
Upper respiratory tract infections — rational antimicrobial use ACG
Last updated 9 June 2026
Overview
This ACE Clinical Guideline (ACG) provides guidance on appropriate antimicrobial use for treating upper respiratory tract infections (URTIs) in primary and generalist care settings, highlighting situations where antimicrobial therapy can be safely withheld, and other instances where timely administration of antimicrobial therapy may be beneficial.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Assess patients’ clinical signs and symptoms and establish a working diagnosis (e.g. uncomplicated URTI, acute rhinosinusitis, pharyngotonsillitis, acute otitis media).
Do not prescribe antibiotics for patients with uncomplicated URTI.
For patients with acute rhinosinusitis, pharyngotonsillitis or acute otitis media:
When a bacterial infection is clinically suspected, consider if an antibiotic is needed based on clinical features and individual risk factors for severe disease outcome.
Do not routinely prescribe antivirals for otherwise healthy patients with uncomplicated URTI.
Download the ACG, references and Expert Group details in PDF
Upper respiratory tract infections – rational antimicrobial use (May 2026) [PDF]
URTI ACG references (May 2026) [PDF]
URTI ACG EG composition and other details (May 2026) [PDF]
ACG EtR framework
The Evidence-to-Recommendation (EtR) framework is a document that outlines the underpinning evidence and rationale for the recommendations in our ACGs. Download the EtR framework below to learn more about factors that have informed the strength of the ACG recommendations, including certainty of evidence, clinical benefit/risk balance, local resource implications, feasibility considerations, patient preferences and values, acceptability and other considerations.
URTI EtR framework with summary of findings (May 2026)
Request for a hard copy
Click here
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Overuse of antibiotics in primary care in Singapore is a common and significant problem, well recognised and acknowledged by most (82.7%) general practitioners surveyed.1 Antibiotic overprescribing is especially common for upper respiratory tract infections (URTIs) in both adult and paediatric populations.
Antibiotics and antivirals are often not indicated for URTIs as these conditions are usually self-limiting, and most untreated patients (82%) are symptom free after one week.2-5 As URTIs are one of the most common reasons for consultations in the primary care setting, this presents an opportunity for healthcare professionals to steward antimicrobial use through judicious prescribing and patient education. This ACE Clinical Guideline (ACG) provides guidance on appropriate antimicrobial use for treating URTIs in primary and generalist care settings, highlighting situations where antimicrobial therapy can be safely withheld, and other instances where timely administration of antimicrobial therapy may be beneficial.
Diagnosis and severity assessment
Recommendation 1: Assess patients’ clinical signs and symptoms and establish a working diagnosis (e.g. uncomplicated URTI, acute rhinosinusitis, pharyngotonsillitis, acute otitis media).
A comprehensive assessment is essential to establish an accurate working diagnosis which will guide subsequent management decisions, including whether antimicrobials are needed.
Common diagnoses of URTIs
URTIs encompass many acute illnesses and are predominantly caused by viruses. Common URTI diagnoses include uncomplicated URTI, acute rhinosinusitis, pharyngotonsillitis, laryngitis and acute otitis media (AOM). While these conditions share many overlapping symptoms, each presents with distinct clinical characteristics. Figure 1 summarises the key features of common URTI diagnoses.
During the assessment of an URTI, clinicians should remain mindful of other potential differential diagnoses that may require different treatment approaches (see 'Differential diagnoses').
Notepad: Differential diagnoses
Refer to the ACGs on the following conditions for further details: |
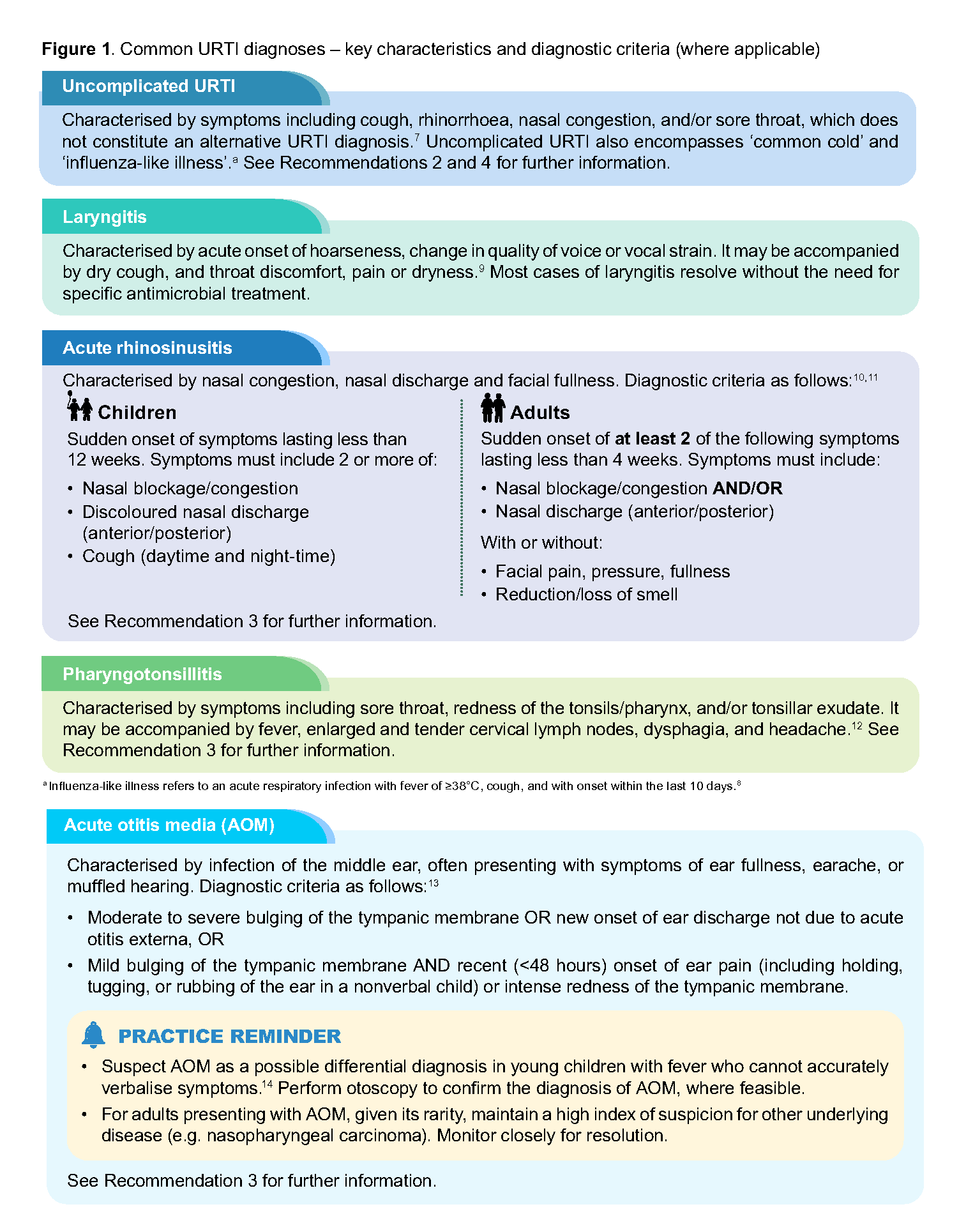
Figure 1. Common URTI diagnoses – key characteristics and diagnostic criteria (where applicable)
Red flags for possible serious conditions
Clinicians must maintain clinical vigilance to identify red flags and consider alternative serious diagnoses (e.g. epiglottitis, deep neck infections, meningitis) that may present with overlapping URTI-like symptoms. Where a more serious disease is suspected, a physical consultation is preferred to allow for a more thorough assessment. Figure 2 summarises some red flags which should prompt suspicion of more serious differential diagnoses, and consideration of care escalation.
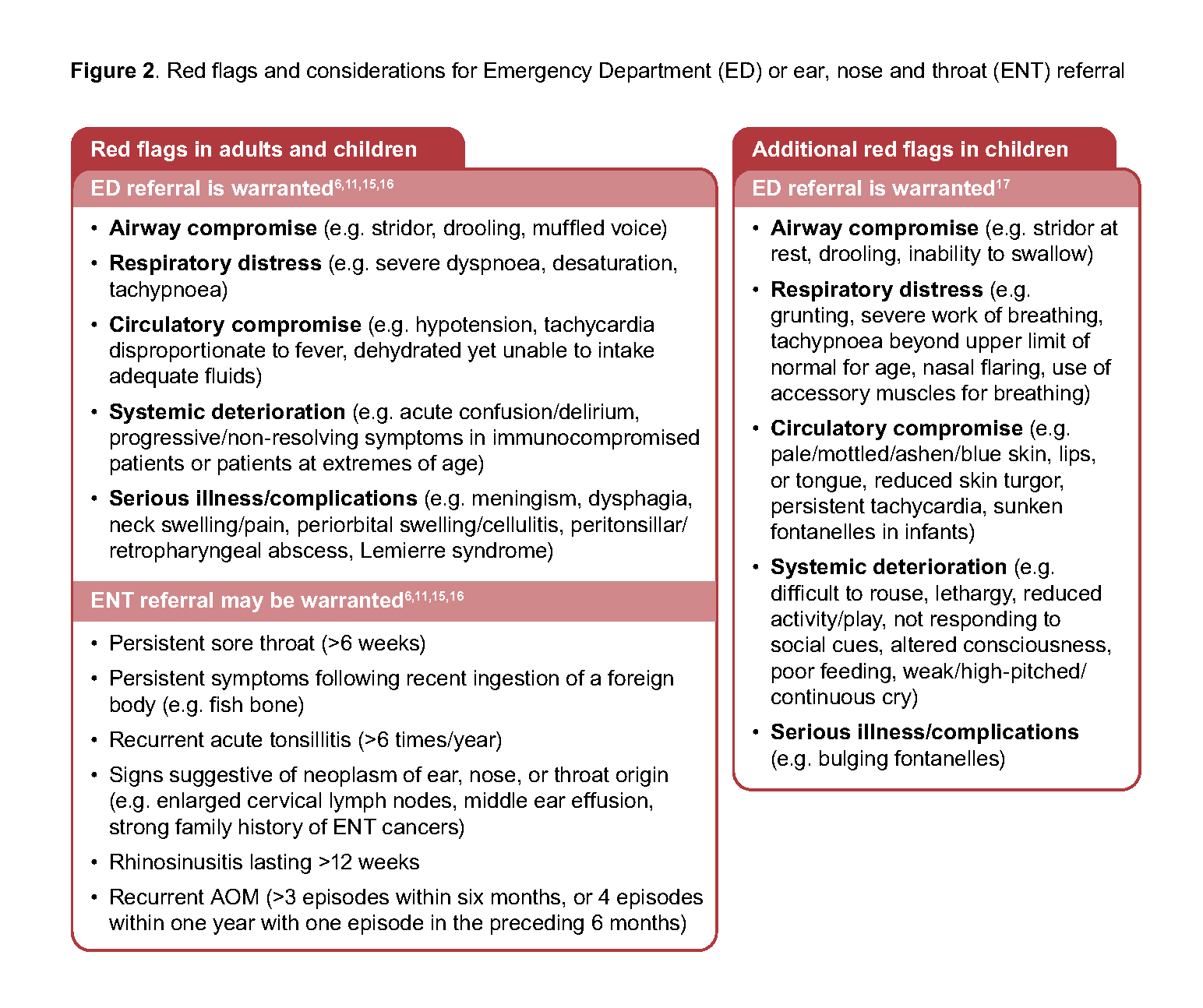
Figure 2. Red flags and considerations for Emergency Department (ED) or ear, nose and throat (ENT) referral
Consideration of antibiotics for URTI management
Recommendation 2: Do not prescribe antibiotics for patients with uncomplicated URTI.
The potential harms of antibiotic use for uncomplicated URTIs generally outweigh the limited benefits. Severe or suppurative complications arising from uncomplicated URTIs are rare,5 and the clinical benefits of antibiotic therapy remains uncertain (in the absence of risk factors or complications), as most patients recover at a similar rate regardless of whether antibiotics are used.5,18,19
Antibiotic exposure substantially increases the risk of antimicrobial resistance. Amongst primary care patients, the odds of developing resistance to an antibiotic are two times higher for a patient who received a course of antibiotic compared to a patient who did not, and these odds increase with longer treatment duration or repeated courses.20
Adverse effects are common with antibiotic use, with an estimated 1 in 10 patients experiencing symptoms such as nausea, vomiting, or diarrhoea.18 Less frequently, antibiotic use can result in Clostridioides difficile colitis, which carries significant morbidity.21,22
When there is poor patient knowledge and misperceptions about antibiotic use, patients may expect clinicians to prescribe antibiotics even when it is unnecessary;23–25 this has been shown to influence antibiotic prescribing practices.24 As such, it is important for clinicians to exercise their clinical judgement to determine when antibiotics are truly indicated. As uncomplicated URTIs are common presentations and self-limiting, URTI consultations present valuable opportunities for patient education about unnecessary antibiotic use and its associated harms.
PATIENT EDUCATION Manage patient’s expectations for antibiotics
Click here for more patient education materials on responsible use of antibiotics. |
Figure 3. Duration of common URTI symptoms
Duration of URTI symptoms | |
|---|---|
For adults | For children30 |
URTI episodes last 8 days on average.26 However, specific symptoms can vary considerably in duration. For patients with:
| URTI episodes last 7-15 days on average, with 50% of the population recovering by day 10. Specific symptoms vary in duration. For patients with:
|
Symptomatic management of uncomplicated URTI
Recognising that antibiotics have minimal to no effect on symptomatic relief (e.g. cough),31,32 symptomatic medications are commonly prescribed to manage the symptoms of URTIs. While numerous symptomatic medications are available and marketed for this purpose, the evidence supporting the efficacy of most of these medications remains uncertain.15,33-41 This may be due to the self-limiting nature and short duration of URTIs, which can make it challenging to detect significant differences in outcomes.
Some preparations that may be effective include:
Echinacea – may help shorten URTI duration (effects may vary between preparations);42 not routinely recommended in children
Honey – may help with cough frequency and severity; contraindicated in children <1 year (due to risk of infant botulism)43
Intranasal mometasone or saline irrigation – may help with management of nasal blockage/congestion in post-acute rhinosinusitis (i.e. when rhinosinusitis symptoms persist >10 days).11 The use of intranasal steroid in children are usually restricted to those age ≥2 years old (depending on product).
If prescribing symptomatic medications, be mindful of their associated precautions. For example:b
Avoid medications that are contraindicated or unsuitable for the paediatric population.
Mucolytics should be avoided in children <2 years old due to choking risk related to inability to expectorate loose phlegm.
Promethazine is contraindicated for children <2 years old due to risk of respiratory depression.
Codeine-containing cough preparations are contraindicated in children <12 years old.
Oral decongestants (e.g. pseudoephedrine or phenylephrine) should be avoided in children <2 years old and used with caution in children 2-12 years old (depending on product), due to adverse drug reactions (e.g. tachycardia, palpitation, hypertension).
Exercise caution when prescribing multiple antihistamines concurrently (e.g. prescribing promethazine or diphenhydramine cough syrup with another first- or second-generation oral antihistamine), or when prescribing sedating antihistamines in the elderly population due to risk of falls.
Choose an alternative medication if there is a significant risk of medication interaction (e.g. dextromethorphan with alcohol, sleeping pills, anxiolytics) or adverse drug reaction (e.g. acute retention of urine with codeinecontaining cough suppressant).
PRACTICE REMINDER
|
PATIENT EDUCATION Ensure patients understand the importance of keeping up to date with recommended vaccinations
Click the links for more information on Covid-19 vaccination, NCIS and NAIS Remind patients to practice good hand hygiene and respiratory etiquette, especially during acute illness
|
b Examples are non-exhaustive. Information from local product information leaflet/product insert have been referenced and supplemented with information from consolidated product monographs (e.g. Lexicomp) and expert consensus where local product inserts are unavailable or unclear. Refer to local product inserts for full details before prescribing.
Recommendation 3: For patients with acute rhinosinusitis, pharyngotonsillitis or acute otitis media:
When abacterial infection is clinically suspected, consider if an antibiotic is neededbased on clinical features and individual risk factors for severe disease outcome.
To decide whether an antibiotic is clinically warranted for the treatment of acute rhinosinusitis, pharyngotonsillitis or AOM:
Assess if the patient’s presenting clinical signs and symptoms point towards a significant bacterial infection (Figure 4). Patients with signs and symptoms suggestive of a significant bacterial infection are likely to benefit from antibiotic therapy.
Consider if the patient has risk factors which increases their likelihood of severe disease and exercise clinical judgement to decide if the patient’s risk factors warrant lowering the treatment threshold for initiating antibiotics. Risk factors which increase the likelihood of severe disease include:6,10,15,44-50
Older age (>65 years)
Immunocompromised status
Chronic pulmonary disease
Cardiovascular disease
Chronic kidney disease
Chronic metabolic disease (including diabetes mellitus)
Presence of upper airway structural abnormalities/variants (e.g. in children with congenital diseases like Down syndrome)
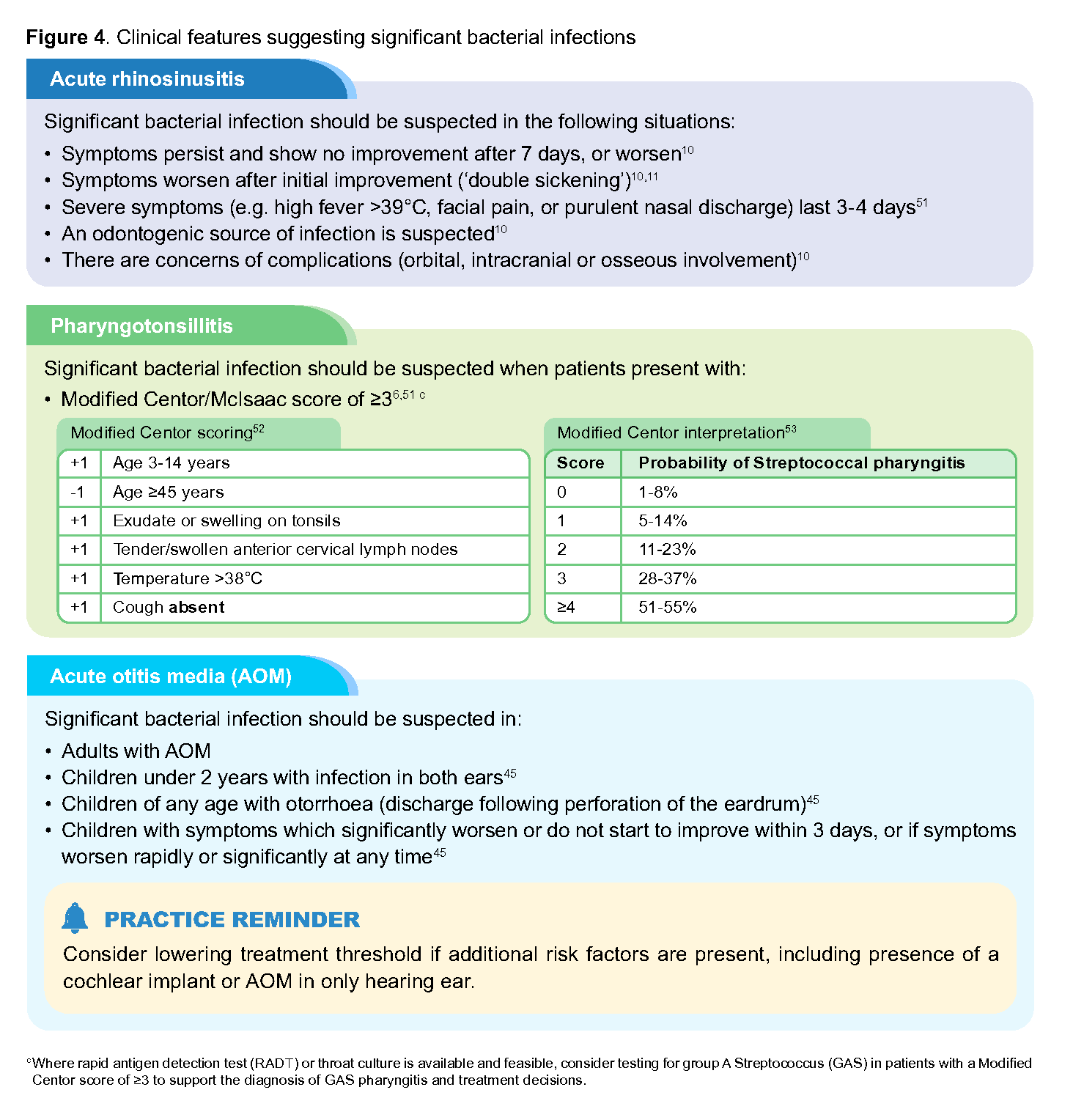
Figure 4. Clinical features suggesting significant bacterial infections
Selecting appropriate antibiotics
If the decision is made to start antibiotics for a patient with a suspected bacterial infection:
Consider the underlying URTI condition for which antibiotics are prescribed (e.g. acute rhinosinusitis, pharyngotonsillitis, acute otitis media)
Identify any risk factors which may suggest resistant organisms, such as recent hospitalisation
Evaluate the suitability of antibiotic choice for the individual patient (e.g. medication allergies, likelihood of adverse effects)
4. Select the narrowest spectrum antibioticd for the shortest effective course at an appropriate dose54 (refer to Supplement 1 on page 9)
Patient-reported drug allergies are common in clinical practice and it has been reported that most self-reported drug allergies are inaccurate.55,56 Similarly, patients with documented or reported penicillin allergy may not have true penicillin allergy and it is advisable to verify the penicillin allergy (e.g. clarify characteristics of past reactions and review documented medication history to check if the patient has previously tolerated penicillin).
PATIENT EDUCATION Promote correct antibiotic use
click here to access patient counselling resources on responsible antibiotics use |
Dispensing antibiotics only when they are immediately required
To prevent unnecessary antibiotic use, consider delaying the dispensing of antibiotics if they are not deemed to be required immediately, for example by: 32,45,57,58
Issuing an antibiotic prescription at the initial visit but with delayed dispensing instructions
Advising the patient to recontact the clinic to request for antibiotics at a later day
Clear guidance must be provided to patients on when to have the prescription dispensed, or when to recontact the clinic to request for antibiotics (e.g. symptoms worsen or fail to improve after 3-5 days) and when to return for review (e.g. development of new symptoms or red flags, persistent fever).45,58,59
The practice of dispensing antibiotics at the initial visit with instructions for delayed use is best reserved for circumstances where delayed dispensing of antibiotics is not feasible. While this practice facilitates timely treatment if a patient's condition worsens, its impact on inappropriate or unnecessary antibiotic use is unknown. There is a risk that the dispensed antibiotics may be used before clinically indicated. Unused antibiotics pose an unnecessary expense to the patient and may inadvertently encourage future self-medication.
d In line with the World Health Organization’s AWaRe classification (Access, Watch and Reserve); antibiotics in the 'Access' category generally have a lower resistance potential than the 'Watch' and 'Reserve' categories.54
Antivirals in URTI management
Recommendation 4: Do not routinely prescribe antivirals for otherwise healthy patients with uncomplicated URTI.
Uncomplicated URTIs are predominantly caused by viruses which include rhinovirus, adenovirus, non-severe acute respiratory syndrome (non-SARS) seasonal coronavirus, and respiratory syncytial virus; most uncomplicated URTIs are not caused by influenza virus or COVID-19 (SARS-CoV2) virus.7,60,61 Even when they are, most conditions would be self-limiting without the need for antivirals, especially for patients who are otherwise healthy.
For influenza, baloxavir and oseltamivir are the more commonly used antivirals for mild-to-moderate influenzae locally. However, baloxavir and oseltamivir only provide modest benefits in faster symptom resolution, by approximately 24 hours and 18 hours respectively, with no impact on hospitalisation rates and mortality.50,63 Treatment with antivirals may also result in adverse effects, commonly gastrointestinal disturbances (e.g. nausea and vomiting).50,64,65
For COVID-19, nirmatrelvir + ritonavir is available locally for mild-to-moderate COVID-19. However, its use should be limited to patients who are at high risk of progressing to severe COVID-19. For patients at low risk of developing severe disease, the risk of potential adverse effects, medication interactions and associated treatment cost outweigh the potential benefits of treatment with nirmatrelvir + ritonavir.66 When indicated for patients at high risk of developing severe disease, treatment should begin as early as possible and within five days of symptom onset. When prescribing nirmatrelvir + ritonavir, counsel the patient on the potential adverse effects (of which altered taste and diarrhoea are commonly described), potential drug-drug interactions and associated treatment cost. For more information on COVID-19 treatment and nirmatrelvir + ritonavir use, refer to COVID-19 - National Centre for Infectious Diseases.
PRACTICE REMINDER For patients with risk factors for severe disease:f
|
eMild-to-moderate influenza is defined as influenza without severe illness or syndrome [e.g. sepsis, septic shock, severe pneumonia, acute respiratory distress syndrome (ARDS), multi-organ failure] or mortality.62
f For risk factors for severe influenza, see risk factors in Recommendation 3. For risk factors for severe COVID-19, refer to Annex A of MOH Circular 67/2025.
g Refer to MOH Drug Advisory Committee Technology Guidance for Medication Assistance Fund (MAF) clinical criteria for nirmatrelvir + ritonavir.
hInterpret results based on the sensitivity and specificity of individual RADT kits, as marked variation may be present across kits.
Supplementary guides
Expert Group
Chairpersons
Adj A/Prof David Tan Hsien Yung, Family Medicine (NUP)
A/Prof Barnaby Young, Infectious Disease (NCID)
Members
A/Prof Chua Peng Wei Melvin, Geriatric Medicine (SKGH)
Dr Chung Wei Teng (Gladys), Pharmacy (NUH)
Dr Chung Shimin Jasmine, Infectious Disease (SGH)
Mr Lam Young Zheng, Pharmacy (Unity)
Dr Derek Li Shi'an, Family Medicine (Raffles Medical)
Dr Loh Jiashen, Infectious Disease (Farrer Park Hospital)
Dr Ong Sin Hwee, Family Medicine (NHGP)
Dr I Gusti Ngurah Prawira Suartha Oka, Family Medicine (SHP)
Dr Arthi Premkumar, Geriatric Medicine (AH)
Dr Jeevan Raaj, Emergency Medicine (SGH)
Dr Seo Woon Li, Paediatrics (NUH)
Dr Sharon Shen Fengli, Family Medicine (EH Medical Family Clinic)
Dr Somasundaram Subramaniam, ENT (Allergy & Sinus ENT Specialist Centre)
Dr Weng Yanyi, Emergency Medicine (TTSH)
Dr Wong Poh Chen Petrina, Paediatrics (Petrina Wong Clinic for Children, Respiratory & Sleep)
Dr Wong Tien Hua, Family Medicine (Mutual Healthcare Medical Clinic)
For more information on the Expert Group composition and other details, click here.

Feedback
Click here to give us feedback on this ACG.
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Upper respiratory tract infections – rational antimicrobial use. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2026. Available from: go.gov.sg/acg-urti
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.