
When to order CT/MRI for headache ACG
Last updated 3 June 2026
Published on 31 Aug 2022
Last Updated on 31 Aug 2022
Overview
This ACE Clinical Guideline (ACG) covers the use of CT/MRI brain for diagnostic investigation of headache, providing evidence-based recommendations on the role of CT/MRI brain for primary and secondary headaches.
ACGs serve as the primary reference for clinical management in Singapore's healthcare system and can inform the standard of care (i.e. the treatment and level of care that is considered reasonable and appropriate by medical experts in respect of a given condition). Our guidelines, developed through rigorous evidence review and multi-disciplinary expert group inputs, may inform healthcare policy decisions and funding frameworks, and may have other system-wide implications.
ACG Recommendations
Patients with migraine or TTH, without red flags: CT is not indicated; MRI is not indicated.
Patients with cluster headache or other trigeminal autonomic cephalalgias, without red flags: CT may be indicated; MRI is indicated.
Patients with sudden, severe headache: CT is indicated; MRI may be indicated.
Patients with headache and cancer or infection (suspected or known): CT may be indicated; MRI is indicated.
Patients with post-traumatic headache: CT is indicated; MRI may be indicated.
Patients with new headache accompanied by red flags, or with worsening headache: CT may be indicated; MRI is indicated.
Download the ACG
When to order CT/MRI for headache (August 2022) [PDF, 1.2 MB]
Request for a hardcopy
Registered doctors, pharmacists and nurses may claim 1 Continuing Medical Education (CME)/Continuing Professional Education (CPE) point under category 3A/ category V-B for reading each ACG.
Statement of Intent
This ACE Clinical Guideline (ACG) provides concise, evidence-based recommendations and serves as a common starting point nationally for clinical decision-making. It is underpinned by a wide array of considerations contextualised to Singapore, based on best available evidence at the time of development. The ACG is not exhaustive of the subject matter and does not replace clinical judgement. The recommendations in the ACG are not mandatory, and the responsibility for making decisions appropriate to the circumstances of the individual patient remains at all times with the healthcare professional.
Introduction
Globally, headache* leads to the third highest number of years lived with disability (YLDs) after low back pain and depressive disorders, and the highest YLDs in people aged 15 to 49 years.1 Moreover, YLDs attributed to headache* have continued to rise over time.2 In Singapore, it is estimated that more than 80% of residents have experienced headache in their lifetime.3 Although computed tomography (CT) and magnetic resonance imaging (MRI) of the brain are increasingly available for investigation of headache, their clinical utility varies with the clinical presentation and working diagnosis.
*Defined as migraine or tension-type headache, and their complication of medication overuse headache.1
Overall approach to headache assessment
The assessment of headache begins with thorough history taking and physical examination to determine the likely diagnosis. Headaches that have an independent pathophysiology and are not caused by another condition are referred to as primary headaches.4 Primary headaches account for the majority of headaches, with migraine and tension-type headache (TTH) being the most common. The diagnosis of a primary headache is reached based on the patient’s clinical presentation, including an absence of features suggesting another cause.5 When any of such features is present (they are often known as red flags), a secondary headache may be more likely and investigations are usually indicated─including CT/MRI brain (see section “CT/MRI for secondary headaches” starting on page 3).6
The focus of this clinical guidance is on the role of CT/MRI brain for further evaluation of headache to confirm the diagnosis. When ordering CT/MRI brain, consider consulting with radiology on details including specific sequences, contrast agents, and complementary examinations (such as CT/MR angiography/venography).6
CT/MRI for primary headaches
Recommendation 1: Patients with migraine or TTH, without red flags: CT is not indicated; MRI is not indicated.
Migraine typically presents as moderate to severe, unilateral pulsating headache that may be preceded by or occurring concurrently with a visual or sensory disturbance referred to as aura. Other accompanying features can include nausea or vomiting, sensitivity to light or sound, and exacerbation of headache with normal daily activities.4 TTH is typically characterised by mild to moderate, bilateral non-pulsatile pain that develops gradually, often described as pressure or tightness.4
CT/MRI brain is generally not indicated for patients with typical migraine (even in the presence of aura) or TTH, because the chance of detecting a significant abnormality is low and similar to that of people without a headache (regardless of whether the migraine or TTH is acute or chronic).6,7
Notepad: When to reconsider the diagnosis of migraine or TTH When migraine or TTH does not improve despite appropriate management─including lifestyle changes, and acute or prophylactic pharmacological treatment─the diagnosis may need to be revisited (how soon improvement is expected differs depending on the management strategy).8 Consider reassessing the patient for an alternative diagnosis at this point, including the need for referral or investigations, such as CT/MRI brain. |
Recommendation 2: Patients with cluster headache or other trigeminal autonomic cephalalgias, without red flags: CT may be indicated; MRI is indicated.
Trigeminal autonomic cephalalgias (TACs) are characterised by headache with autonomic symptoms or signs on the same side (for example, conjunctival injection, watery eye, nasal obstruction/discharge, or ptosis).4 Cluster headache is the most well-known type of TACs. For patients with TAC-like presentation, it is recommended to do CT/MRI brain at least once, especially if it has not been done before. This is because symptoms or signs similar to those seen in TACs could be caused by an intracranial lesion (for example, of the pituitary gland).6 Although only affecting a small number of patients, an intracranial lesion needs to be excluded through CT/MRI brain, as it cannot be differentiated from TACs clinically. MRI is preferred over CT as it is better for detecting intracranial lesions.
CT/MRI for secondary headaches
Less common than primary headaches, secondary headaches are the symptom of another condition or pathology, such as subarachnoid haemorrhage or brain tumour.9 One should suspect a secondary headache when the patient presents with associated features (red flags).
The presence of red flags increases the likelihood of a secondary headache (particularly when two or more are present that suggest the same underlying condition or pathology) and usually lowers the threshold for ordering investigations, including CT/MRI brain. However, most red flags are not highly specific to secondary headaches and clinical judgement should still be exercised in deciding whether to proceed with investigations when red flags are present. Also, not all red flags carry the same significance for investigations, for example painkiller overuse on its own may not warrant imaging, but suggests possible medication overuse headache. Referral to a relevant specialist could be considered at any point, as appropriate.
There are multiple red flags for secondary headaches. See Table 1 below for the internationally accepted systematic SNNOOP10 list of red flags for secondary headaches.5
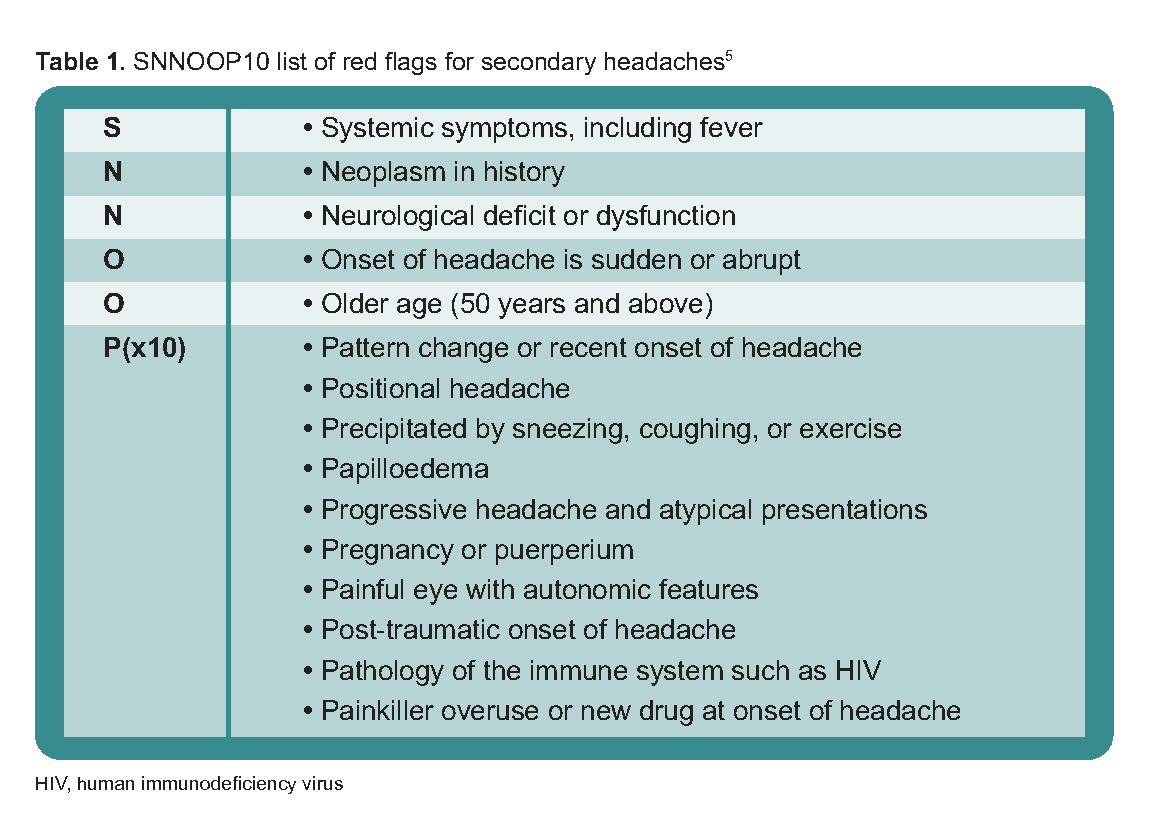
Table 1. SNNOOP 10 list of red flags for secondary headaches
On balance, investigations are usually indicated when headache is accompanied by red flags. Recommendations 3 to 6 pertain to the more common clinical scenarios involving red flags, in which CT/MRI brain is warranted. The decision to order CT/MRI brain, refer to a specialist, or follow up with the patient should be made in light of individual patient circumstances─including those involving red flags that are not specifically mentioned in the following recommendations.
Notepad: Choosing between CT and MRI Considerations informing the choice between CT and MRI include clinical presentation, contraindications, diagnostic accuracy, and availability of the test. Overall, CT is preferred over MRI in urgent situations (for example, emergencies or headache with rapid progression), and to exclude intracranial haemorrhage. MRI does not carry radiation risk and it provides more detailed investigation of suspected intracranial lesions. |
Recommendation 3: Patients with sudden, severe headache: CT is indicated; MRI may be indicated.
Patients with thunderclap headache (TCH), defined as severe headache of sudden onset that reaches maximum intensity within a minute,4 require urgent CT brain to investigate suspected intracranial bleeding, particularly subarachnoid haemorrhage (SAH). MRI brain or other investigations may be indicated if CT is negative (especially when CT was done more than six hours after headache onset), to look for SAH or other causes of TCH.10
Recommendation 4: Patients with headache and cancer or infection (suspected or known): CT may be indicated; MRI is indicated.
Suspicion for brain cancer or central nervous system infection should be higher when a patient presents with associated features, including systemic symptoms or signs (such as fever, chills, night sweat, myalgia, or weight loss), history of cancer, and immunosuppression. CT/MRI brain is recommended for these patients, especially if they are aged 50 years and older and the headache is new.
Recommendation 5: Patients with post-traumatic headache: CT is indicated; MRI may be indicated.
A headache occurring after a traumatic injury to the head warrants investigation with CT/MRI brain. CT brain is indicated for patients with a headache developing within seven days after the traumatic event.4 In addition to its accuracy for evaluating bony structures and excluding intracranial haemorrhage, CT is easier to perform than MRI on patients who are on ventilator support, in traction, or agitated. MRI brain may be considered when neurological deficits are present and not explained by CT brain findings.11
Recommendation 6: Patients with new headache accompanied by red flags, or with worsening headache: CT may be indicated; MRI is indicated.
In addition to Recommendations 3 to 5, a new headache with red flags (see Table 1 on page 3) or an existing headache that is worsening (including development of new features and headache not improving with appropriate management) warrant CT/MRI brain to investigate the underlying cause. This also applies to primary headaches accompanied by red flags or that are worsening over time (for example, TTH with neurological deficit, new migraine in a pregnant woman, or worsening of TTH or migraine─such as increasing frequency/intensity or development of aura).
Notepad: Headache and sinusitis While headache (especially migraine and TACs) and sinusitis could manifest similar symptoms (such as head or face pressure/pain, nasal obstruction/discharge, or change in olfaction), sinusitis is usually accompanied by features of infection, including fever and purulent nasal discharge. Consider referral to an ear, nose and throat specialist for further evaluation (including the need for imaging), especially if symptoms persist or progress despite appropriate management, or if complications are suspected (such as orbital or intracranial spread of infection).12 |
Expert group
Chairperson
Dr Bernard Chan Poon Lap, Neurology (NUH)
Members
A/Prof Francis Lee Chun Yue, Emergency Medicine (KTPH)
Dr Vincent Ng Yew Poh, Neurosurgery (NNI)
A/Prof David Loke Kok Teik, Ear, Nose & Throat (KTPH)
Prof Lim Choie Cheio Tchoyoson, Neuroradiology (NNI)
Dr Yasmin Idu Jion, Neurology (NNI)
Clin Asst Prof Gilbert Tan Choon Seng, Family Medicine (SHP)
Project lead
Adj A/Prof Tan Cher Heng, Diagnostic Radiology (TTSH)
Feedback
Click here to give us feedback on this ACG.
© Agency for Care Effectiveness, Ministry of Health, Republic of Singapore
All rights reserved. Reproduction of this publication in whole or in part in any material form is prohibited without the prior written permission of the copyright holder. Application to reproduce any part of this publication should be addressed to: ACE_HTA@moh.gov.sg
Suggested citation:
Agency for Care Effectiveness (ACE). When to order CT/MRI for headache. ACE Clinical Guidance (ACG), Ministry of Health, Singapore. 2022. Available from: go.gov.sg/acg-when-to-order-ct-mri-for-headache
The Ministry of Health, Singapore disclaims any and all liability to any party for any direct, indirect, implied, punitive or other consequential damages arising directly orindirectly from any use of this ACG, which is provided as is, without warranties.