
Managing pre-diabetes — a growing health concern ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) covers diagnosis and management of pre-diabetes, with a focus on lifestyle intervention (including diet and physical activity) and pharmacotherapy.
First published in 2017, this ACG has been updated in 2021 to incorporate the latest evidence where relevant.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG recommendations
Pre-diabetes is asymptomatic but puts a person at high risk of developing type 2 diabetes mellitus (T2DM) and cardiovascular disease (CVD).
Early diagnosis, appropriate management and follow-up help to prevent or delay T2DM in persons with pre-diabetes.
Recommend lifestyle intervention to all persons with pre-diabetes.
Tailor lifestyle intervention to individual needs for sustained behavioural changes.
Consider metformin for persons with pre-diabetes when
glycaemic status does not improve despite lifestyle intervention OR
they are unable to adopt lifestyle intervention,
especially if the persons outlined in the two points above have a body mass index (BMI) of ≥ 23 kg/m2, are younger than 60 years of age, or are women with a history of gestational diabetes.
Download the ACG and references in PDF
Managing pre-diabetes - a growing health concern (Jul 2021) [PDF]
Managing pre-diabetes - a growing health concern references (Jul 2021) [PDF]
Dec 2023 update: practice tips in Table 4 for nitrofurantoin and fosfomycin for treatment of acute uncomplicated cystitis have been updated.
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Preventing or delaying the progression to T2DM
Pre-diabetes is defined by glycaemic levels that are higher than normal, but lower than diabetes thresholds. Pre-diabetes is asymptomatic but predisposes individuals to T2DM and CVD. Around 14% of Singaporeans have impaired glucose tolerance and without lifestyle changes, at least 35% of persons with pre-diabetes in Singapore will progress to T2DM within eight years.1,2 There is a pressing need to address pre-diabetes as part of the efforts to reduce the impact of T2DM and CVD.
Education increases awareness of pre-diabetes and enables individuals to adopt lifestyle changes.
Diagnosis of pre-diabetes
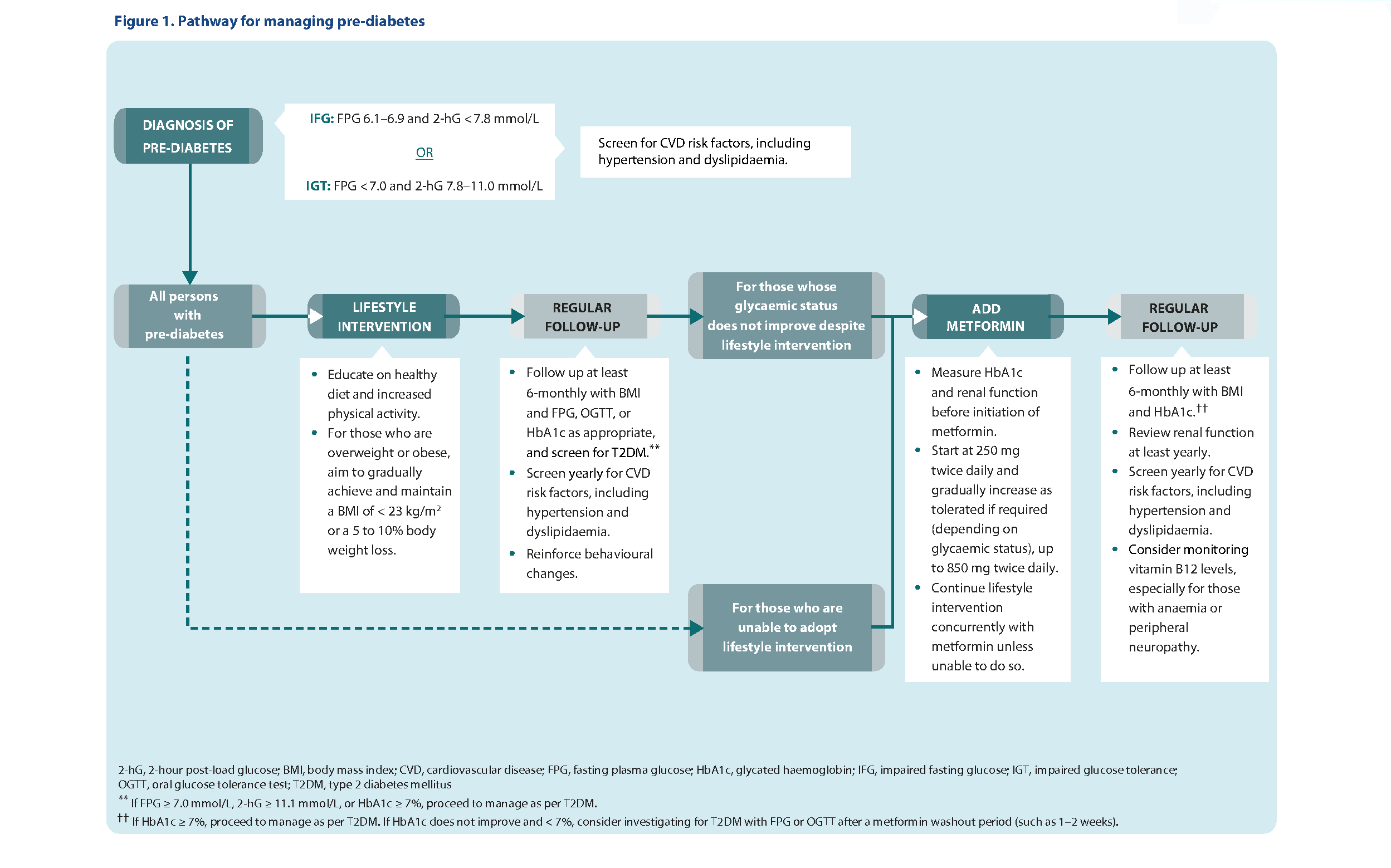
In Singapore, glucose thresholds in Table 1 below are used to diagnose pre-diabetes (impaired fasting glucose or impaired glucose tolerance).
Table 1. Glucose thresholds for pre-diabetes
Pre-diabetes | Fasting plasma glucose (mmol/L) | 2-hr post-load glucose (mmol/L)* |
|---|---|---|
IFG | 6.1–6.9 | < 7.8 |
IGT | < 7.0 | 7.8–11.0 |
IFG, impaired fasting glucose; IGT, impaired glucose tolerance
In Singapore, glycated haemoglobin (HbA1c) is not currently indicated as a diagnostic test for pre-diabetes.†
Lifestyle intervention
Lifestyle intervention is recommended for all persons with pre-diabetes, as adopting healthy diet and increased physical activity reduces the risk of them developing T2DM by 31 to 37% over 2 to 6 years, and is cost-effective.3-5
For those who are overweight or obese, aim to gradually achieve and maintain a BMI of < 23 kg/m2 or a 5 to 10% body weight loss.
Smokers are advised to stop smoking, as smoking impairs glucose metabolism, insulin sensitivity and secretion.6
Healthy diet
A healthy and balanced diet plays a key role in preventing or delaying the progression to T2DM in persons with pre-diabetes.7-12
Advise those who are overweight or obese to achieve weight loss by implementing a negative caloric balance.
Increased physical activity
Obesity and a sedentary lifestyle are major risk factors for developing T2DM and can be modified by an increase in physical activity.7-12
Pedometers or fitness trackers allow progress to be monitored over time and may provide additional motivation.13
Instructions on lifestyle intervention Convey the following points to persons with pre-diabetes during consultations. Healthy diet Portion a healthy plate
Avoid sweetened beverages and foods
Eat less fat
Limit alcohol intake
Increased physical activity
|
* 2-hour 75-g oral glucose tolerance test (OGTT).
†For more information on HbA1c as a screening test for diabetes mellitus in Singapore, please refer to the Ministry of Health Circular No. 08/2019.
‡ A standard drink is one can (330 mL) of beer, half a glass (100 mL) of wine, or one nip (30 mL) of spirits or hard liquor.
Sustained behavioural changes
Providing information without individualised advice may not be sufficient to bring about robust and sustained lifestyle changes. Lifestyle intervention should therefore be tailored to each person’s needs and continuously encouraged.14
Tailor lifestyle intervention to individual needs
Assess lifestyle (such as diet and physical activity preferences, work nature, physical or budget constraints).
Identify areas for improvement towards a healthier lifestyle.
Provide advice on practical and sustainable lifestyle changes that fit into daily activities.
Reinforce behavioural changes continuously
Encourage persons with pre-diabetes to keep a log of their diet, exercise, and weight.
Advise them to visit the HealthHub website to find out more about pre-diabetes and associated lifestyle change programmes. They can also download the HealthHub SG and HealthHub Track applications (App Store or Google Play Store).
Supplement verbal advice with written information.
Click here to access pre-diabetes information on the HealthHub website.
Pharmacotherapy
Pharmacotherapy for pre-diabetes is less effective than lifestyle changes and may be considered after a trial of intensive lifestyle intervention.9,15 Discuss the benefits, side effects, and cost before commencing treatment.
Metformin is the drug of choice as it has the strongest evidence and the longest safety data.4,16 It has been shown to reduce the incidence of T2DM in persons with pre-diabetes by 26% over three years.3
Acarbose§ has shown a favourable trend in preventing or delaying T2DM in pre-diabetes.17 However, the evidence for acarbose is not as robust or well-studied as for metformin. Consider acarbose only when metformin is not well-tolerated. Acarbose acts mainly by decreasing postprandial glucose. Hence, its glucose-lowering effect is more likely to benefit persons with IGT and not IFG alone.18
Indication, dosing regimen, and side effects of metformin for pre-diabetes
Consider metformin for persons with pre-diabetes when
glycaemic status does not improve despite lifestyle intervention OR
they are unable to adopt lifestyle intervention,
especially if persons outlined in the two points above have a BMI of ≥ 23 kg/m2, are younger than 60 years of age, or are women with a history of gestational diabetes.
Start metformin at 250 mg twice daily and gradually increase as tolerated if required (depending on glycaemic status), up to 850 mg twice daily.
Take metformin with meals to reduce side effects such as nausea, vomiting, or diarrhoea.
§Off-label for pre-diabetes; locally registered as additional therapy in association with diet in patients with diabetes mellitus.
Overview of lifestyle intervention in pre-diabetes
Role of lifestyle intervention
Lifestyle intervention reduces the risk of developing T2DM by 31 to 37% over 2 to 6 years
For those who are overweight or obese, aim to gradually achieve and maintain a BMI of < 23 kg/m2 or a 5 to 10% body weight loss
Ways to implement lifestyle intervention
How to sustain lifestyle changes
Expert group
Lead discussant
Dr. Phua Eng Joo (KTPH)
Chairperson
Dr. Darren Seah (NHGP)
Group members
Ms. Debra Chan (TTSH)
A/Prof. Goh Su-Yen (SGH)
Dr. Khoo Chin Meng (NUHS)
Prof. Joyce Lee (UC Irvine)
Ms. Lee Hwee Khim (SHP)
Dr. Lim Hui Ling (International Medical Clinic)
Ms. Ng Soh Mui (NUP)
Dr. Gilbert Tan (SHP)
Dr. Tham Tat Yean (Frontier Healthcare Group)
Ms. Pauline Xie (NHGP)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Type 2 diabetes mellitus – personalising management with non-insulin medications
Initiating basal insulin in type 2 diabetes mellitus
Foot assessment in people with diabetes mellitus
Gestational diabetes mellitus — an update on screening, diagnosis, and follow-up
Managing pre-diabetes — beyond guidelines for better outcomes
Diabetic Retinal Photography (DRP) Screening Technical Reference Guide
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Managing pre-diabetes – a growing health concern. Appropriate Care Guide (ACG), Ministry of Health, Singapore. 2021. Available from: go.gov.sg/acg-managing-pre-diabetes-a-growing-health-concern
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.