
Type 2 diabetes mellitus — personalising management with non-insulin medications ACG
Last updated 16 June 2026
Overview
This ACE Clinical Guideline (ACG) focuses on optimising management of type 2 diabetes mellitus (T2DM) by personalising selection of non-insulin T2DM medications based on patient comorbidities and risk factors, in particular cardiovascular and renal factors.
This ACG replaces the 2017 ACG “Oral glucose-lowering agents in type 2 diabetes mellitus – an update”.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Assess the patient’s glycaemic control and risk of adverse cardiorenal outcomes.
Select and adjust T2DM medication(s) based on the patient’s glycaemic control and their risk of adverse cardiorenal outcomes.
Consider metformin as first-line T2DM medication.
Consider prescribing an SGLT2 inhibitor or GLP-1 RA for patients with T2DM who need to reduce their risk of adverse cardiorenal outcomes.
Adopt a patient-centred approach to make shared decisions on T2DM management.
Educate patients with T2DM on sustained lifestyle intervention, medication adherence, and regular review.
Review all patients with T2DM regularly, including treatment response and complication screening.
Download the ACG and references in PDF
T2DM – personalising management [PDF, 1.6 KB]
T2DM – personalising management references [PDF, 145 KB]
T2DM – personalising management useful resources [PDF, 10 KB}
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
An estimated 537 million adults aged 20 to 79 years—that is 1 in 10 adults—are living with diabetes.1 For the past three decades, diabetes has been one of the top ten drivers of increasing mortality and burden of disease worldwide.2 In Singapore, diabetes was the sixth leading cause of mortality and burden of disease combined (in 2019).3 The National Population Health Survey (2019-2020) reports that 9.5% of residents aged 18 to 74 had diabetes mellitus. Of those who self-reported having diabetes and attended the survey-related health examination, a quarter had poor glycaemic control.4
More than 95% of people with diabetes have type 2 diabetes mellitus (T2DM).5 Since 2015, the publication of clinical trials demonstrating the cardiovascular and renal benefits of some newer classes of T2DM medications have changed the approach to managing T2DM. However, in Singapore, despite the increasing availability of such medications, metformin and sulphonylureas continue to be the main medications used by patients with T2DM. Thus, in line with international recommendations, this ACG encourages healthcare professionals to optimise management of T2DM by personalising selection of non-insulin T2DM medications based on patient comorbidities and risk factors, in particular cardiovascular and renal factors.
Clinical needs assessment
Recommendation 1: Assess the patient’s glycaemic control and risk of adverse cardiorenal outcomes.
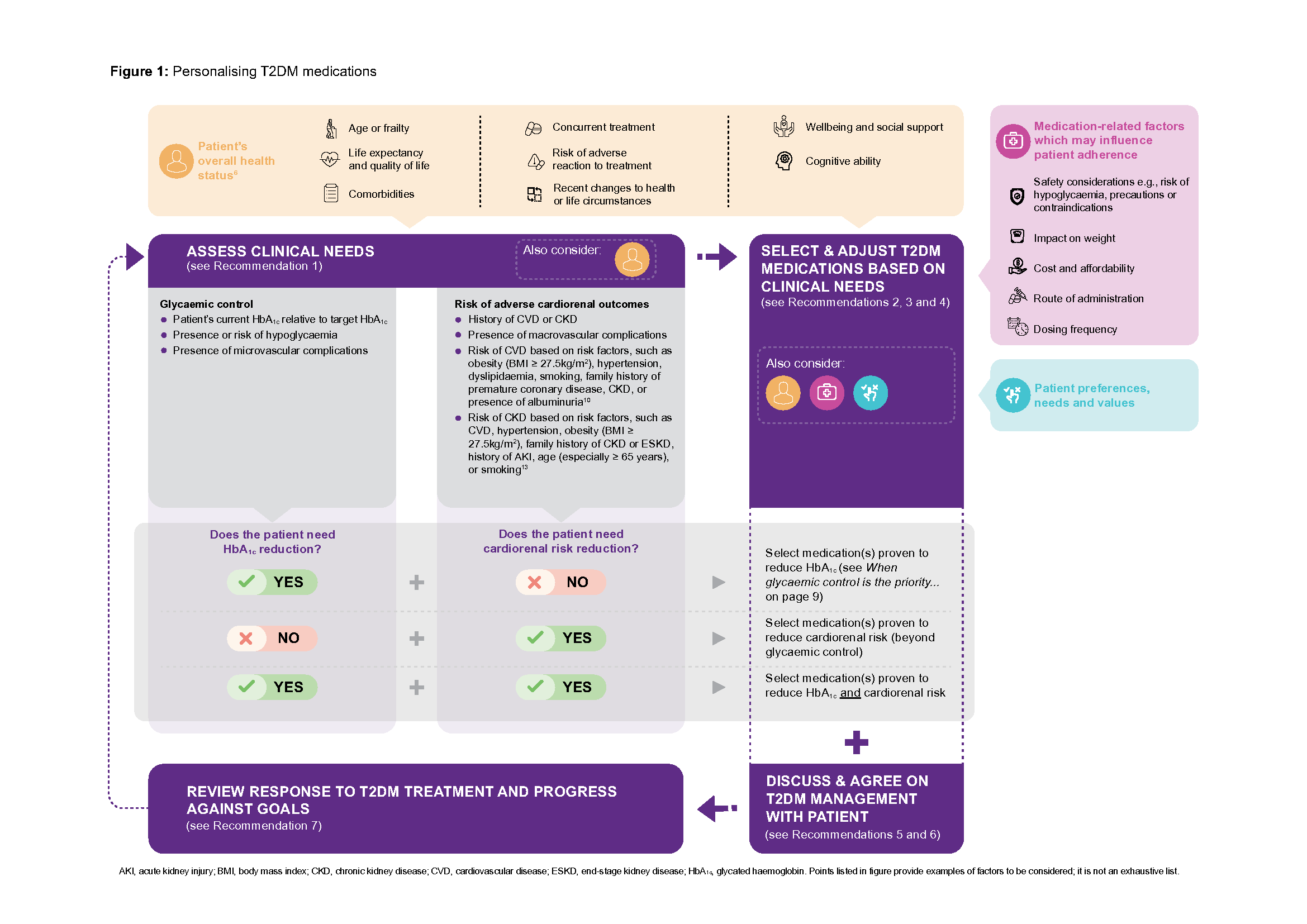
Assessment of a patient’s glycaemic control and their risk of adverse cardiorenal outcomes is critical to guide appropriate T2DM treatment, given their significant impact on diabetes morbidity and mortality. In this ACG, these two areas—glycaemic control, and risk of adverse cardiorenal outcomes—are referred to as the patient’s ‘clinical needs’.
For patients with newly diagnosed T2DM, assess their clinical needs before discussing and deciding about appropriate treatment. For ongoing patients, reassess the patient’s clinical needs against their current management goals and response. In both cases, complement this assessment with an evaluation of the patient’s overall health status (see Figure 1 Patient’s overall health status).
Glycaemic control
The goal of T2DM management is to prevent or delay diabetes-related complications while improving the quality of life of patients.6 A core part of this has been, and still remains, maintaining good glycaemic control in order to reduce the risk of microvascular complications.
Notepad: Glycated haemoglobin (HbA1c) target Target HbA1c should be individualised based on the patient’s overall health status, in consultation with the patient. For most patients, a target HbA1c of ≤7.0% provides a reasonable balance between a reduction in risk of microvascular complications and risk of hypoglycaemia. Examples of when a more stringent HbA1c target (e.g., ≤6.5%) may be appropriate:7,8
Examples of when a less stringent HbA1c target (e.g., ≤8.0%) may be appropriate:7,8
|
Risk of adverse cardiorenal outcomes
Patients with diabetes are at increased risk of developing cardiovascular disease (CVD),9 with atherosclerotic cardiovascular disease (ASCVD) being the leading cause of morbidity and mortality for patients with diabetes.10 Related to CVD is the association between diabetes and increased rate of hospitalisation for heart failure.10 In addition, patients with diabetes may also develop kidney-related complications, with diabetic kidney disease being the most common cause of end-stage kidney disease (ESKD).11 The increased risk for progression to ESKD is concomitantly accompanied by an increased risk of cardiovascular morbidity and mortality.11,12 Hence, cardiorenal risk reduction is also a critical consideration for patients with T2DM, particularly now that there are T2DM medications which have been shown to reduce this risk (see Recommendation 4).
Click here for larger version of the image
Pharmacological treatment
Diabetes medications play a key role in managing T2DM for most if not all patients. Importantly, medications are to be used in conjunction with lifestyle intervention. Patients may require medications soon after diagnosis, or after a period (e.g., 3 to 6 months) of lifestyle intervention alone. This ACG focuses on personalising non-insulin T2DM medications, acknowledging that insulin still has an important role in the management of T2DM.
Notepad: Lifestyle intervention: a cornerstone of successful T2DM management All international guidelines advocate lifestyle intervention as essential to prevent and manage T2DM.14-20 A healthy lifestyle can have direct impact on glycaemic control and CVD risk,7,19 with the latter being a major cause of mortality among patients with T2DM.21 In particular, even moderate weight loss (5% of body weight) in patients who are overweight or obese can decrease insulin resistance, improve glycaemic control, reduce the need for T2DM medications, and reduce the risk of CVD.22,23 For patients with chronic kidney disease (CKD) who are overweight or obese, weight loss is also associated with a reduction in albuminuria and proteinuria.24,25 Many local resources and programs provide information to encourage those at risk of T2DM or living with T2DM to adopt a healthy lifestyle, including:26-28
Examples of patient resources and programs include Guide to Healthy Eating for Managing Diabetes Mellitus, Let’s B.E.A.T. Diabetes or 3 Be’s to Beat Diabetes (National Diabetes Reference Materials). |
Notepad: Insulin and T2DM Many patients with T2DM may require and benefit from insulin therapy. When clinically indicated, insulin therapy should be commenced without delay. Typically, insulin therapy is started when patients are unable to reach their glycaemic targets despite optimal treatment with non-insulin T2DM medications alone, or for those with symptomatic hyperglycaemia.29 Appropriate weight management and other lifestyle interventions remain important. Insulin therapy is usually introduced by initiating basal insulin (intermediate- or long-acting insulin). When starting insulin therapy, review concomitant T2DM medications and continue where appropriate; and educate patients and their carers about preventing and managing hypoglycaemia. For further information, see ACG on Initiating basal insulin in type 2 diabetes mellitus. |
Recommendation 2: Select and adjust T2DM medication(s) based on the patient’s glycaemic control and their risk of adverse cardiorenal outcomes.
Dual focus in T2DM management
The focus on glycaemic control and risk of adverse cardiorenal outcomes continues into T2DM management, with these clinical needs underpinning T2DM medication selection. This approach represents a significant shift from centering treatment decisions solely on achieving glycaemic control, with recent major international guidelines all recommending reduction of cardiorenal risk as an equally important focus of T2DM management.14-20
Other considerations for T2DM medication selection
In addition to clinical needs, other factors that should be considered in the medication selection process (see Figure 1 on page 3) include:
the patient’s overall health status;
medication-related factors which may influence patient adherence; further information about these factors can be found in a clinician infographic, Type 2 diabetes mellitus – personalising management with non insulin diabetes medications (see Useful resources on page 12);
the patient’s preferences, needs and values (see Recommendation 5 on page 9).
For example, consider two hypothetical scenarios involving two 55-year-old patients newly diagnosed with T2DM.
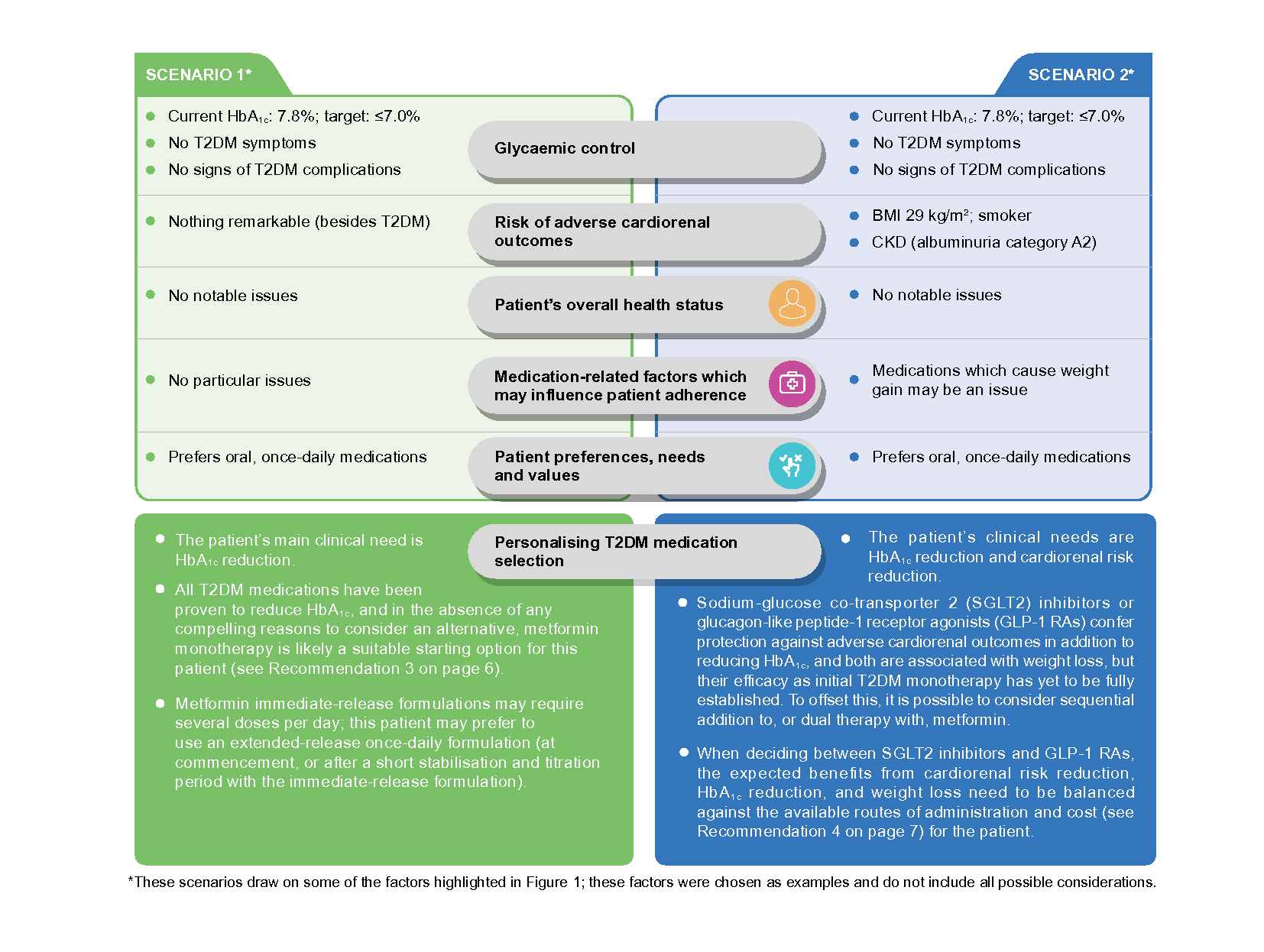
In both scenarios, all the above-mentioned factors should be discussed with the patient to determine the most appropriate medication(s) for the patient’s current situation. There may be additional considerations that may not have been previously discussed or warrants revisiting (e.g., in Scenario 2, it is worth clarifying the patient’s circumstances and preferences in relation to the cost of treatment).
Recommendation 3: Consider metformin as first-line T2DM medication.
Benefits of metformin
Metformin remains a good initial treatment choice for most patients with T2DM, alongside comprehensive lifestyle intervention.15-17,20 Metformin is effective in reducing HbA1c30,31 and some evidence suggests metformin may reduce the risk of cardiovascular events and death.14,19,32,33 The favourable efficacy profile, accompanied by its neutral effects on body weight and low risk of hypoglycaemia,14,17,34 long-term safety record, wide availability and low cost, make metformin an appropriate and feasible treatment foundation for most patients with T2DM.
In patients with contraindication or intolerance to metformin [e.g., if estimated glomerular filtration rate (eGFR) <30 mL/ min/1.73m2], the choice of first-line T2DM medication should follow the considerations outlined in Figure 1.30
Notepad: Managing the gastrointestinal side effects of metformin Common concerns about potential side effects with metformin, particularly gastrointestinal side effects, can usually be minimised or managed by:
|
Comparison to other T2DM medications as monotherapy
Metformin compares well to sulphonylureas in terms of relative effectiveness and safety. Both reduce HbA1c to a similar extent, but sulphonylureas are associated with greater weight gain and higher risk of hypoglycaemia.30,35 Little systematic data is available for comparisons with newer T2DM medication classes especially as first-line treatment.
Most international guidelines support the use of metformin as first-line T2DM medication. However, a few suggest that SGLT2 inhibitors or GLP-1 RAs may also be appropriate initial medications for patients with T2DM with or at high risk of developing ASCVD, heart failure or CKD. This is based on growing evidence of the benefits of these classes of medications in cardiorenal risk reduction and on limited post-hoc subgroup analyses observing that these benefits may be independent of metformin use.14,36 As most primary studies for SGLT2 inhibitors and GLP-1 RAs generally involved patients who were taking other concurrent medications [mostly metformin – see Cardiovascular outcome trials (CVOTs) on page 7], the efficacy of these newer medications as monotherapy has yet to be fully established.b
Consideration for starting with dual therapy
Commencing treatment with monotherapy facilitates the monitoring of beneficial and adverse effects of the new medication. Patients should be reviewed (e.g., after three months) for treatment response and titration.
Initial dual therapyb may be considered for patients in certain situations, for example, for those in whom monotherapy is not expected to be sufficient, or when initial HbA1c is 1.5% or more above target. Some international guidelines echo this, recommending dual therapy for example in patients with higher initial HbA1c to increase likelihood of reaching treatment target17 and due to potential benefits in more rapid attainment of glycaemic targets;14 or given benefits offered by another medication independent of their effect on HbA1c.12,15 For example, recent meta-analyses have shown significant HbA1c reductions and similar hypoglycaemia risk for dipeptidyl peptidase-4 inhibitors (DPP4 inhibitors) or SGLT2 inhibitors in combination with metformin, compared to metformin alone.37,38
a Cost and affordability need to be discussed with the patient as the extended-release formulations are more expensive (compared to immediate-release formulations) and are not currently included in government subsidy lists.
b The evidence in relation to recommended first-line treatment and the role of initial dual therapy in T2DM is expected to continually evolve. ACE will continue to monitor for any significant changes after the publication of this ACE Clinical Guidance.
Recommendation 4: Consider prescribing an SGLT2 inhibitor or GLP-1 RA for patients with T2DM who need to reduce their risk of adverse cardiorenal outcomes.
Cardiorenal benefits of SGLT2 inhibitors and GLP-1 RAs
Cardiovascular outcome trials (CVOTs) report cardiorenal benefits associated with these two classes of T2DM medications in addition to improvements in glycaemic control.
In Singapore, registered SGLT2 inhibitors include canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin. Registered GLP-1 RAs include dulaglutide, liraglutide, lixisenatide,c and semaglutide. In summary, at a class level, for the following key endpoints:
Reducing major adverse cardiovascular events
SGLT2 inhibitors39-42 and GLP-1 RAs41-44 both significantly reduce the risk of major adverse cardiovascular events [composite endpoint of CV death, non-fatal myocardial infarction (MI), or non-fatal stroke], CV death and death from any cause.
GLP-1 RAs significantly reduce the risk of non-fatal stroke but not non-fatal MI43,44 while the converse was true for SGLT2 inhibitors.40
Reducing hospitalisation for heart failure
SGLT2 inhibitors39-42 and GLP-1 RAs41-44 both significantly reduce the risk of hospitalisation for heart failure, with SGLT2 inhibitors showing a larger effect.41,45
Reducing adverse renal outcomes
SGLT2 inhibitors39,41,42 and GLP-1 RAs41,42,44,46 both significantly reduce the risk of adverse renal outcomes [composite endpoint with varying definitions depending on study, e.g., doubling of serum creatinine level, new-onset macroalbuminuria, ≥40% decrease in eGFR, progression to ESKD, or death from renal causes], with SGLT2 inhibitors showing a larger effect;41,45 the renal benefit of GLP-1 RAs is driven by a reduction in macroalbuminuria alone, without any significant reduction in hard endpoints of renal function (eGFR, doubling of serum creatinine, and progression to ESKD).46
For information on the reported benefits of individual SGLT2 inhibitors and GLP-1 RAs for each of the above mentioned endpoints, refer to the clinician infographic (see Useful resources).
Notepad: Cardiovascular outcome trials (CVOTs) CVOTs have been mandated by the United States Food and Drug Administration since 2008 to evaluate cardiovascular safety of new T2DM medications. CVOTs involving DPP-4 inhibitors, SGLT2 inhibitors and GLP-1 RAs have demonstrated the cardiovascular safety of these classes (with the exception of saxagliptin which is associated with a significant increase in risk of hospitalisation for heart failure47). SGLT2 inhibitors and GLP-1 RAs have demonstrated cardiorenal benefits against placebo. While these studies have had a significant impact on the clinical treatment of T2DM, it is important to note, as with all clinical trials, the study’s primary intent, inclusions and parameters, which may affect the applicability of the findings to the wider T2DM population. Generally, at the time of study enrolment, most patients had a mean HbA1c between 6.6% and 8.7% and were already taking other T2DM medications (mostly metformin). Different studies included patients at different levels of risk for a cardiorenal event, with most patients having existing ASCVD, T2DM duration greater than 10 years, or a BMI in the overweight or obese category; some studies also included patients with or without heart failure and renal impairment. Several endpoints were reported, with differences in reported endpoints or endpoint definitions between studies. |
c Not available as single-ingredient product; only available in combination with insulin.
Patients requiring cardiorenal risk reduction
There is general agreement that patients with T2DM who have established ASCVD, heart failure or CKD would benefit from the cardiorenal risk reduction offered by SGLT2 inhibitors or GLP-1 RAs, independent of HbA1c levels. For those without established disease, the decision to reduce cardiorenal risk needs to be made on an individual basis, considering the patient’s risk factors (see examples in Figure 1).
Other considerations before prescribing SGLT2 inhibitors or GLP-1 RAs
In addition to considering their cardiorenal benefits, the decision on the most appropriate medication for an individual patient must include consideration of the factors mentioned in Figure 1. For SGLT2 inhibitors and GLP-1 RAs, discussion with the patient should include the following:
Safety considerationsd Risk of hypoglycaemia
Precautions SGLT2 inhibitors:
GLP-1 RAs:
|
Impact on weightd
|
Cost and affordabilityd
|
Route of administration and dosing frequencyd
|
d Further information can be found in the medication table, Non-insulin type 2 diabetes medications in Singapore (see Useful resources); refer to individual product inserts for full details, including side effects of individual medications.
Notepad: When glycaemic control is the priority... All T2DM medications, including insulin, have been shown to reduce HbA1c levels. When used as add on therapy to metformin, all T2DM medications show beneficial glucose-lowering efficacy compared to placebo.31 When improved glycaemic control is a treatment priority, in addition to considering the desired treatment target and the glucose-lowering effects of the medication, personalise selection of a medication for an individual patient by considering the other factors listed in Figure 1. For example:
Refer to the clinician infographic and medication table to inform prescribing decisions (see Useful resources). |
Patient involvement and education
Recommendation 5: Adopt a patient-centred approach to make shared decisions on T2DM management.
Healthcare professionals are encouraged to adopt a patient-centred approach6,15 which involves engaging the patient in a tailored discussion about their T2DM and its management. Below are practical examples of a patient-centred approach when discussing T2DM management with patients.
Areas of discussion | Examples of patient-centred approach |
|---|---|
Progressive nature of T2DM, its impact on the patient’s other comorbidities and their health; prognosis and management goals. | Check the patient’s understanding about their condition. Ask about the patient’s priorities in relation to T2DM in the context of their overall health, and what they hope to achieve. Encourage the patient to ask questions. |
Patient’s central role and the importance of being actively involved in their T2DM management. | Gauge the patient’s interest and motivation to engage in self-management. Encourage the patient to receive complementary care from multiple healthcare professionals and check that this is feasible. |
Available treatment options (including lifestyle intervention and insulin), how and when they fit into the overall management, and their benefits and risks. | Ask the patient about their preferences and seek their input on decisions relating to their treatment. Ascertain the patient’s knowledge about their treatment and ensure they have the correct information to adhere to the agreed plan. |
How progress of T2DM and impact of treatment will be monitored and who will be involved. | Ensure proposed follow-up plans are feasible and sustainable for the patient. Share HbA1c and other test results with the patient (with context of their management goals) prior to their next appointment if possible, encouraging them to think over the results and prepare for their review. |
Notepad: Patient-centred care and shared decision-making Patient-centred care provides care that is ‘respectful of and responsive to individual patient preferences, needs and values, and [ensures] that patient values guide all clinical decisions.’ 48 It also encourages active collaboration and shared decision-making between the patient, their family and the healthcare professional team.49 For patients with diabetes, patient-centred care can improve glycaemic control,50, 51 patient self management,51, 52 patient and healthcare professional satisfaction,6,50 and reduce healthcare costs.51 |
Recommendation 6: Educate patients with T2DM on sustained lifestyle intervention, medication adherence, and regular review.
Education regarding T2DM management should be specific and relevant to the patient. Examples of practice tips are provided below. Where helpful, reinforce verbal information with written information.
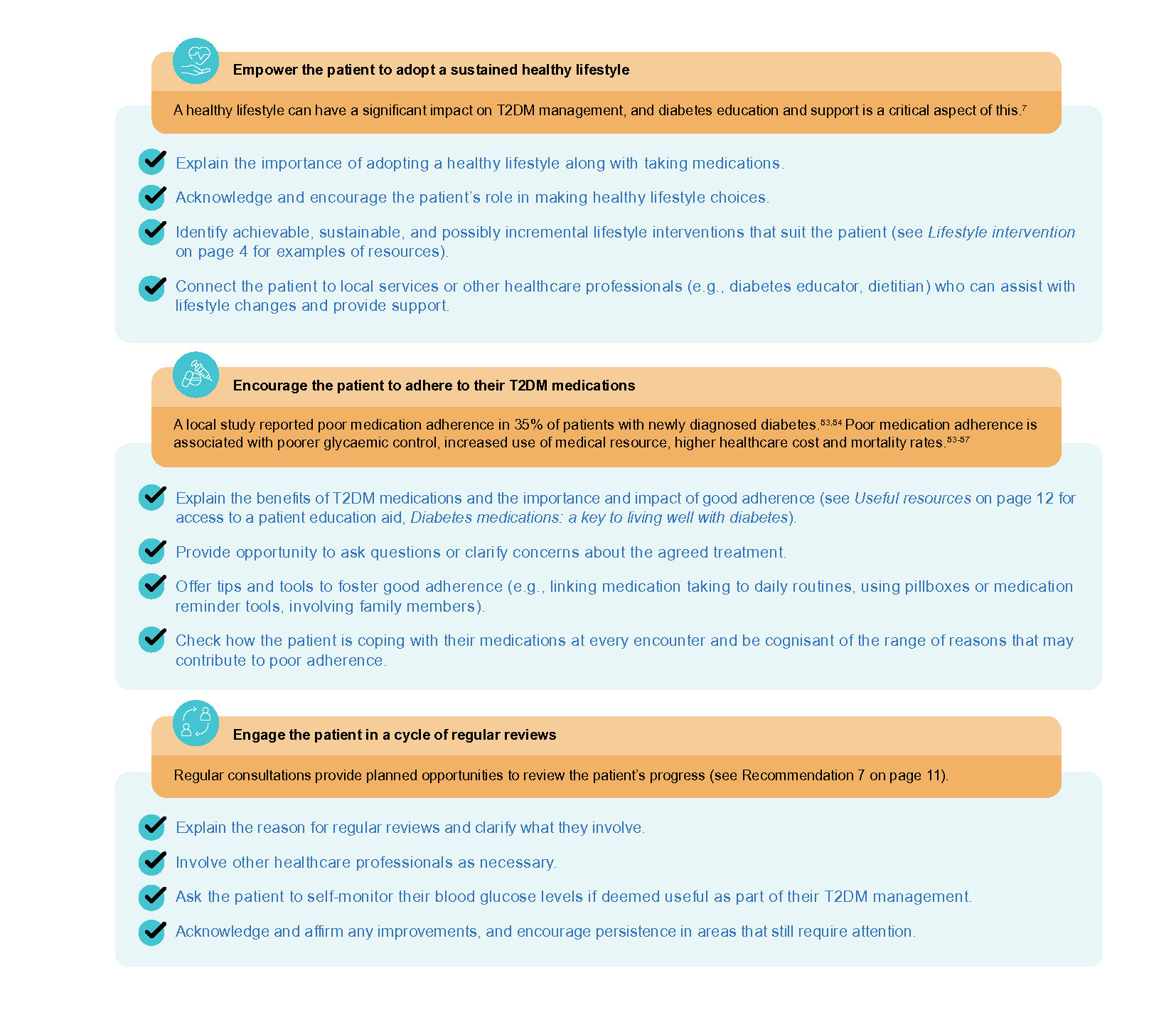
Notepad: Recognising poor adherence to diabetes medications in practice Poor medication adherence to diabetes medications may be associated with multiple factors, including:54,56,57
A well-executed, informal, open and non-judgmental conversation with a patient about how they are coping with their medications can be an effective and successful way of identifying issues with adherence. |
Monitoring and follow-up
Recommendation 7: Review all patients with T2DM regularly, including treatment response and complication screening.
Review parameters and frequency
Tailor the frequency of follow-up consultations. For example, review:
every six months if the patient is doing well and meeting their agreed treatment goals
every three months if the patient is not doing well or finding it challenging to achieve their treatment goals
earlier as required, e.g., when starting, adjusting or stopping a medication.
Review parameters include HbA1c, blood pressure, weight, BMI, lipid profile, kidney parameters (such as eGFR and urinary albumin:creatinine ratio), smoking, eye and foot assessments. Complication screening should be conducted at least annually (e.g., kidney, eye and foot assessments).
Local programs may provide useful resources and frameworks to facilitate regular reviews for patients with T2DM, such as the Chronic Disease Management Programme or Healthier SG Care Protocols.
Interdisciplinary care
Consider involving various healthcare professionals with complementary expertise to provide holistic care to the patient. For patients with diabetes, interdisciplinary care has been associated with improvements in patient outcomes (e.g., improved glycaemic control, reduction in blood pressure and lipid levels, improved quality of life) or processes of care (e.g., increased monitoring and complication screening).58,59 Importantly, interdisciplinary care must be coordinated (e.g., by the primary care clinician) to avoid confusion, duplication or gaps in care.
In addition to involving an interdisciplinary team in providing routine T2DM care, there may be times when involvement of an appropriate medical specialist is required, for example for:60
patients with difficulty achieving glycaemic control despite appropriate management
patients with or at risk of frequent hypoglycaemia, diabetic ketoacidosis, or hyperglycaemic hyperosmolar state, regardless of HbA1c levels
patients with diabetes complications requiring active specialist management, including:
Patients with foot ulceration, gangrene or severe foot infection (see ACG on Foot assessment in people with diabetes mellitus)
Patients with concomitant CKD stage 3b or higher, or with unexpected or rapid decline in renal function (see ACG on Chronic kidney disease – early detection)
Patients with diabetic macular oedema, severe non-proliferative diabetic retinopathy or unexplained drop in visual acuity/eye findings
Expert group
Chairperson
A/Prof Bee Yong Mong, Endocrinology (SGH)
Members
Dr Thofique Adamjee, Internal Medicine (KTPH)
Ms Debra Chan Shu Zhen, Pharmacy (TTSH)
Ms Chieng Ying Jia Shermin, Nursing (NUP)
Clin Prof Terrance Chua, Cardiology (National Heart Centre Singapore)
Dr Ajith Damodaran, Primary Care (Serangoon Garden Clinic)
A/Prof Goh Su-Yen, Endocrinology (SGH)
A/Prof Michelle Jong, Endocrinology (TTSH)
Dr Khoo Chin Meng, Endocrinology (NUH)
Dr Eric Khoo, Endocrinology (Gleneagles Medical Centre)
Dr Loke Kam Weng, Primary Care (Keat Hong Family Medicine Clinic)
Dr Alvin Ng Kok Heong, Nephrology (Mount Elizabeth Novena Hospital)
Dr Ng Huiwen Christine, Primary Care (NUP)
Dr Darren Seah Ee-Jin, Primary Care (NHGP)
Dr Gilbert Tan Choon Seng, Primary Care (SHP)
Dr Cheryl Tan Ying Lin, Pharmacy (SGH)
Dr Tham Tat Yean, Primary Care (Frontier Healthcare Group)
Prof Anantharaman Vathsala, Nephrology (NUH)
Dr Woo Jia Wei, Cardiology (Sunrise Heart and Internal Medicine Clinic)

Feedback
Click here to give us feedback on this ACG.
Related ACGs and Other related resources
Gestational diabetes mellitus — an update on screening, diagnosis, and follow-up
Initiating basal insulin in type 2 diabetes mellitus
Managing pre-diabetes — a growing health concern
Foot assessment in people with diabetes mellitus
T2DM Clinician Infographic and Medication Table [PDF, 2.6 MB] (updated 17 July 2024)
Subsidised non-insulin medications for T2DM [PDF, 149 KB]
Patient education aid [PDF, 463 KB]
Diabetic Retinal Photography (DRP) Screening Technical Reference Guide
Guide to Healthy Eating for Managing Diabetes Mellitus
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). Type 2 diabetes mellitus – personalising management with non-insulin medications. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2023. Available from: go.gov.sg/acg-t2dm-personalising-medications
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly or indirectly from any use of this ACG, which is provided as is, without warranties.