
Urinary tract infections — appropriate diagnosis and antibiotic use for uncomplicated cystitis and pyelonephritis ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) highlights the importance of appropriate diagnosis and treatment of urinary tract infections (UTI) to reduce inappropriate antibiotic use. The ACG offers evidence-based recommendations on the treatment of UTI in adults, focusing on uncomplicated acute cystitis and pyelonephritis in healthy, non-pregnant pre-menopausal women. Principles of appropriate selection of antibiotics as well as patient education on antibiotic use and antimicrobial resistance awareness are also highlighted.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Avoid routinely screening for and treating asymptomatic bacteriuria.
Diagnose uncomplicated cystitis based on history and presentation in patients with two or more typical signs or symptoms such as dysuria, frequency, urgency, or absence of vaginal discharge.
a. Conduct a urine dipstick test to confirm diagnosis of uncomplicated cystitis where there is uncertainty; and
b. Conduct a urine culture and sensitivity test for unresolved or recurrent cystitis.Suspect uncomplicated pyelonephritis in patients presenting with sudden-onset flank pain or tenderness, particularly when accompanied by other systemic symptoms such as fever, nausea or vomiting.
Conduct urine tests (dipstick or microscopy, plus culture and sensitivity) for all patients with suspected uncomplicated pyelonephritis to confirm diagnosis and guide management.
Prescribe nitrofurantoin empirically for uncomplicated cystitis; if nitrofurantoin is not suitable, prescribe amoxicillin-clavulanate or fosfomycin.
Prescribe amoxicillin-clavulanate empirically for patients with uncomplicated pyelonephritis and tailor antibiotic choice accordingly when urine culture and sensitivity results are available; if amoxicillin-clavulanate is not suitable, consider cefuroxime as an alternative.
Download the ACG and reference in PDF
UTI – appropriate diagnosis and antibiotic use references (Dec 2023) [PDF, 422 KB]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Urinary tract infection (UTI) is a common bacterial infection in females, affecting about 1 in 2 women at some point in their life.1 UTIs are associated with reduced quality of life2 and significant clinical and economic burden.3
Escherichia coli (E. coli) is the main causative bacteria for UTIs locally and internationally.4,5 Antibiotic therapy is effective in treating UTIs, and reduces the severity of infections and duration of symptoms.6 However, the susceptibility of E. coli to antibiotics is evolving over time, and high antibiotic resistance, particularly towards ciprofloxacin and cotrimoxazole, has been reported for E. coli locally.4,5,7 Inappropriate use of antibiotics remains one of the main issues contributing to antimicrobial resistance (AMR) problems globally. This ACG aims to provide updated guidance on the appropriate use of antibiotics for UTIs in Singapore especially for non-pregnant pre-menopausal women.
Urinary tract infections (UTIs) can involve different parts of the urinary tract including the bladder and the kidneys. UTIs are commonly classified into lower UTI involving the bladder (cystitis), versus upper UTI involving the kidneys (pyelonephritis). UTIs can be uncomplicated or complicated depending on the nature of the associated infection and likelihood of developing complications:8,9
• Uncomplicated UTI: UTI limited to non-pregnant women with no known relevant anatomical and functional abnormalities of the urinary tract, or no known relevant comorbidities.
• Complicated UTI: UTI associated with an increased chance of a complicated course, which increases the risk that the infection will be more serious than expected.
Figure 1 shows a common classification of selected UTIs, with the focus of the ACG highlighted.
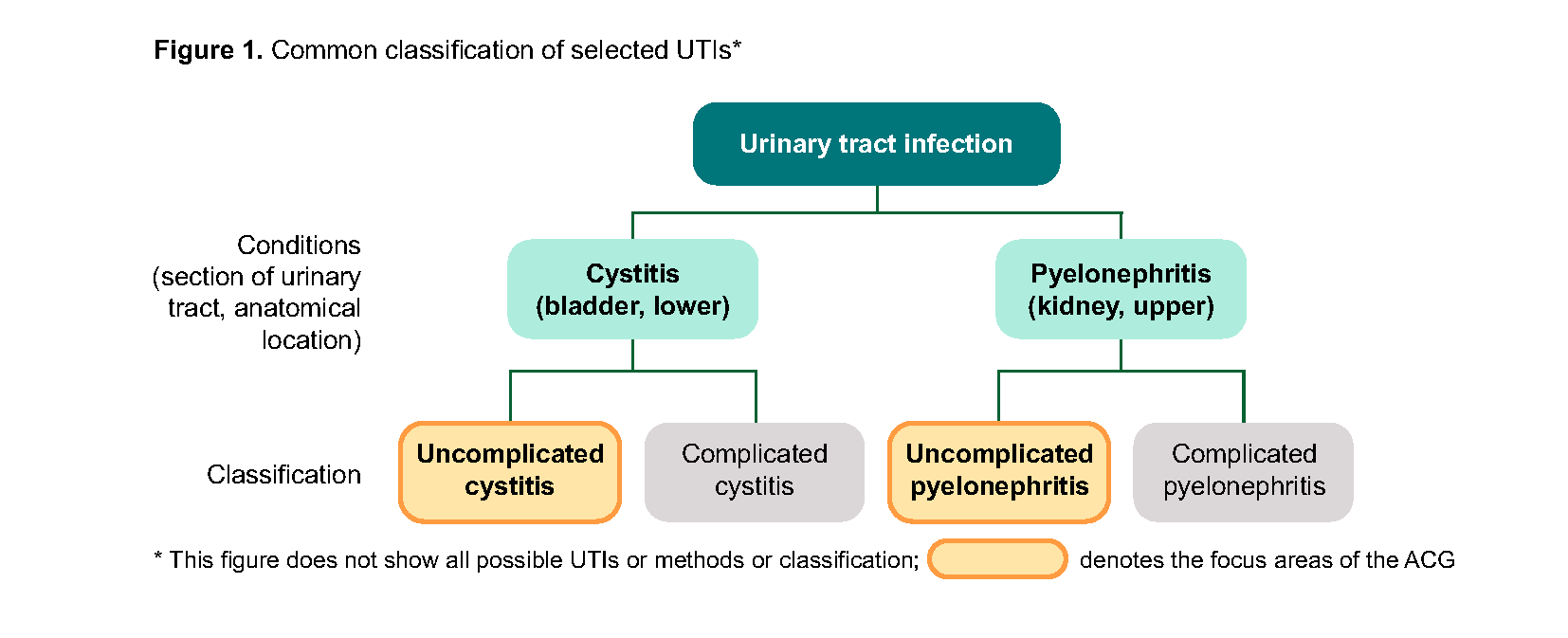
Figure 1. Common classification of selected UTIs*
As UTIs more commonly occur in women than men, this ACG’s main focus is on acute uncomplicated cystitis and acute uncomplicated pyelonephritis in non-pregnant pre-menopausal women. Other relevant populations (e.g., men) and situations (e.g., recurrent cystitis) will be briefly mentioned in some sections.
The following are outside the scope of the ACG: UTIs in individuals under 16 years old, and all complicated UTIs including UTIs in pregnant women, catheter-associated UTIs, and urosepsis.
Assessment and diagnosis of UTI
Recommendation 1: Avoid routinely screening for and treating asymptomatic bacteriuria.
Asymptomatic bacteriuria refers to the isolation of a significant count (>105 bacteria/mL) of a single bacterial species from a clean catch urine specimen of an individual who has no acute signs or symptoms of a UTI.9,10 Asymptomatic bacteriuria may be observed during routine health screening or along with other investigations in non-pregnant women who are healthy.
Screening and treatment for asymptomatic bacteriuria in healthy, non-pregnant women should not be routinely conducted. This is because the evidence suggests no differences in outcomes (development of symptomatic UTI or complications such as urosepsis or pyelonephritis) between those treated with antibiotics for asymptomatic bacteriuria compared to those not treated with antibiotics.11 While antibiotic therapy is associated with eradicating more urinary pathogens, it is also associated with more adverse events, including development of antibiotic resistant bacteria. Additionally, unnecessary screening and treatment are associated with increased cost and resource utilisation.
Recommendation 2: Diagnose uncomplicated cystitis based on history and presentation in patients with two or more typical signs or symptoms such as dysuria, frequency, urgency, or absence of vaginal discharge.
Uncomplicated cystitis occurs in non-pregnant women with no known relevant urological abnormalities or comorbidities.8-10 In most cases, uncomplicated cystitis can be diagnosed based on presenting history, and signs and symptoms. Figure 2 summarises the typical course of action for managing patients with suspected UTI based on the patient’s initial signs and symptoms.
The presenting signs and symptoms may vary among patients, but the most common classic symptoms include:8,10,12
Frequency
Urgency
Dysuria
Other signs and symptoms may include incomplete emptying, nocturia, abdominal pain, chills, foul-smelling urine, and haematuria.12 The presence of vaginal discharge or irritation reduces the probability that the signs and symptoms are due to cystitis (see Examples of differential diagnoses for cystitis for other conditions which may present with similar signs and symptoms).
Diagnose uncomplicated cystitis if there are ≥2 typical signs or symptoms, such as dysuria, frequency, urgency, or absence of vaginal discharge.
In addition, the patient’s history would usually include risk factors which are associated with cystitis (see examples in Table 1).
Notepad: Examples of differential diagnoses for cystitis13
|
Table 1. Examples of risk factors for cystitis
Risk factors associated with healthy pre-menopausal women | Other risk factors |
|---|---|
|
|
Other populations |
|---|
The presenting signs and symptoms of acute cystitis in men are similar to those in women. However, the diagnosis of UTI in men cannot be made based on signs and symptoms alone and needs further assessments (see Other populations under Recommendation 3). |
For non-pregnant women with recurrent cystitis (i.e. 2 episodes within 6 months, or 3 episodes within 12 months),15,16 the presenting signs and symptoms of acute cystitis are similar to those in women without recurrent cystitis. However, in women with recurrent cystitis, consider reviewing possible causes of recurrent cystitis, and conducting further assessments to inform management (see Other populations under Recommendation 3). |
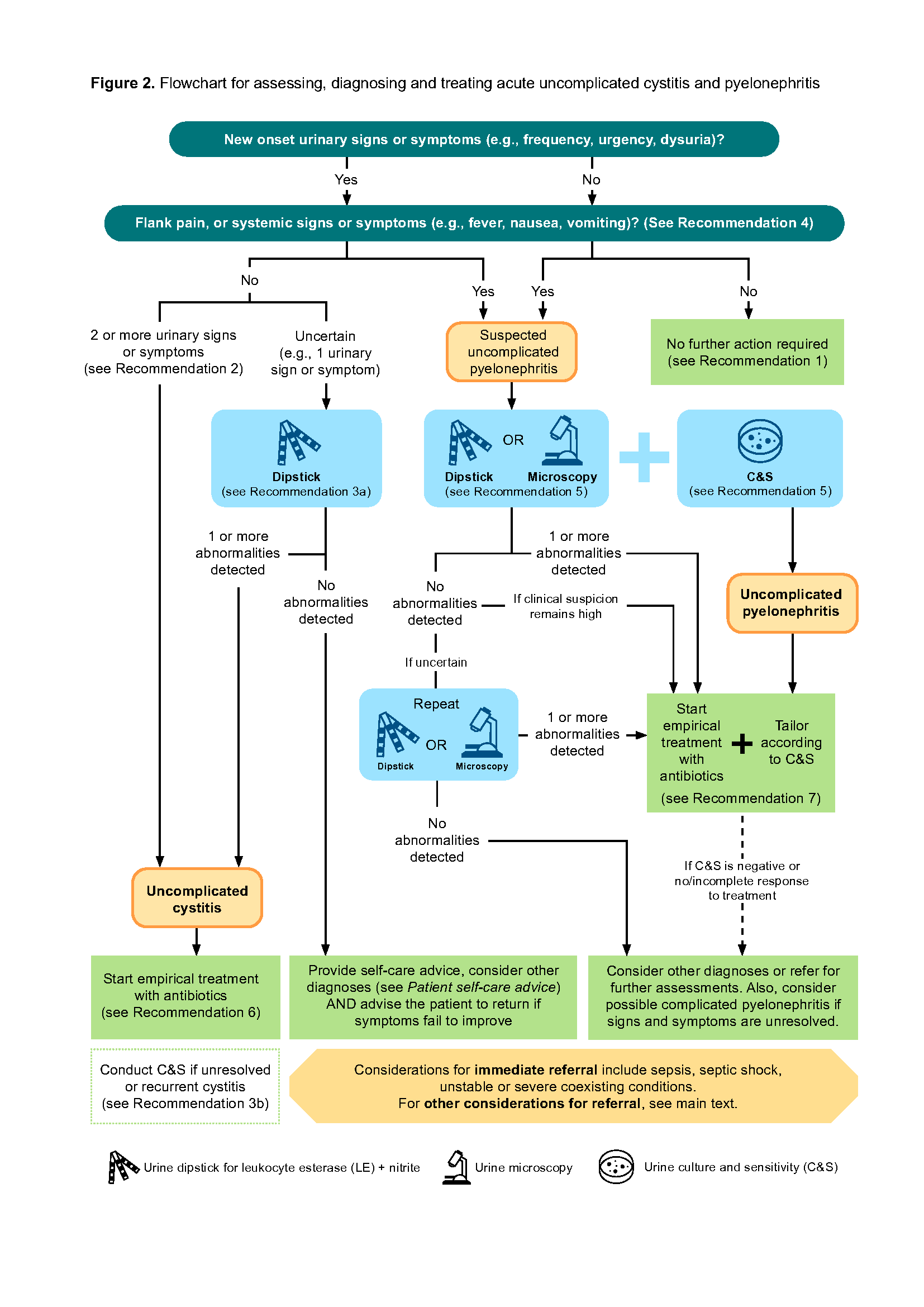
Figure 2. Flowchart for assessing, diagnosing and treating acute uncomplicated cystitis and pyelonephritis
Recommendation 3: a. Conduct a urine dipstick test to confirm diagnosis of uncomplicated cystitis where there is uncertainty; and b. Conduct a urine culture and sensitivity test for unresolved or recurrent cystitis.
The diagnosis of acute uncomplicated cystitis can be made solely on presenting signs and symptoms and history in most cases, and urine tests are generally not required unless there is uncertainty about the diagnosis. Table 2 summarises these urine tests, including information on when to test, findings that support the diagnosis, and other considerations. Figure 2 indicates when these tests should be considered, and the typical course of action based on the test results.
Urine dipstick
In patients with typical signs and symptoms of cystitis, urine dipstick tests are not necessary as they lead to minimal increase in diagnostic accuracy8 and are unlikely to alter management.10 However, if the diagnosis is unclear (e.g., patient only has one symptom), conducting a urine dipstick test can increase the likelihood of a cystitis diagnosis.8-10,17 In this instance, dipstick tests can help confirm the diagnosis of cystitis (in the context of urinary signs and symptoms)9,18 through the presence of one or more of the following:
Nitrite – detects presence of nitrate-reducing bacteria (including Enterobacterales which is the group of bacteria responsible for most UTIs). It is considered to be most predictive of bacteriuria, assuming infection is caused by a nitrate-reducing bacteria and has been retained in the bladder for more than four hours9,10
Leukocyte esterase (LE) – detects pyuria; produced by leukocytes, with levels increasing in response to infections9
Urine culture and sensitivity
Urine culture and sensitivity (C&S) is considered the gold standard test for patients presenting with signs and symptoms suggestive of UTI and helps to tailor antibiotic management based on the C&S results. However, in the context of diagnosing cystitis, urine C&S is normally not necessary except in cases of unresolved or recurrent cystitis. See Table 2 for further information.
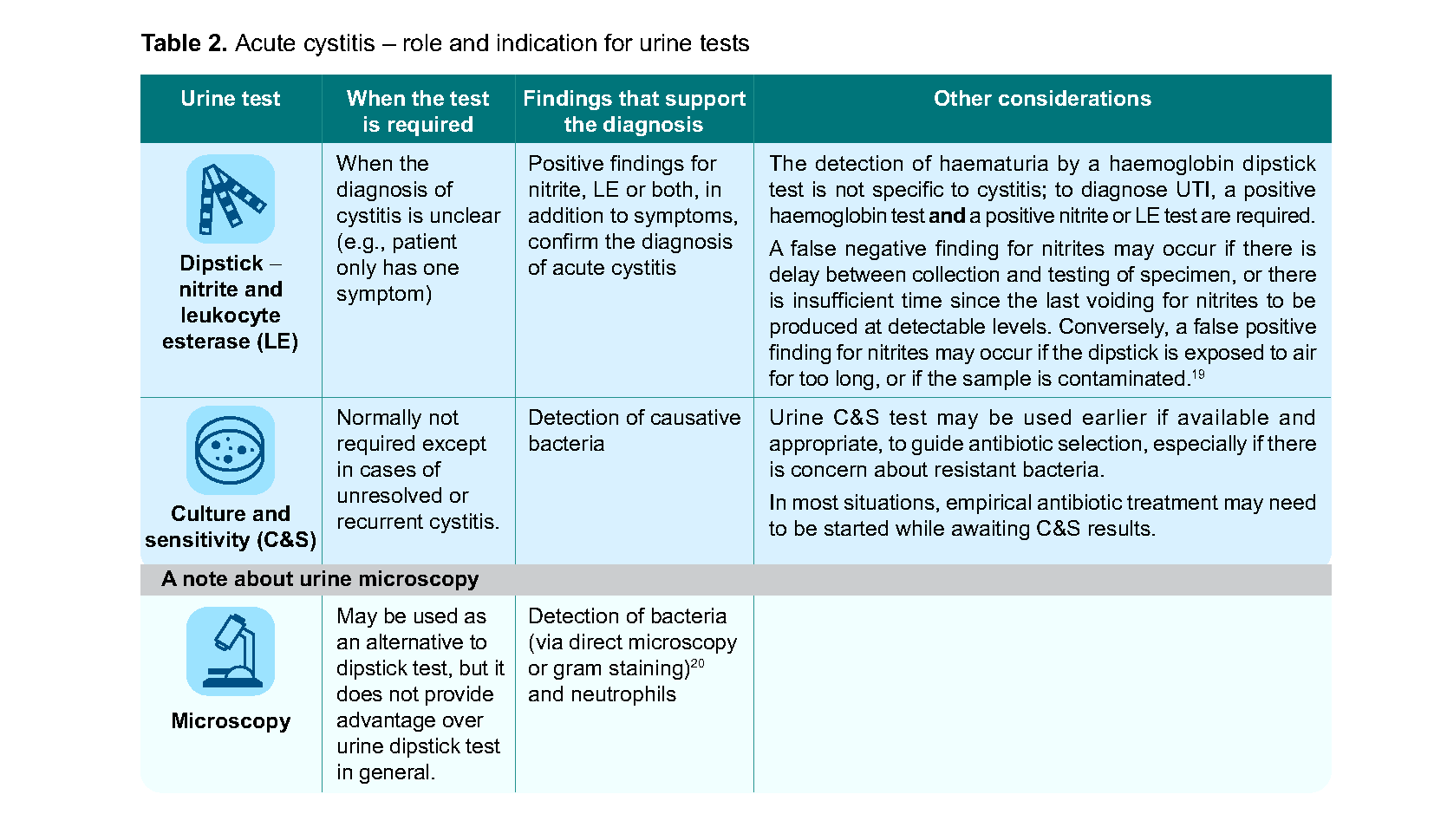
Table 2. Acute cystitis – role and indication for urine tests
Other populations |
|---|
Detection of bacteria (via direct microscopy or gram staining)20 and neutrophils Cystitis is much less common in men than in women.21 All occurrences of cystitis in men are considered to be ‘complicated’ and need further assessments. Therefore, a urine C&S test is recommended for all men presenting with signs and symptoms of cystitis, and antibiotic therapy should be tailored based on urine C&S results. |
In women with history of recurrent cystitis, where available, review previous urine C&S results and history of antibiotics used. Conduct urine C&S to guide management plan. |
Recommendation 4: Suspect uncomplicated pyelonephritis in patients presenting with sudden-onset flank pain or tenderness, particularly when accompanied by other systemic symptoms such as fever, nausea or vomiting.
Uncomplicated pyelonephritis is defined as a kidney infection in non-pregnant pre-menopausal women with no known relevant urological abnormalities or comorbidities.8 Unlike cystitis, the diagnosis of pyelonephritis cannot be made solely on presenting signs and symptoms, but these signs and symptoms may help to differentiate pyelonephritis from other clinical conditions (see Examples of differential diagnoses for patients presenting with sudden-onset flank pain or costovertebral tenderness).
The clinical presentation and severity of pyelonephritis can vary widely, and patients may present with different signs and symptoms,22 including the following (see Figure 2):
Systemic signs and symptoms (e.g., fever, chills, nausea, vomiting)23
Bladder symptoms (e.g., dysuria, frequency, urgency)22
Kidney signs and symptoms (e.g., acute-onset flank pain or costovertebral tenderness on palpation)24
While many of the listed signs and symptoms may not always be present, acute-onset flank pain or tenderness is found to be the most common symptom in patients with acute pyelonephritis,24 and the presence of this symptom (with accompanying pyuria or bacteriuria) is considered highly suggestive of pyelonephritis.10,22,25
Notepad: Examples of differential diagnoses for patients presenting with sudden-onset flank pain or costovertebral tenderness23,26
|
Acute pyelonephritis cases may be associated with moderate or severe complications such as sepsis or bacteraemia. Therefore, any suspicion of pyelonephritis needs to be confirmed quickly with further diagnostic tests (see Recommendation 5).
Recommendation 5: Conduct urine tests (dipstick or microscopy, plus culture and sensitivity) for all patients with suspected uncomplicated pyelonephritis to confirm diagnosis and guide management.
In patients with suspected uncomplicated pyelonephritis, urine tests are necessary to confirm the diagnosis, as well as to guide management. If urine dipstick or microscopy does not show any abnormalities, management should be guided by clinical judgement while awaiting the results from C&S. Table 3 summarises the role of urine tests and considerations to support the diagnosis. Figure 2 indicates when these tests should be conducted, and the typical course of action based on the test results.
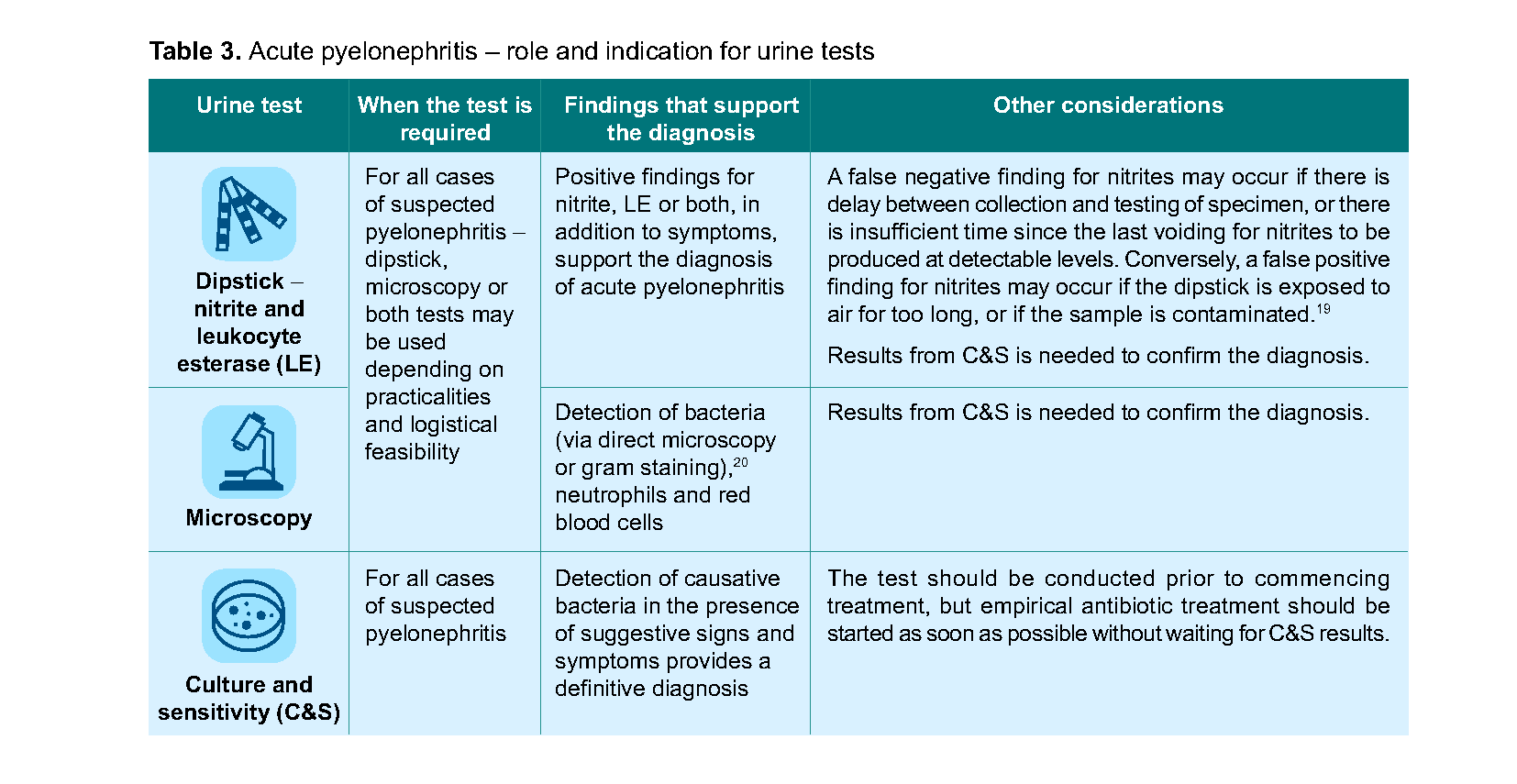
Table 3. Acute pyelonephritis – role and indication for urine tests
Notepad: Role of imaging in uncomplicated pyelonephritis Imaging (e.g., abdominal and pelvic CT with IV contrast) is not routinely indicated for the diagnosis of uncomplicated pyelonephritis.10,27 Examples of situations where imaging may be considered:
In some situations, where available and feasible, bedside abdominal ultrasound may be a useful adjunct in the evaluation of pyelonephritis (e.g., to detect ipsilateral hydronephrosis). |
Management of UTI
Treatment decision and selection of antibiotics
Antibiotics remain the mainstay of treatment for UTI. Treatment decision should include consideration of:28
Expected benefits of antibiotic treatment in reducing disease severity and duration, and reducing risk of developing complications due to non-treatment
Risks of antibiotic treatment (e.g., contributing to AMR problem; antibiotic-associated side effects, including diarrhoea)
The severity of the symptoms
Patient factors (e.g., allergy or intolerance to antibiotics, patient’s preference, and renal function)
When deciding on the most appropriate antibiotic, consider:
Local antimicrobial susceptibility or resistance data where available; the antibiotic recommendations in this ACG are mostly based on the susceptibility and resistance data for E. coli, the most common pathogen for UTI
Antibiotic spectrum of activity (with narrow-spectrum antibiotics generally preferred where possible to minimise the risk of antibiotic resistance)
Features of the antibiotics (e.g., efficacy at the site of infection, required dosing frequency, available dosage forms)
Availability and other factors which may affect patient adherence (e.g., potential side effects, cost)
In this ACG, most of the suggested antibiotics are oral antibiotics as they are commonly used and usually available in the primary care setting.
Recommendation 6: Prescribe nitrofurantoin empirically for uncomplicated cystitis; if nitrofurantoin is not suitable, prescribe amoxicillin-clavulanate or fosfomycin.
Compared to placebo, non-pregnant women with microbiologically confirmed acute uncomplicated cystitis who received antibiotics were more likely to have complete symptom resolution and microbiological success (defined as negative urine culture), and less likely to experience relapse after the end of treatment.29 Recommended empirical antibiotics for patients with acute uncomplicated cystitis include nitrofurantoin, or if not suitable, amoxicillin-clavulanate or fosfomycin.
Nitrofurantoin is preferred because it is effective against both gram-positive and gram-negative bacterial strains and it is indicated for treatment of lower UTI including uncomplicated cystitis. Resistance to nitrofurantoin remains relatively rare despite several decades of widespread use.30 Importantly, the local strain of E. coli remains highly susceptible to nitrofurantoin.4,5
Amoxicillin-clavulanate is an option for patients for whom nitrofurantoin is unsuitable or contraindicated. Amoxicillin-clavulanate is effective against most gram-positive and gram-negative bacterial strains causing community-acquired UTIs.31 It has a broader spectrum of activity and a higher incidence of gastrointestinal side effects than nitrofurantoin,32 hence the preference for nitrofurantoin.
Fosfomycin is another option for treatment of uncomplicated cystitis if nitrofurantoin is unsuitable. It is effective against E. coli.4,33 As a complete course only requires the administration of a single dose of medication, it may be a good option for patients who may have difficulty with medication adherence.
Information on suggested dosing and duration, common side effects and practice points are listed in Table 4.
Due to high levels of local resistance exhibited by E. coli to ciprofloxacin and co-trimoxazole, only use these medications for acute uncomplicated cystitis if supported by C&S results.4,5 |
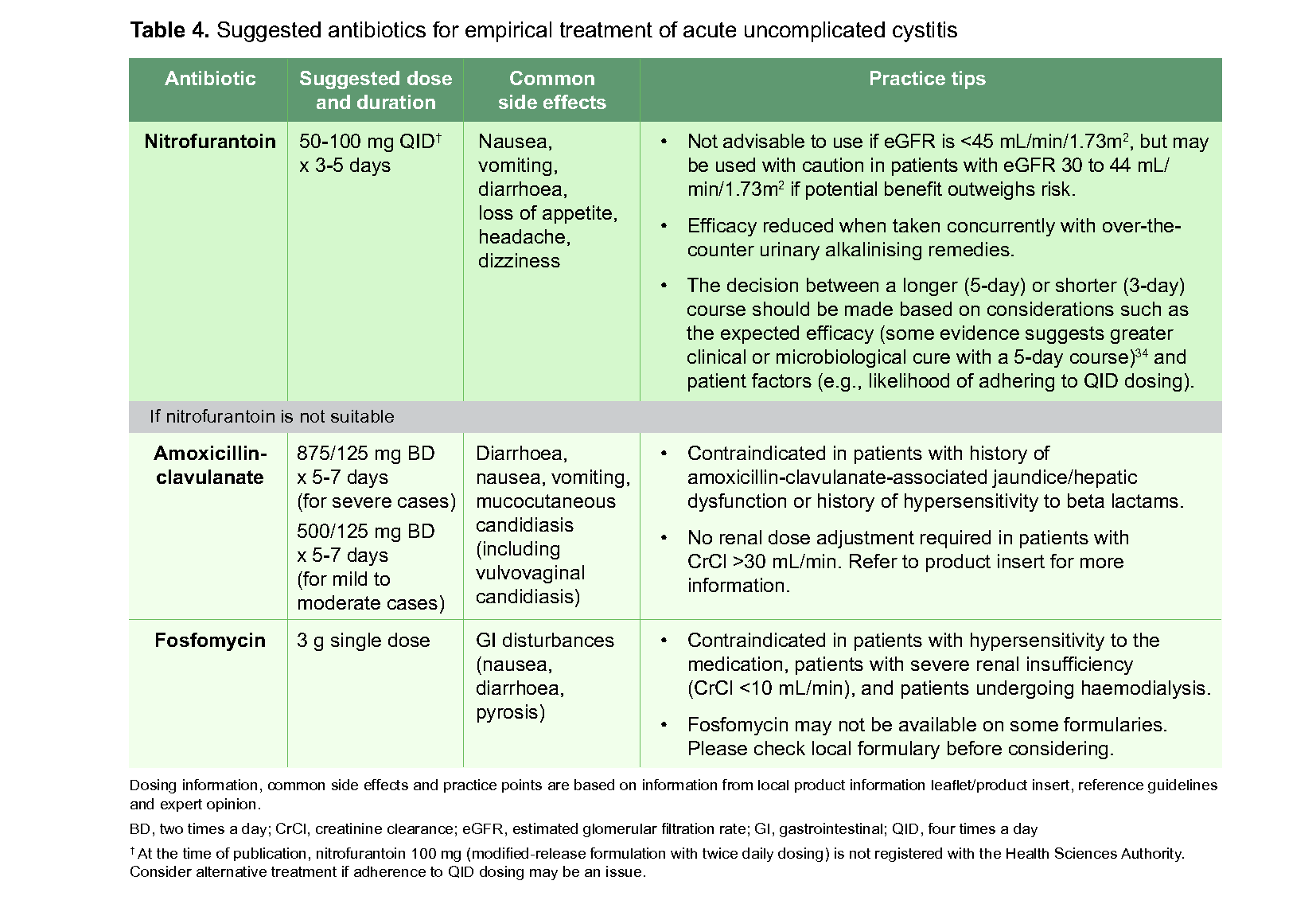
Table 4. Suggested antibiotics for empirical treatment of acute uncomplicated cystitis
Click here for larger version of the image
Notepad: Do NSAIDs play a role in acute uncomplicated cystitis? Nonsteroidal anti-inflammatory drugs (NSAIDs) may play a role in two different ways:
In both circumstances, consideration of NSAID use will also depend on the patient’s underlying comorbidities (e.g., may not be a suitable option for patients with renal impairment or gastrointestinal ulcers). |
Patient self-care
All patients with UTI should be encouraged to practise self-care and be informed of the appropriate and responsible use of antibiotics. See Patient self-care advice and Patient education on antibiotic use and antimicrobial resistance awareness for information and resources.
Notepad: Patient self-care advice | |
Encourage patients with UTIs to practise self-care. | |
Specific advice to support treatment plan:
| General advice to minimise recurrence:
|
Notepad: Patient education on antibiotic use and antimicrobial resistance awareness | |
Good antimicrobial stewardship includes using antibiotics responsibly and appropriately. | |
Remind patients prescribed antibiotics to:
| Examples of useful patient resources on antimicrobial stewardship: |
While most cases of uncomplicated cystitis are self-limiting and will resolve with appropriate pharmacological and non-pharmacological treatment, there may be instances when a referral to a specialist may be needed (see Considerations for referral under Recommendation 7).
Other populations |
Consider a much longer duration of antibiotic therapy (e.g., a 14-day course) when treating lower UTI in men.36 UTIs in men are less common than women because in men, there is a longer distance from the urethra and anus to the kidney, hence a lower likelihood of ascending infections. Men are also less subjected to hormonal changes. However, once affected, it is considered to be complicated and requires a longer course of antibiotic therapy due to higher risk of treatment failure.23 Nitrofurantoin may not be a suitable treatment option for men with suspected prostate involvement (i.e. prostatitis) as this medication is unlikely to reach therapeutic levels in the prostate. Further assessments or referral to a specialist may be needed in such patients (see Considerations for referral under Recommendation 7). |
Recommendation 7: Prescribe amoxicillin-clavulanate empirically for patients with uncomplicated pyelonephritis and tailor antibiotic choice accordingly when urine culture and sensitivity results are available; if amoxicillin-clavulanate is not suitable, consider cefuroxime as an alternative.
In patients with acute uncomplicated pyelonephritis, start empirical treatment with oral antibiotics as soon as possible after conducting a urine C&S (see Recommendation 5), and tailor treatment based on C&S results.8 Antibiotics that do not reach therapeutic concentrations in renal tissue (such as nitrofurantoin and fosfomycin) play a limited role in the management of acute uncomplicated pyelonephritis and should not be used.8,10
For patients with acute uncomplicated pyelonephritis, the following antibiotics are recommended mainly based on local E. coli susceptibility and resistance data,4,5 as well as the efficacy of the medication at the target tissue:
Oral amoxicillin-clavulanate is recommended as initial empirical treatment in patients with acute uncomplicated pyelonephritis, with therapy tailored accordingly based on C&S results.
Cefuroxime may be considered as an alternative if amoxicillin-clavulanate is not a suitable option (e.g., issues with tolerability or side effects). In the primary care setting, it is expected that oral cefuroxime (cefuroxime axetil) will be more readily available. (See note about parenteral antibiotics in Table 5).
The general guidance on the recommended empirical antibiotics for patients with acute uncomplicated pyelonephritis are provided in Table 5.
Ciprofloxacin and co-trimoxazole can be effective medications for the treatment of pyelonephritis. However, due to high levels of local resistance exhibited by E. coli to ciprofloxacin and co-trimoxazole, only use these medications for acute uncomplicated pyelonephritis if supported by C&S results.4,5 |
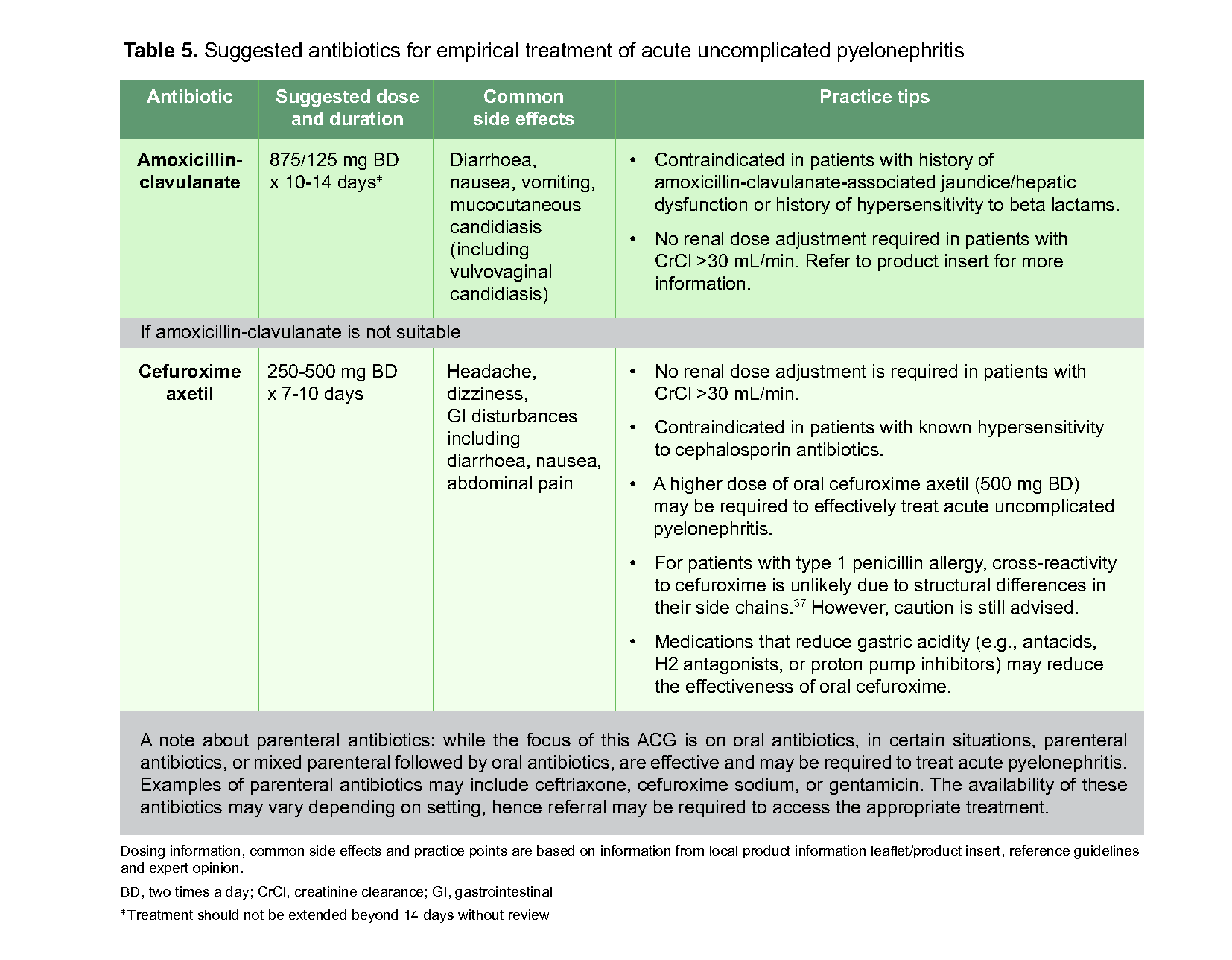
Table 5. Suggested antibiotics for empirical treatment of acute uncomplicated pyelonephritis
Click here for larger version of the image
Patient self-care and education on antibiotic use complement antibiotic treatment of uncomplicated pyelonephritis. See Patient self-care advice and Patient education on antibiotic use and antimicrobial resistance awareness in Recommendation 6.
Patients with complicated pyelonephritis with associated risks factors or underlying comorbid conditions may require hospital admission or further investigations. See Figure 2 for conditions that need immediate referral and below for other considerations for referral.
Notepad: Considerations for referral Examples of patient factors which may prompt referral:
|
Expert group
Chairperson
A/Prof David Michael Allen, Infectious Disease Medicine, NUH
Members
Dr Sky Koh Wei Chee, Family Medicine, NUP
A/Prof Piotr Chlebicki, Infectious Disease Medicine, SGH
Asst Prof David Terrence Consigliere, Urology, NUH
Dr Khong Haojun, Family Medicine, NHGP
Dr Asok Kurup, Infectious Disease Medicine, Infectious Diseases Care Pte Ltd
Dr Kwek Thiam Soo, Family Medicine, Bukit Batok Medical Clinic (NUHS PCN)
Ms Lee Yu Jie, Pharmacy, SHP
Dr Moey Kirm Seng Peter, Family Medicine, SHP
Dr Ng Juak Cher, Family Medicine, Raffles Medical Group Tampines (Raffles Medical PCN)
Dr Ng Tat Ming, Pharmacy, TTSH
Dr Wong Wei Chin, Geriatric Medicine, TTSH
Dr Jonathan Yeo Cheng Hsun, Family Medicine, FMC Chinatown (I-Care PCN)
Collaborating organisation
ACE would like to acknowledge the support and assistance from the Antimicrobial Resistance Coordinating Office, National Centre for Infectious Diseases (AMRCO, NCID) in the development of this ACE Clinical Guideline.

Feedback
Click here to give us feedback on this ACG.
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Urinary tract infections – appropriate diagnosis and antibiotic use for uncomplicated cystitis and pyelonephritis. ACE Clinical Guideline (ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-uti-appropriate-diagnosis-and-antibiotic-use
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.