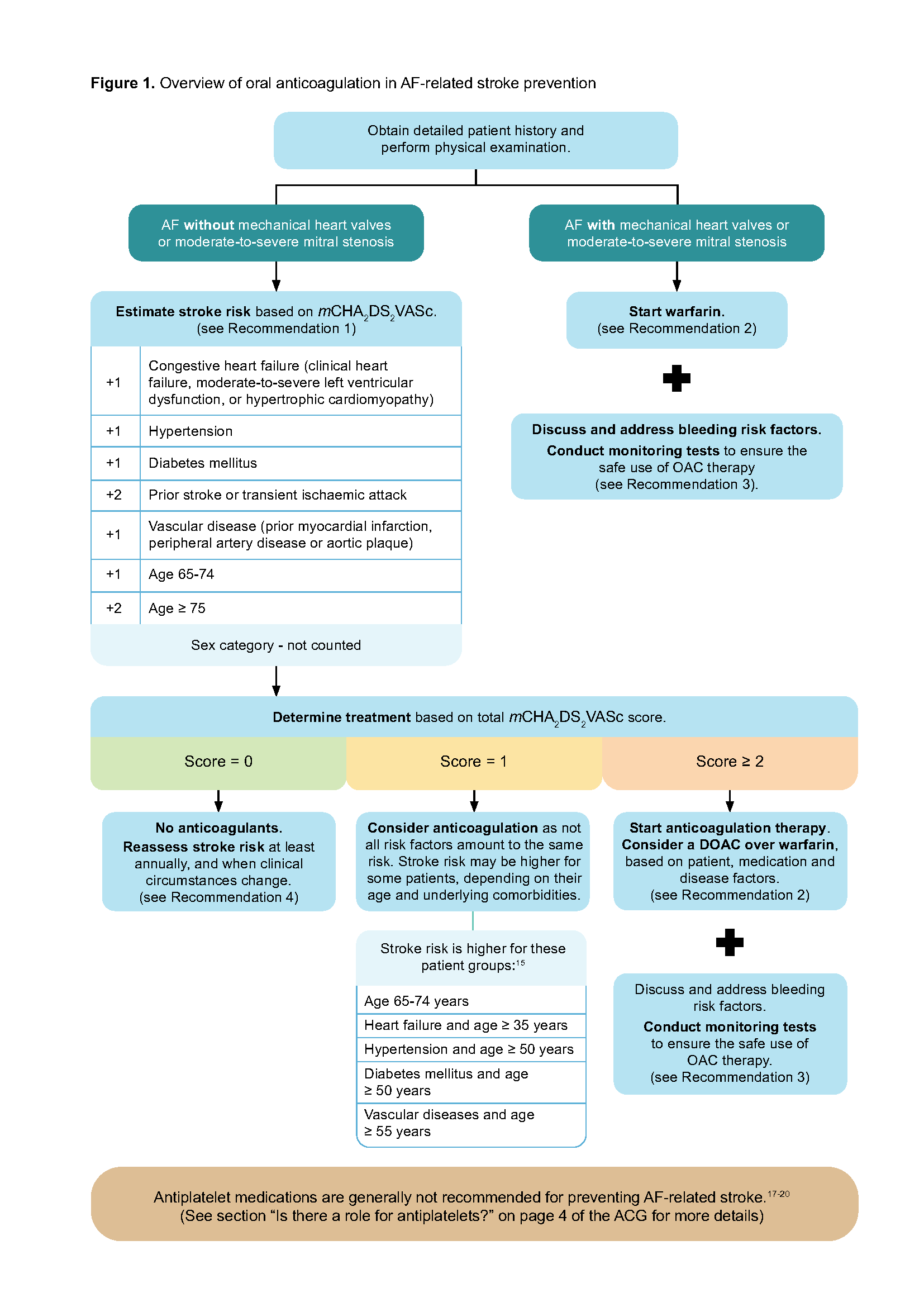
Figure 1. Overview of oral anticoagulation in AF-related stroke prevention
DOACs
Overall, DOACsa are recommended over warfarin for patients with AF without mechanical heart valves or moderate-to-severe mitral stenosis, due to their more favourable benefit-risk profile, fewer drug interactions, and improved convenience for patients as routine coagulation monitoring is not needed. With a lack of head-to-head trials, evidence is insufficient to recommend one DOAC over the others for safety and efficacy.
Compared to warfarin, DOACs are more effective at reducing AF-related strokes and systemic embolisms (SSE), especially for Asian patients.22,23 They are also associated with fewer intracranial haemorrhages (ICH; about 2 to 5 ICH events avoided for every 1,000 patients treated per year) and have similar risks of gastrointestinal (GI) bleeding in Asian patients, compared to warfarin.4,23,24 Another consideration for selecting a DOAC is that there is no need for international normalised ratio (INR) monitoring (e.g. in patients who find it difficult to access, or are reluctant to undergo, frequent INR monitoring). DOACs can also be used for some patients with valvular heart disease (see Table 1), but not for those with mechanical heart valves or moderate-to-severe mitral stenosis.
Table 1. Using DOACs for patients with AF and concomitant valvular heart disease (VHD)
VHD subgroup | DOAC use |
|---|---|
Mechanical heart valves or moderate-to-severe mitral stenosis | Not recommended* 25,26 |
Bioprosthetic heart valves | Recommended† 27-29 |
Aortic stenosis, mild mitral stenosis, aortic, mitral or tricuspid regurgitation | Recommended† 30-31 |
* Harm was shown through higher rates of SSE and major bleeding.
† Benefits were shown through lower risk of SSE and major bleeding.
Routine monitoring with coagulation tests is not necessary or useful in patients on DOACs, except in cases of severe bleeding or urgent surgery. INR is not specific for DOACs and a normal prothrombin time or activated prothrombin time does not rule out the presence of residual DOACs’ effects.32 However, a normal thrombin time can exclude the presence of clinically significant levels of dabigatran.32
Switching eligible patients from warfarin to a DOAC (see Supplementary guide “Switching between anticoagulants”) could be considered, especially for those who already have a poor INR control (i.e., they are unable to maintain a therapeutic INR after multiple attempts to optimise it),33 taking into account patient preferences and likely adherence to DOACs.
Warfarin
Warfarin is the only medication with proven safety and efficacy in patients with atrial fibrillation and mechanical heart valves or moderate-to-severe mitral stenosis and it is therefore the treatment of choice for these patients.34,35
Other considerations for warfarin therapy in patients with AF
Patient factors favouring warfarin | Precautions and practice considerations: |
|
|
Is there a role for antiplatelets?
Antiplatelet medications are generally not recommended for preventing AF-related stroke.17-20 Compared to aspirin, OACs halve the risk of SSE with no significant difference for bleeding outcomes.36 A recent meta-analysis on aspirin reported a moderate reduction in the risk of all-cause stroke, but a significant increase in the risk of major bleeding and ICH compared with no treatment.37 When anticoagulation therapy is contraindicated, the role of antiplatelet medications is unclear due to the lack of direct evidence for these patients with AF.37,38 Based on local expert opinion, aspirin or clopidogrel could be considered for patients with AF in whom OAC therapy is contraindicated and who also have concomitant conditions that would benefit from antiplatelet medications, such as ischaemic heart disease, peripheral vascular disease, or a history of ischaemic stroke, transient ischaemic attack, or myocardial infarction.
a In this ACG, the term DOAC is used in accordance with the recommendation from the International Society on Thrombosis and Haemostasis.21 DOACs are also known as non-Vitamin K antagonist oral anticoagulants (NOACs).
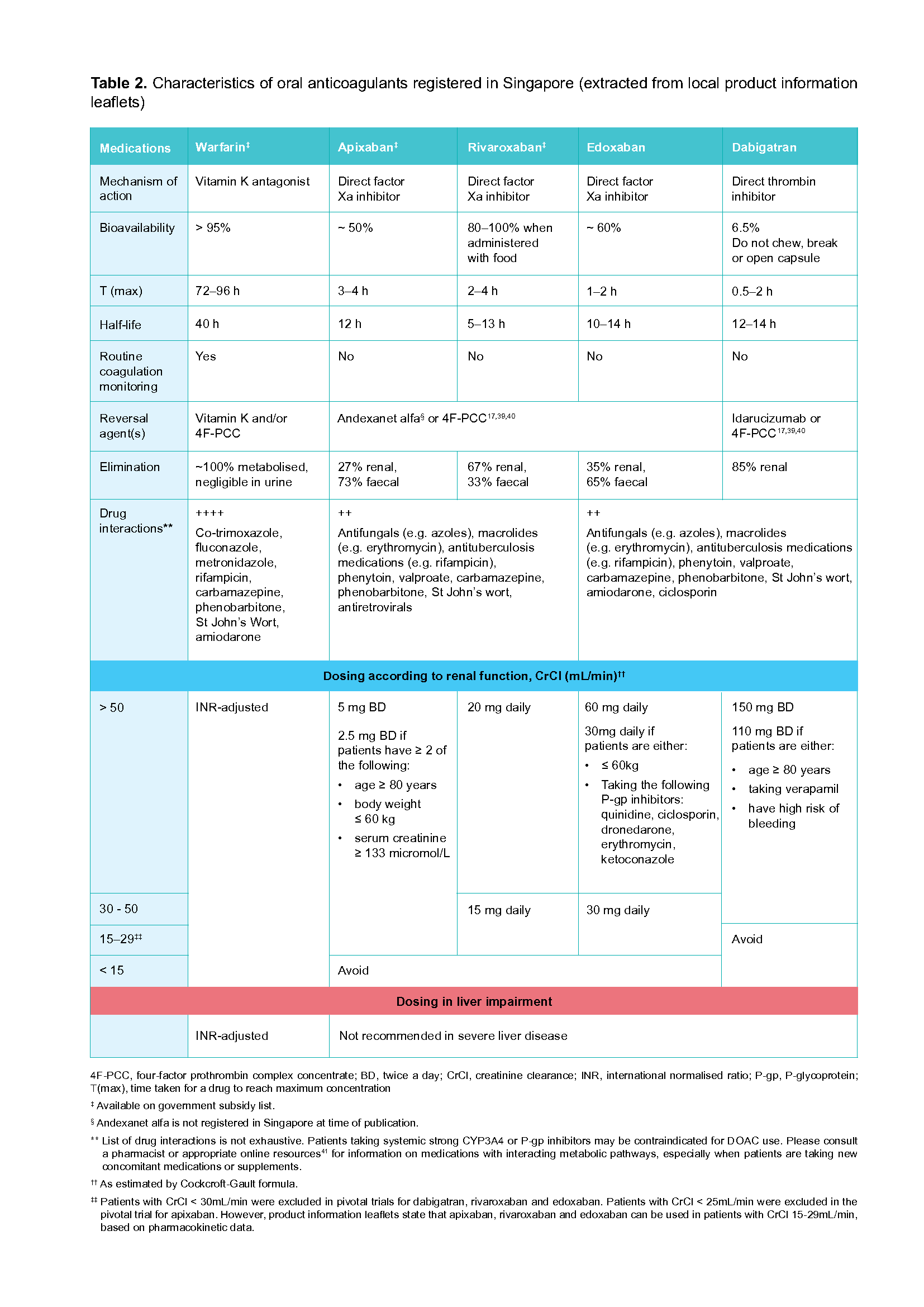
Table 2. Characteristics of oral anticoagulants registered in Singapore (extracted from local product information leaflets)
Click here for larger version of the image
Monitoring and review
Recommendation 3: Conduct monitoring tests and relevant assessments to ensure the safe use of OAC therapy and to minimise bleeding risk.
Regular follow-up is recommended for all patients on OAC therapy to ensure that their treatment is optimised according to patient, drug, and disease factors (see Figure 2 below). More frequent monitoring may be required for individuals at increased risk for bleeding.
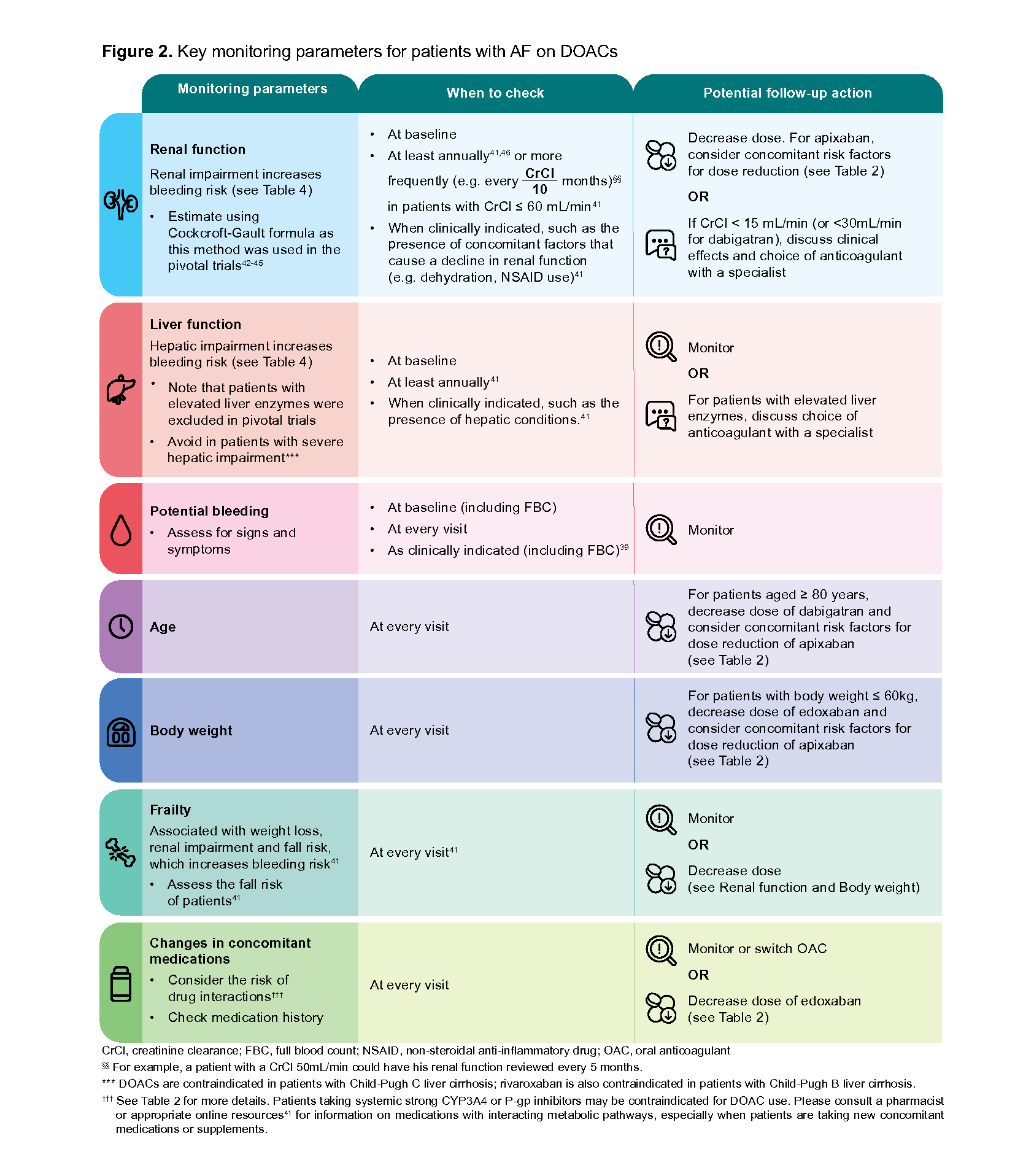
Figure 2. Key monitoring parameters for patients with AF on DOACs
Figure 3. Key monitoring parameters for patients with AF on warfarin
Management of suboptimal INR levels
When a patient on warfarin has INR levels not in the therapeutic range, more frequent INR monitoring and dose adjustments are needed (see Figure 3 and Table 3).47,48 Mild bleeding episodesb can be managed in outpatient settings while severe bleeding episodesc warrant hospitalisations. If reversal of anticoagulation is required due to severe bleeding, patients may be referred to specialists or the emergency department.
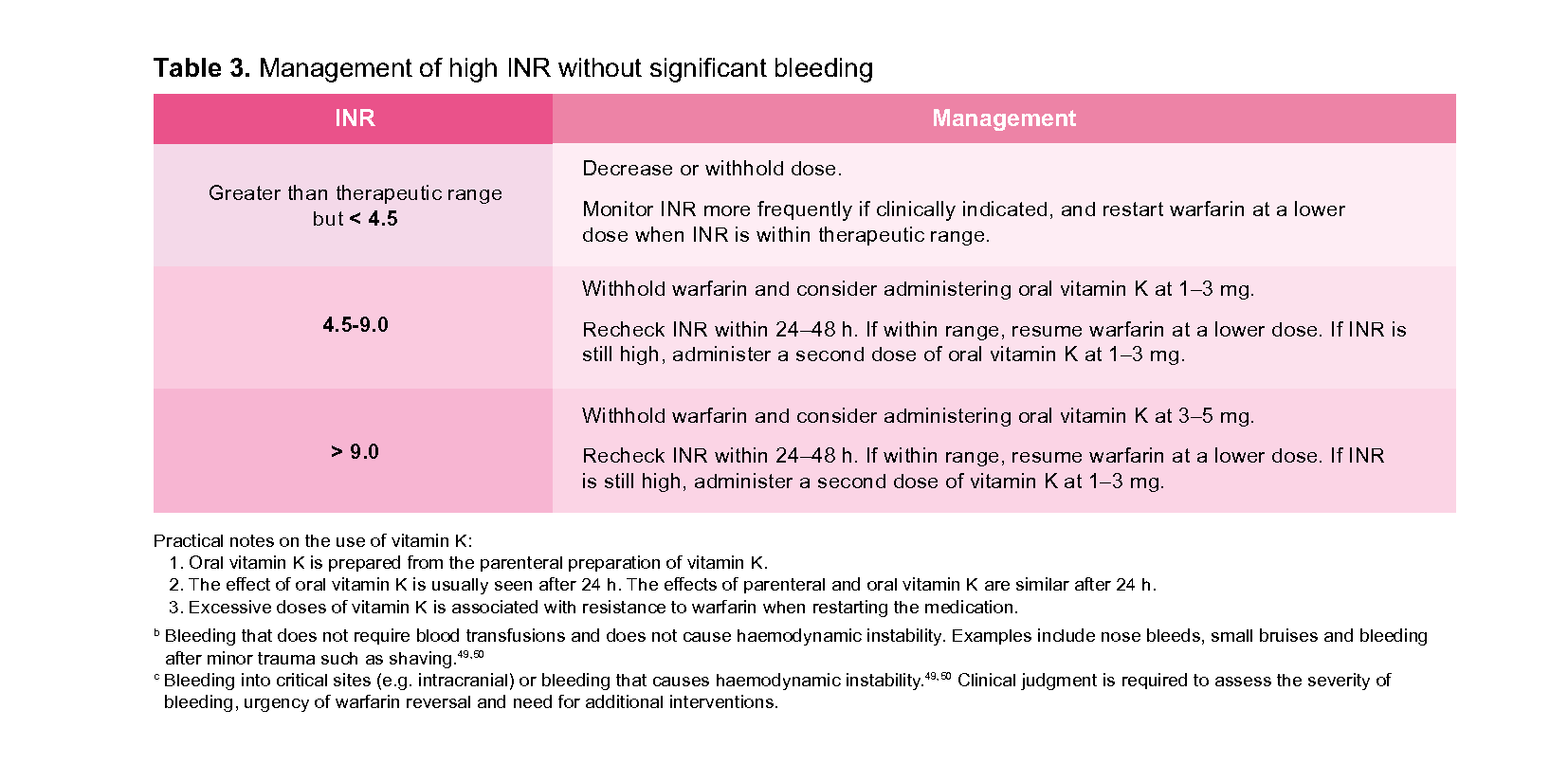
Table 3. Management of high INR without significant bleeding INR Decrease or withhold dose. Greater than therapeutic range but < 4.5
Assessing and addressing bleeding risk
It is important to assess and address bleeding risk throughout the full duration of anticoagulation. Annual major bleeding risks in patients on anticoagulation range from 2.1 to 3.6% for DOACs and 3.1 to 3.4% for warfarin.42-45 Most of these were GI bleeds and less frequently, ICH.
While bleeding risk scores such as HAS-BLED (see Table 4) only have a moderate ability for predicting major bleeding events,51 they are useful to identify modifiable risk factors (see Spanner icon in Table 4).
Notepad: Bleeding risk scores Bleeding risk scores should not be used to withhold anticoagulation. Instead, inform patients accordingly of their bleeding risk and make every effort to reduce bleeding risk. |
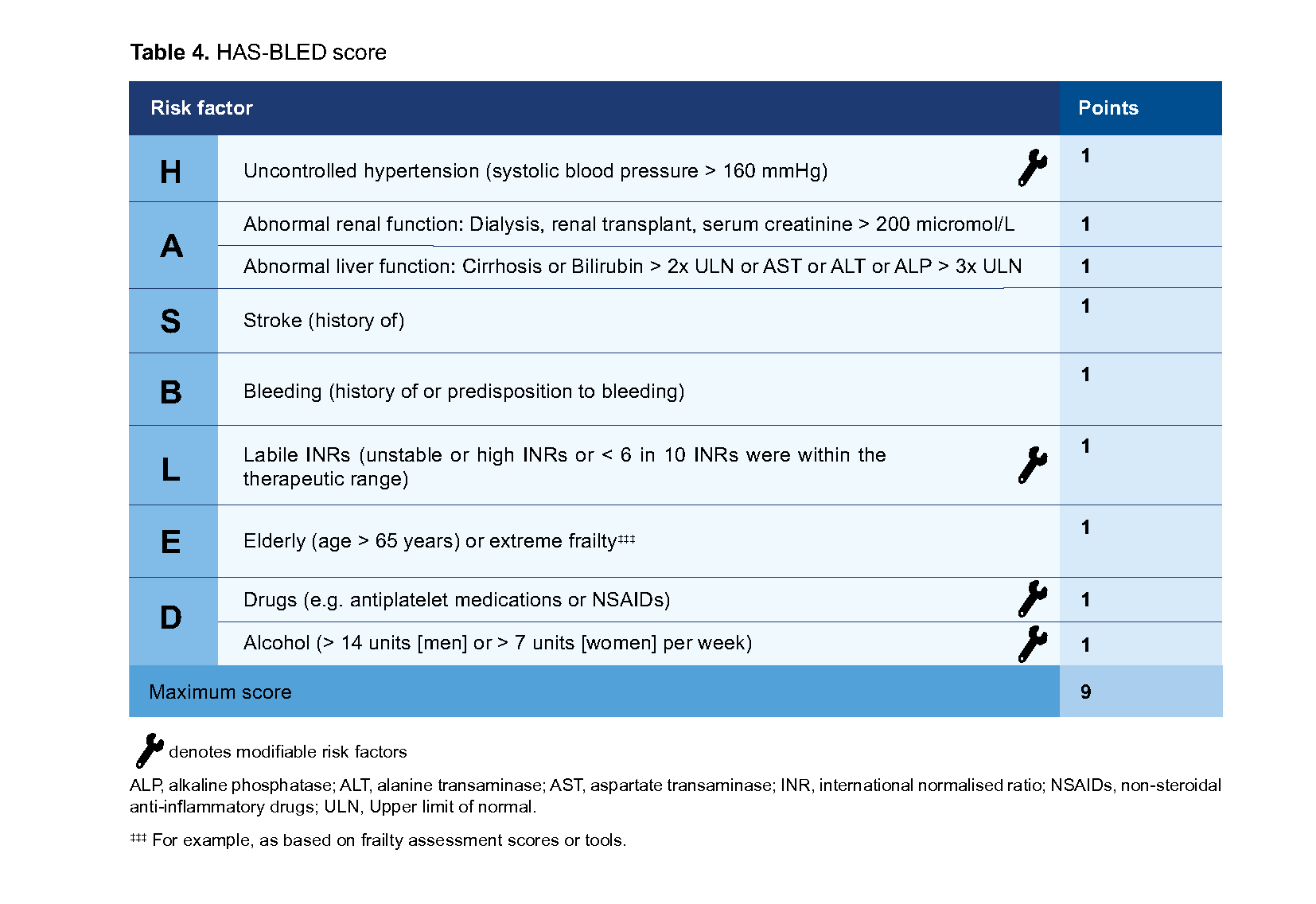
Table 4. HAS-BLED score
Notepad: High bleeding risk A HAS-BLED score of ≥ 3 indicates high bleeding risk, with ≥ 4 bleeds per 100 patients per year.52 Monitor these patients more frequently, and take steps to reduce their bleeding risks. Educate the patient and their carers about recognising signs and symptoms of bleeding. |
Recommendation 4: Reassess stroke risk and review the need for an OAC in patients who are not on OAC therapy at least annually, and when clinical circumstances change.
Stroke risk is not static, and it increases with factors such as age and incident comorbidities. For patients with AF who are not taking OACs, continue to re-assess their mCHA2DS2VASc score at least annually and when clinically indicated.d
d One cohort study of 14,606 Taiwanese patients with AF not taking OAC at enrolment recommended reviewing stroke risk every 4 months; of 6,188 patients who acquired new comorbidities (heart failure, hypertension, diabetes mellitus or vascular diseases), 90% of them experienced an ischaemic stroke at least 4.4 months after acquiring the comorbidities.53
Supplementary Materials
Supplementary guide: Switching between anticoagulants
Expert group
Lead discussant
Dr Lim Toon Wei, Cardiology (NUH)
Chairperson
A/Prof Ching Chi Keong, Cardiology (NHCS)
Members
Dr Bernard Chan, Neurology (NUH)
Mr Kong Ming Chai, Pharmacy (SGH)
Clin A/Prof How Choon How, Family Medicine (CGH)
Dr Hwang Siew Wai, Family Medicine (SHP)
Clin Prof Lee Lai Heng, Haematology (SGH)
Dr Lee Sze Haur, Neurology (NNI@TTSH Campus)
A/Prof Doreen Tan, Cardiology Specialist Pharmacist (NUS/NUHCS)

Feedback
Click here to give us feedback on this ACG.
Related ACGs
Venous thromboembolism - Treating with the appropriate anticoagulant and duration
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Oral anticoagulation for atrial fibrillation. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-oac-for-af
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.